---
title: "Abnormal Shape/Configuration of Corpus Callosum"
docid: "238ca32d-6bc6-4f5a-81b1-6601dd605856"
authors:
- key: "47381de4-c9fd-4999-8dd0-1808cd72db6b"
value: "Luke L. Linscott, MD"
breadcrumbs:
-
name: "Pediatrics"
slug: "pediatrics"
treeNodeId: "a915965c-d436-44cf-ae65-2f22e7246ea4"
-
name: "Differential Diagnosis"
slug: "differential-diagnosis"
treeNodeId: "9e45b379-de58-40ea-b8b0-9877f7ebe994"
-
name: "Brain"
slug: "brain"
treeNodeId: "0ad2e6d5-5dc7-4db0-a2f9-de0cf62fd0de"
-
name: "Abnormal Shape/Configuration of Corpus Callosum"
slug: "abnormal-shapeconfiguration-of-cor-"
treeNodeId: null
category: "Pediatrics"
documentVersionId: "bea8db40-78a1-4745-a1f7-c18bbf5f3f30"
imageCount: 53
lastUpdated: "08/16/19"
pageDescription: "Abnormal Shape/Configuration of Corpus Callosum"
pageKeywords: "Pediatrics, Differential Diagnosis, Brain, Abnormal Shape/Configuration of Corpus Callosum"
pageTitle: "Abnormal Shape/Configuration of Corpus Callosum | STATdx"
enhancedTitle: "Abnormal Shape/Configuration of Corpus Callosum"
type: "DDX"
references: true
breadcrumbs:
- "Pediatrics"
- "Differential Diagnosis"
- "Brain"
- "Abnormal Shape/Configuration of Corpus Callosum"
---
# ESSENTIAL INFORMATION
- ## Key Differential Diagnosis Issues
- Clinical features to consider
- Normal corpus callosum (CC) varies in thickness & shape
- Associated anomalies portend worse prognosis
- If not congenital anomaly, clinical history is crucial
- Prior surgical history, prematurity etc.
- Corpus callosotomy, shunt placement, endoscopic 3rd ventriculostomy
- Imaging features to consider
- Isolated callosal dysgenesis is not common → additional malformations in > 50%
- Malformations of cortical development
- Noncallosal midline anomalies
- Abnormal brainstem or cerebellum
- Look for parenchymal abnormalities to identify etiology
- White matter (WM) volume loss, prior infarction, diffuse axonal injury
- Ventricular abnormalities are common
- Colpocephaly → CC agenesis/dysgenesis, Chiari 2
- Enlarged, angular ventricles → periventricular leukomalacia
- Modality considerations
- CT: Helpful to distinguish cellular vs. inflammatory
- ↑ density → cellular mass, hemorrhage
- ↓ density → edema, inflammation
- MR: Best spatial & contrast resolution
- Sagittal imaging is critical for evaluation of CC
- 3D acquisitions allow multiplanar reconstructions
- ## Helpful Clues for Common Diagnoses
- **Normal Variant**
- Immature CC is thin
- Gradually thickens with progressive myelination
- Size, shape, & thickness of normal CC vary
- Splenium & genu are largest parts of CC
- Normal narrowing at junction of body & splenium ("isthmus")
- Dorsal surface of fully developed, normally myelinated CC is often "wavy"
- **Thin Corpus Callosum**
- Many causes (congenital, acquired)
- All may result in focal or diffuse callosal thinning
- **Periventricular leukomalacia**
- Premature infant is at greatest risk
- Acute findings: US → ↑ periventricular WM echogenicity
- MR: Diffusion restriction, ↑ T1, ↓ T2
- Subacute findings: Cavitation, periventricular cysts
- Chronic findings: ↓ volume of periventricular WM
- Thin posterior body & splenium are most common
- Ventricular enlargement shows angular margins
- **Hypoxic-ischemic encephalopathy**
- Loss of cerebral WM → thin CC
- May occur with profound or partial prolonged injury
- Profound: Often perirolandic → posterior body CC
- Partial prolonged: Watershed injury → entire CC
- **Chronic cerebral infarction**
- Axonal loss → focal/diffuse thinning of CC
- **Obstructive hydrocephalus**
- Look for obstructing lesion (e.g., tumor, aqueductal stenosis) or sequelae of prior hemorrhage/infection
- Acute: CC stretched, bowed upward
- Chronic: Thinned, irregular (sequela of CC impingement against falx & chronic WM injury from hydrocephalus)
- **Chemotherapy & radiation therapy**
- WM injury with volume loss
- e.g., chronic methotrexate toxicity
- **Postsurgical Defects**
- **Corpus c****allosotomy**
- Surgical disruption for intractable epilepsy
- Isolated callosotomy or part of functional hemispherotomy
- Often imaged in postoperative setting to detect residual neuronal connections across midline
- Best seen on sagittal or coronal MR
- **Ventricular drainage catheter tract**
- Small defect in paramidline CC
- Typically with overlying WM parenchymal tract & postoperative skull focus
- May see hypointense intracranial catheter ± hyperintense fluid-filled extracranial components
- **Endoscopic 3rd ventriculostomy**
- Small defect in CC represents scope tract, typically with overlying WM parenchymal tract & postoperative skull focus
- ## Helpful Clues for Less Common Diagnoses
- **Callosal Agenesis**
- Absent WM bridging cerebral hemispheres
- Absent septum pellucidum
- Absent cingulate gyrus with vertically oriented parasagittal sulci radiating to high-riding 3rd ventricle
- Lateral ventricles: Colpocephaly, upturned frontal horns
- Probst bundles (WM tracts that would have formed CC) lie along medial aspects of lateral ventricles
- **Primary Callosal Dysgenesis**
- Absence of 1 or all segments
- Rostrum & splenium are most likely to be deficient
- Remnants vary in size, shape, configuration
- Look for other associated malformations
- "Micro" CC: Small but well formed, often syndromic
- "Mega" CC: Megalencephalic (bulky WM) vs. small to normal brain (syndromic)
- **Chiari 2 Malformation**
- Constellation of intracranial findings secondary to open neural tube defect (e.g., myelomeningocele)
- Small posterior fossa, towering cerebellum that wraps around dorsal brainstem, small elongated 4th ventricle, vermian/tonsillar extension into upper cervical spine, "beaked" tectum, scalloped clivus
- Degree of callosal dysgenesis is highly variable
- Correlates with severity of hydrocephalus
- **Neoplasm**
- **Glioblastoma**
- Common in adults, uncommon in children
- "Butterfly" glioma crosses CC
- Central necrosis + thick, irregular rim enhancement
- **Lymphoma**
- NECT: Hyperdense
- Strong, uniform enhancement
- **Pericallosal Lipoma**
- 40-50% occur in interhemispheric fissure
- Almost always located in subarachnoid space; blood vessels & cranial nerves course through lipoma
- 2 morphologic types
- Bulky, mass-like ("tubulonodular" type)
- Thin, dorsal to body/splenium ("curvilinear" type)
- Midline lipomas may be part of more general midline developmental disorder; CC is often deficient
- **Neurofibromatosis Type 1 (NF1)**
- Patients with NF1 have ↑ CC volume
- Sometimes markedly so & qualitatively evident
- Nonenhancing lesions of NF1 can occur in CC
- If focal lesions of CC enhance, suggest low-grade tumor
- **Holoprosencephaly**
- Alobar
- CC absent
- "Pancake" anterior cerebral tissue
- Monoventricle with large dorsal "cyst"
- Semilobar
- Frontal lobe fusion/hypoplasia; caudate head fusion
- Splenium may be present
- Lobar
- Genu sometimes present; GM often crosses with genu
- Absent anterior midline falx & fissure
- Middle interhemispheric variant (a.k.a. syntelencephaly)
- Splenium & genu present, body deficient
- Middle CC body "dips"
- GM crosses midline in expected location of CC body
- ± bilateral perisylvian polymicrogyria
- ## Helpful Clues for Rare Diagnoses
- **Hypomyelination**
- Primary pathologic hypomyelination is rare
- e.g., Pelizaeus-Merzbacher, *TUBB4A* disorders
- **Inherited Metabolic Leukodystrophies**
- **Metachromatic leukodystrophy**
- Entire CC affected, genu & splenium worst
- **X-linked adrenoleukodystrophy**
- Most commonly involves splenium
- **Alexander disease**
- Frontal lobe & genu involvement
- **Krabbe disease**
- Central WM + deep gray nuclei (especially thalamus)
## References
# Selected References
1. [Al-Hashim AH et al: Corpus callosum abnormalities: neuroradiological and clinical correlations. Dev Med Child Neurol. 58(5):475-84, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=26661037%5Bpmid%5D)
1. [Edwards TJ et al: Clinical, genetic and imaging findings identify new causes for corpus callosum development syndromes. Brain. 137(Pt 6):1579-1613, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24477430%5Bpmid%5D)
1. [Battal B et al: Corpus callosum: normal imaging appearance, variants and pathologic conditions. J Med Imaging Radiat Oncol. 54(6):541-9, 2010](http://www.ncbi.nlm.nih.gov/pubmed/?term=21199431%5Bpmid%5D)
1. [Bourekas EC et al: Lesions of the corpus callosum: MR imaging and differential considerations in adults and children. AJR Am J Roentgenol. 179(1):251-7, 2002](http://www.ncbi.nlm.nih.gov/pubmed/?term=12076946%5Bpmid%5D)
## Images
### Selected Images
 . The CC will gradually thicken as it myelinates from posterior to anterior. Note that the entire pituitary gland normally shows T1 shortening
. The CC will gradually thicken as it myelinates from posterior to anterior. Note that the entire pituitary gland normally shows T1 shortening  in the 1st few weeks of life.](images/app.statdx.com_image_thumbnail_770c0ebd-7c6f-4197-a62b-704c6b7d6bb6_annotated_true_size_900_quality_90_56dafce6_20251018T142218Z.jpg)
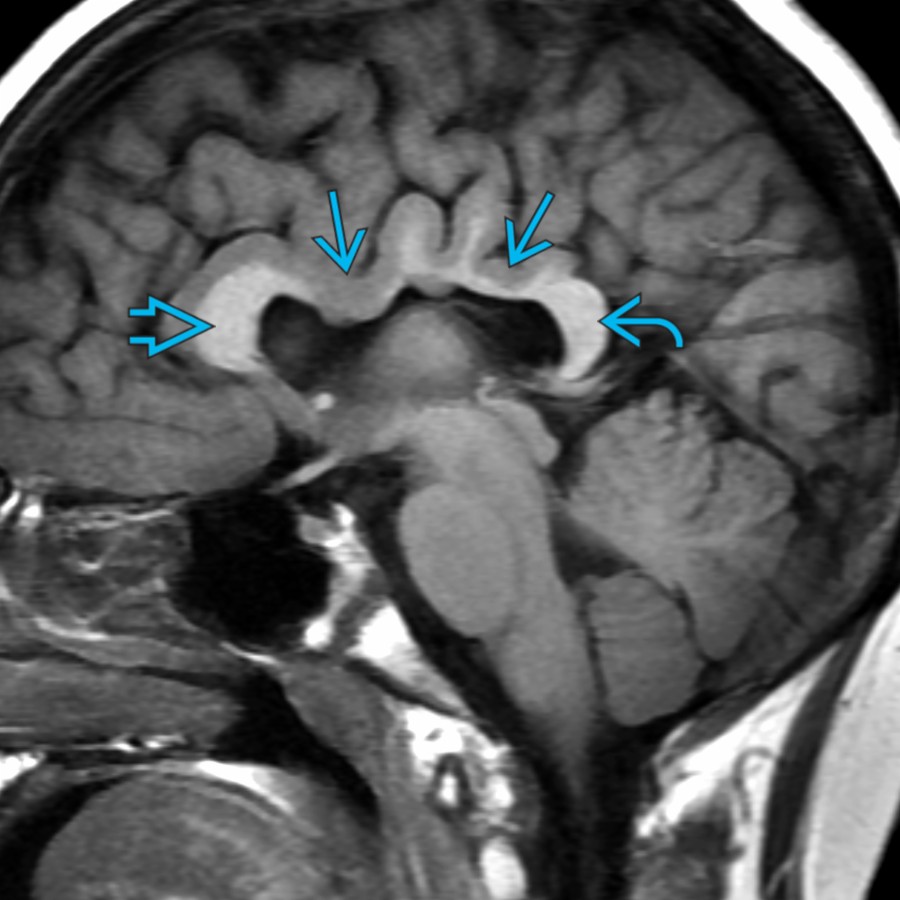
**Normal Variant**
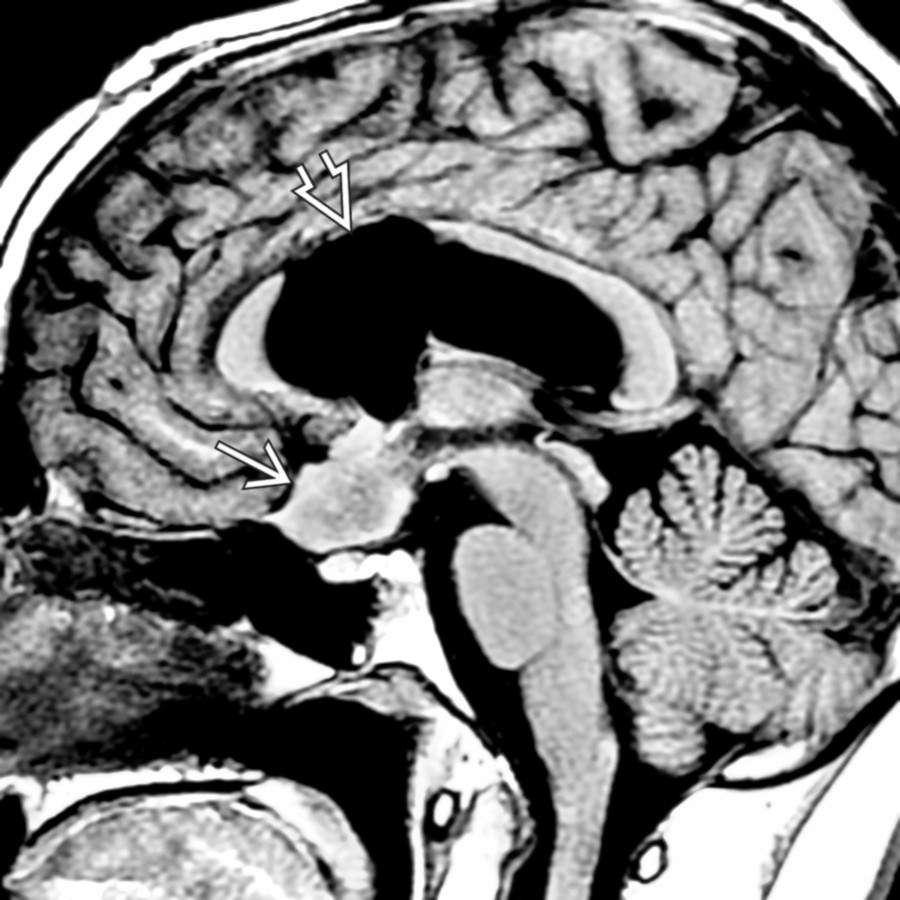
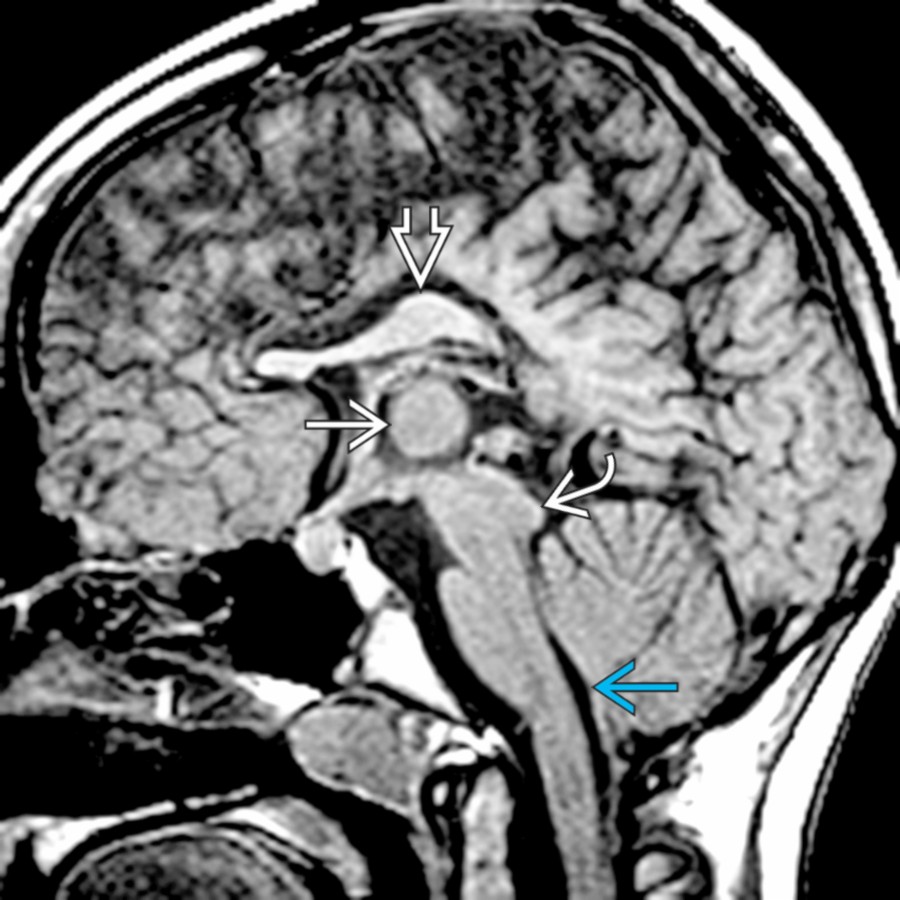
*Midline sagittal T1 MR in a normal term neonate shows a thin, unmyelinated corpus callosum (CC) . The CC will gradually thicken as it myelinates from posterior to anterior. Note that the entire pituitary gland normally shows T1 shortening in the 1st few weeks of life.*
**Normal Variant**
*Midline sagittal T1 MR in a normal term neonate shows a thin, unmyelinated corpus callosum (CC) . The CC will gradually thicken as it myelinates from posterior to anterior. Note that the entire pituitary gland normally shows T1 shortening in the 1st few weeks of life.*

**Normal Variant**
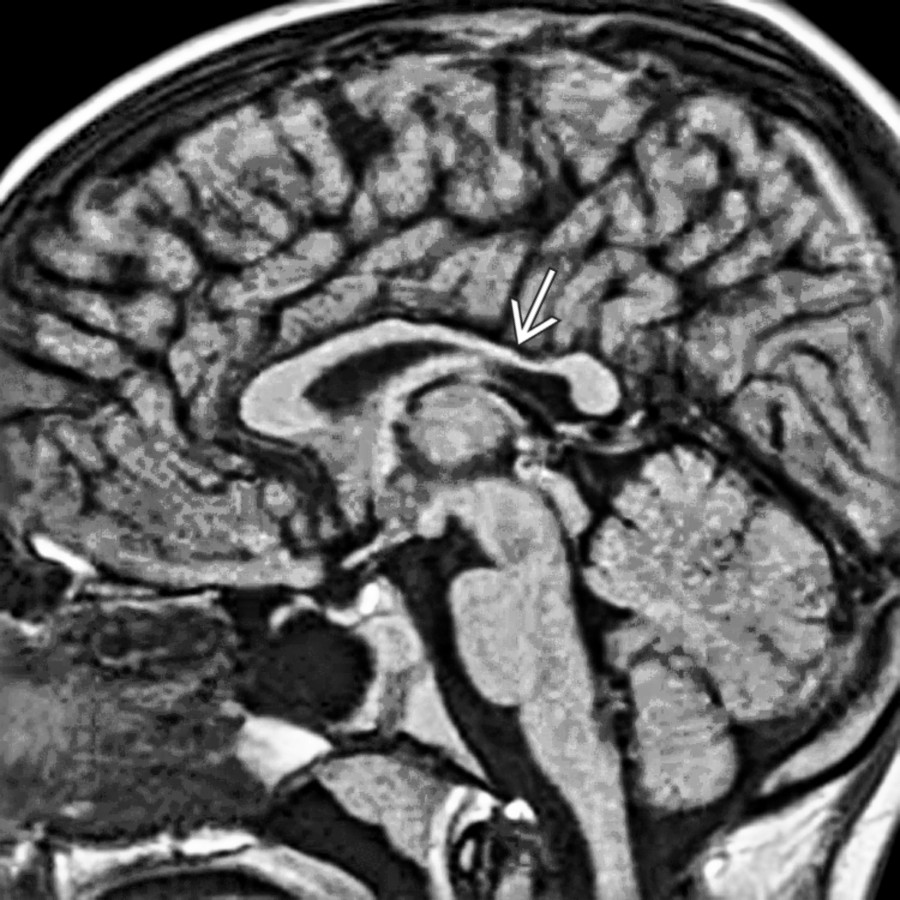
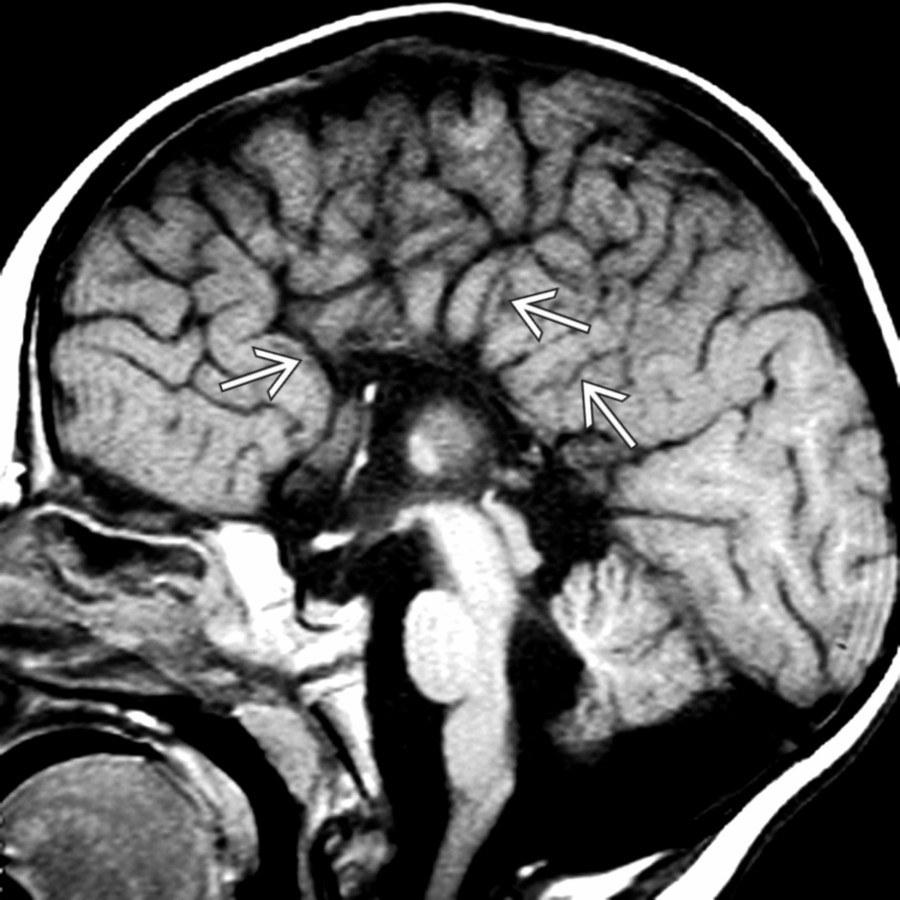
*Midline sagittal T1 MR in a 13 year old with headaches shows a normal variant morphology of the CC with relative thinning of the posterior body . This should not be mistaken for a sign of white matter (WM) volume loss.*
**Normal Variant**
*Midline sagittal T1 MR in a normal term neonate shows a thin, unmyelinated corpus callosum (CC) . The CC will gradually thicken as it myelinates from posterior to anterior. Note that the entire pituitary gland normally shows T1 shortening in the 1st few weeks of life.*

**Normal Variant**
*Midline sagittal T1 MR in a normal term neonate shows a thin, unmyelinated corpus callosum (CC) . The CC will gradually thicken as it myelinates from posterior to anterior. Note that the entire pituitary gland normally shows T1 shortening in the 1st few weeks of life.*

**Normal Variant**
*Midline sagittal T1 MR in a 13 year old with headaches shows a normal variant morphology of the CC with relative thinning of the posterior body . This should not be mistaken for a sign of white matter (WM) volume loss.*
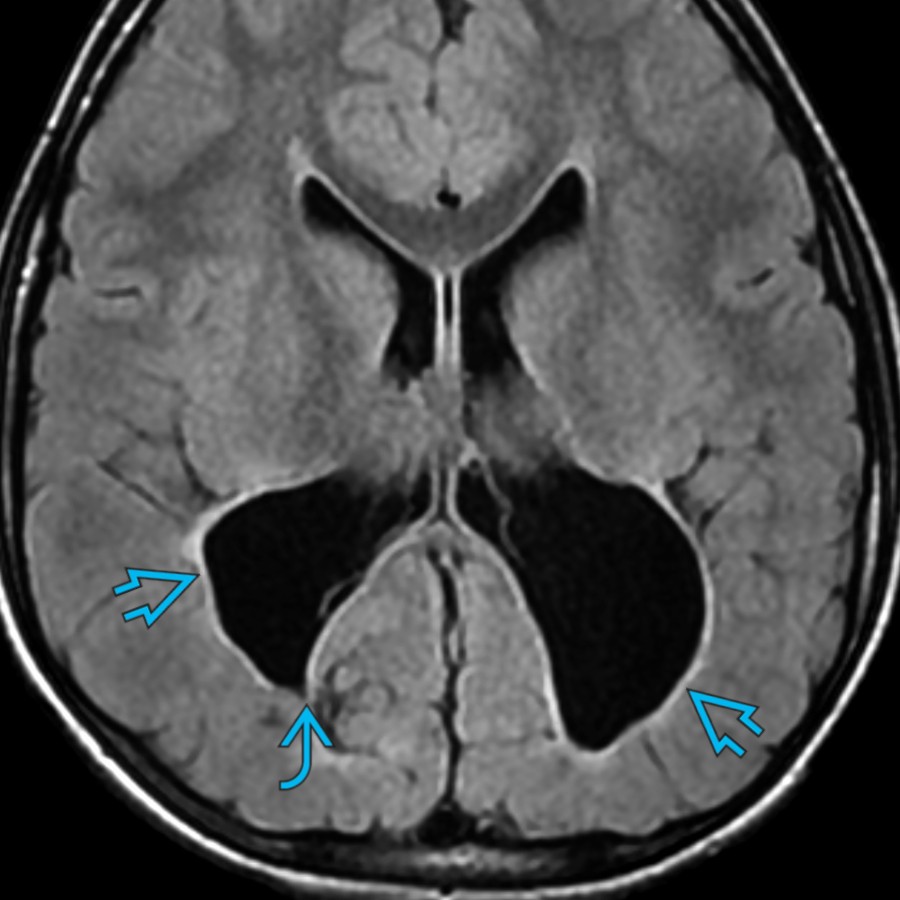
 of the expanded ventricular occipital horns, consistent with PVL related to extreme prematurity.](images/app.statdx.com_image_thumbnail_fdffb43b-acf7-4645-ae14-03f4bc8c461c_annotated_true_size_900_quality_90_a9dd954a_20251018T142218Z.jpg)
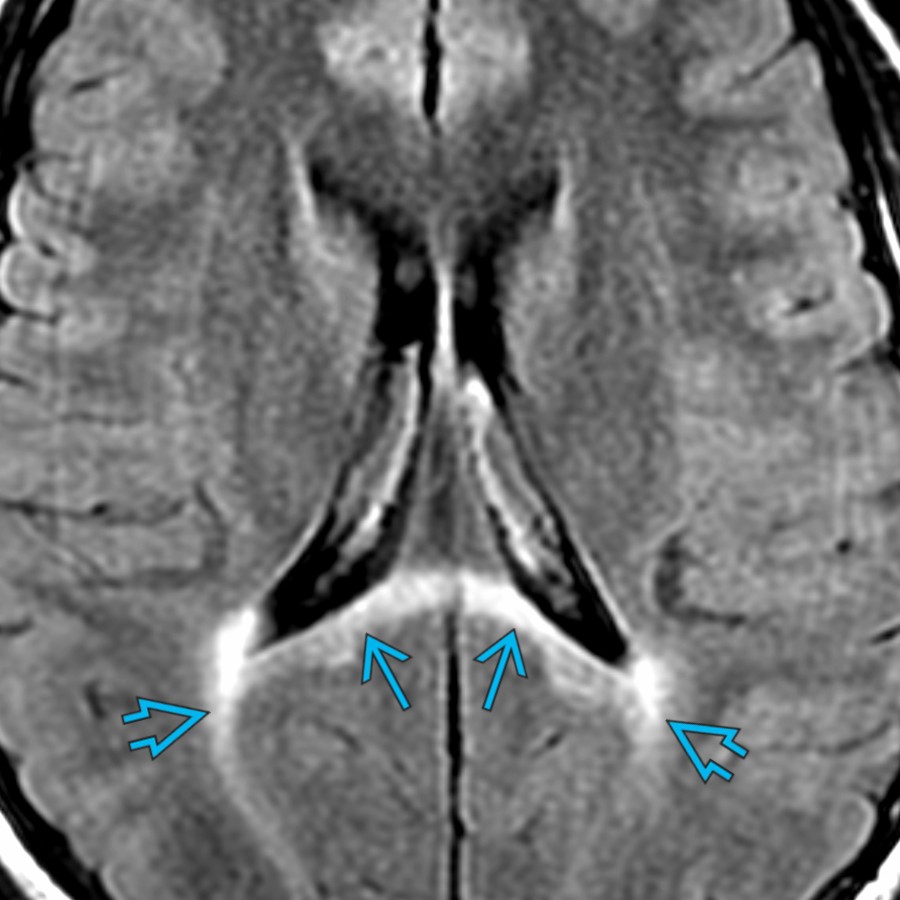
**Periventricular Leukomalacia**
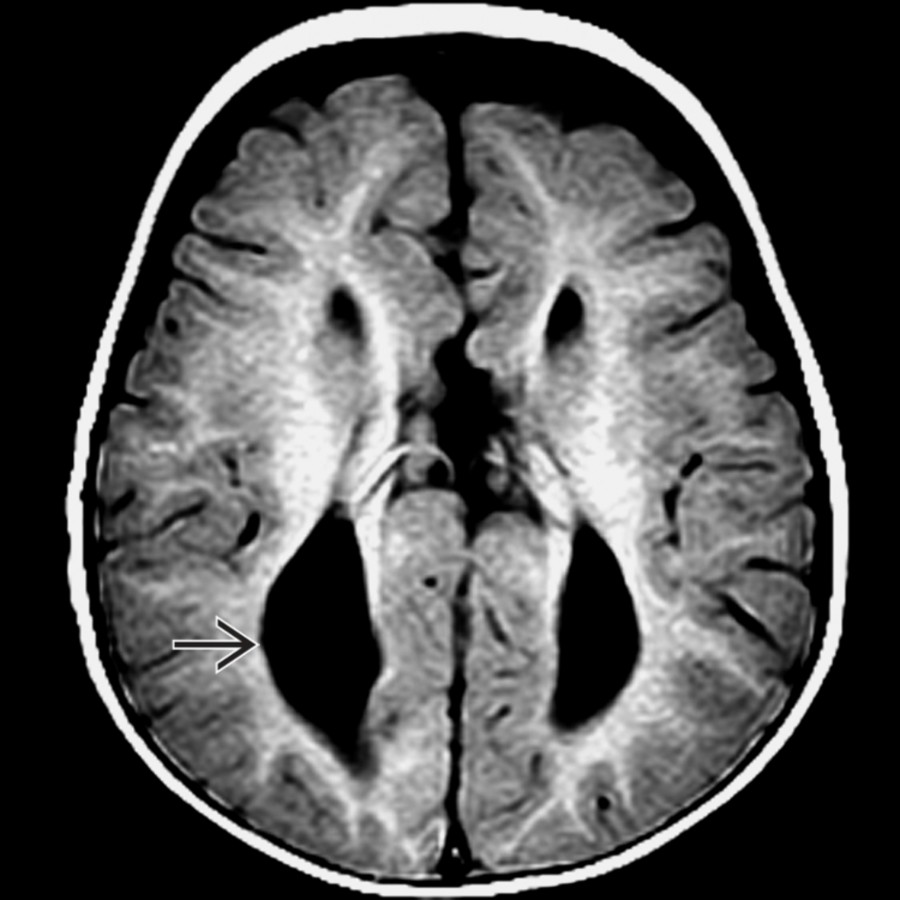
*Axial FLAIR MR in a 7 year old with a history of prematurity & periventricular leukomalacia (PVL) shows severe WM volume loss with relatively little signal abnormality. Also note the angular margins of the expanded ventricular occipital horns, consistent with PVL related to extreme prematurity.*
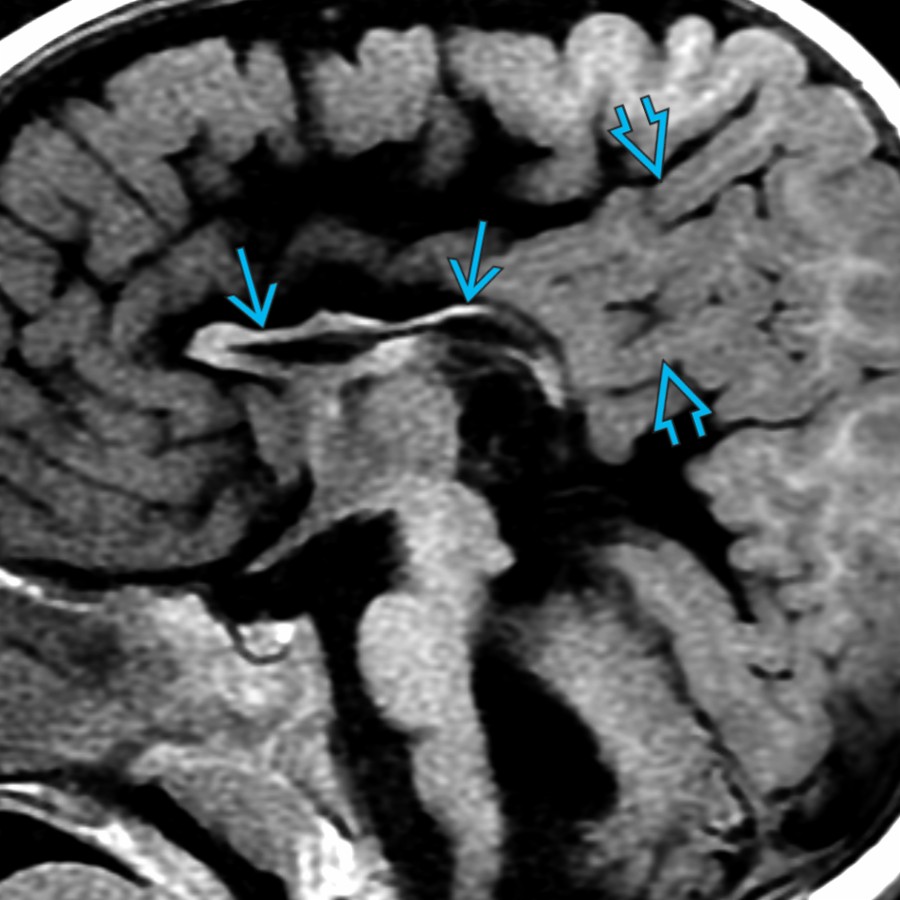
**Periventricular Leukomalacia**
*Midline sagittal T1 MR in the same patient shows marked thinning of the posterior body & splenium of the CC due to WM volume loss. This is the most common area of CC involvement in PVL.*

**Hypoxic-Ischemic Encephalopathy**
*Axial T2 MR in a 9 year old with a history of hypoxic-ischemic encephalopathy (HIE) at birth shows extensive gliosis & encephalomalacia causing WM volume & signal abnormality in a watershed distribution . This results in marked CC thinning.*
**Hypoxic-Ischemic Encephalopathy**
*Midline sagittal T1 MR in the same patient shows marked thinning of the CC secondary to WM loss as a consequence of the remote HIE injury.*
**Periventricular Leukomalacia**
*Axial FLAIR MR in a 7 year old with a history of prematurity & periventricular leukomalacia (PVL) shows severe WM volume loss with relatively little signal abnormality. Also note the angular margins of the expanded ventricular occipital horns, consistent with PVL related to extreme prematurity.*

**Periventricular Leukomalacia**
*Midline sagittal T1 MR in the same patient shows marked thinning of the posterior body & splenium of the CC due to WM volume loss. This is the most common area of CC involvement in PVL.*

**Hypoxic-Ischemic Encephalopathy**
*Axial T2 MR in a 9 year old with a history of hypoxic-ischemic encephalopathy (HIE) at birth shows extensive gliosis & encephalomalacia causing WM volume & signal abnormality in a watershed distribution . This results in marked CC thinning.*

**Hypoxic-Ischemic Encephalopathy**
*Midline sagittal T1 MR in the same patient shows marked thinning of the CC secondary to WM loss as a consequence of the remote HIE injury.*
 , & 4th
, & 4th  ventricles as well as thin T2 hypointensity along the brainstem, consistent with hemosiderin deposition.](images/app.statdx.com_image_thumbnail_a124c2db-747c-4ab8-885e-95a07831790d_annotated_true_size_900_quality_90_967e57cd_20251018T142240Z.jpg)
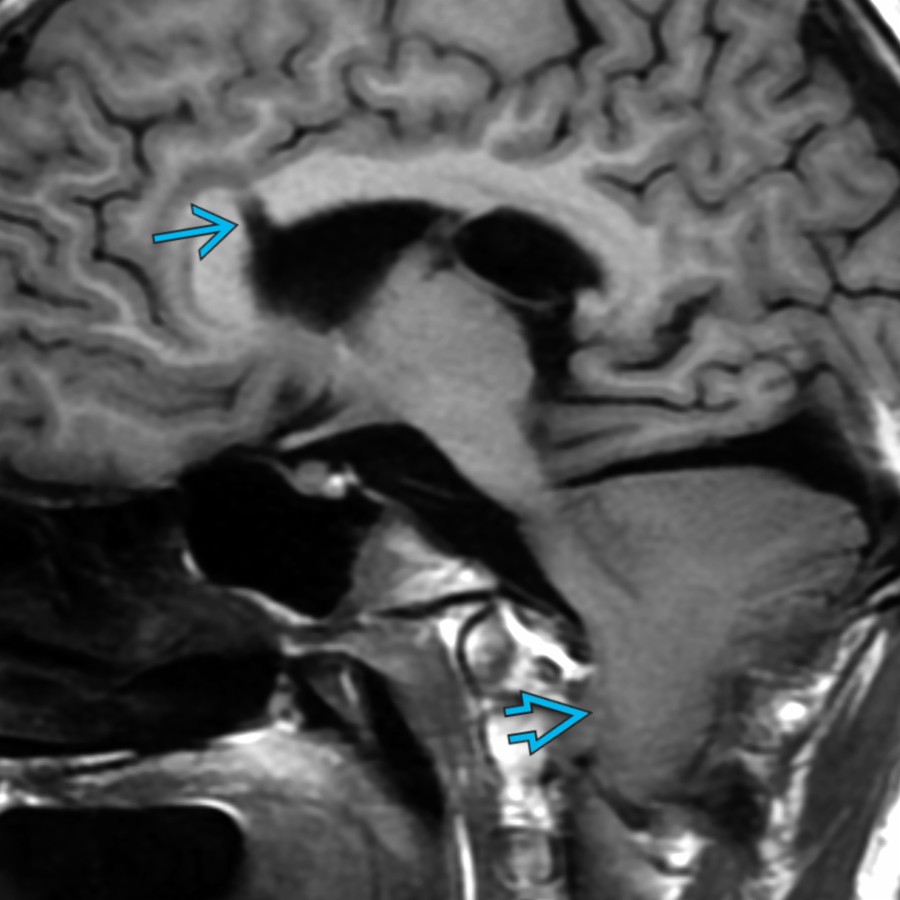
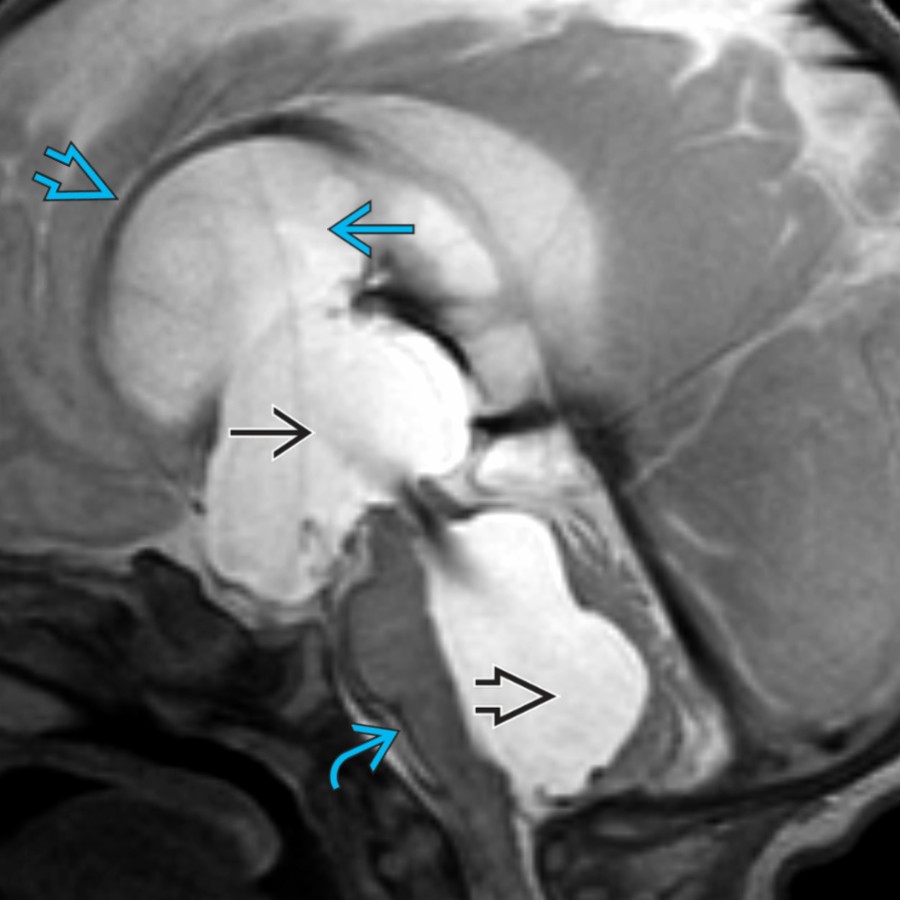
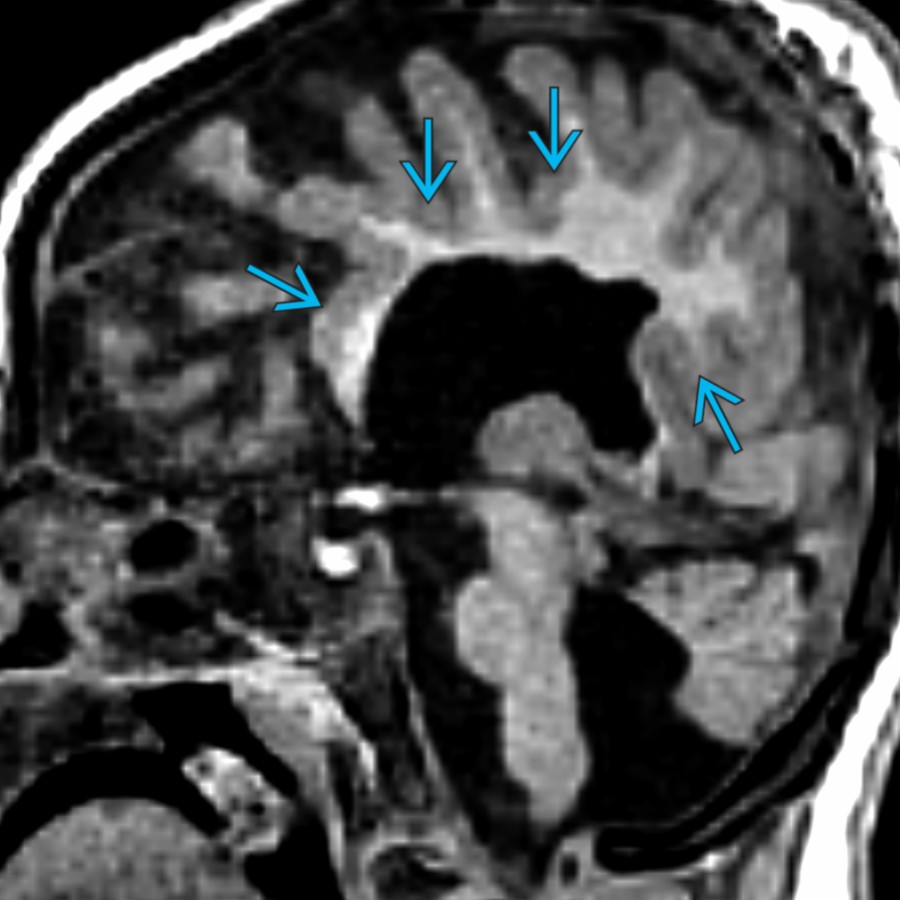
**Obstructive Hydrocephalus**
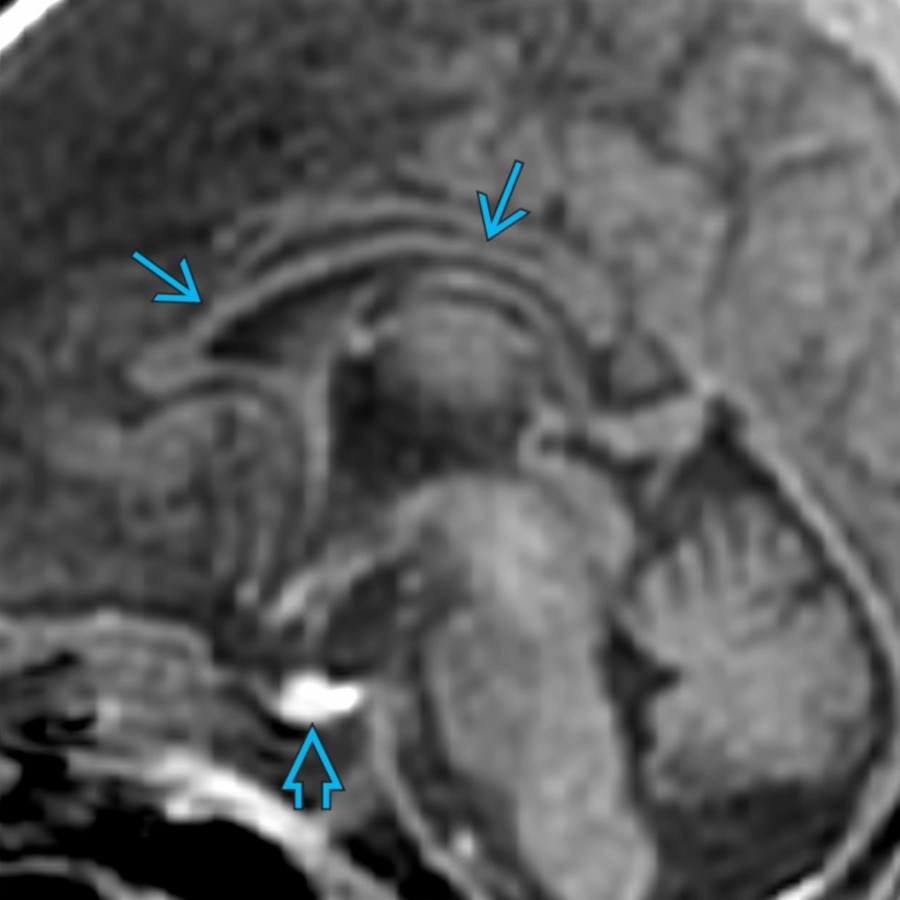
*Midline sagittal T2 MR in a neonate with posthemorrhagic hydrocephalus shows a stretched & thinned CC . Note the enlarged lateral , 3rd , & 4th ventricles as well as thin T2 hypointensity along the brainstem, consistent with hemosiderin deposition.*
**Obstructive Hydrocephalus**
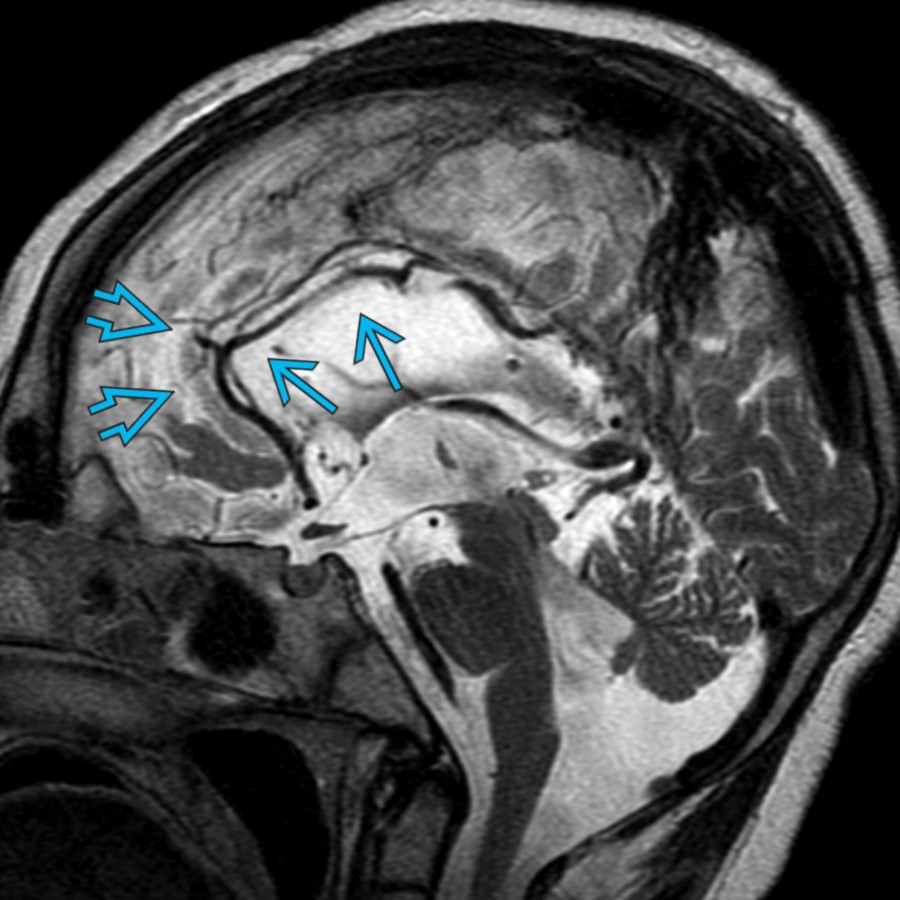
*Midline sagittal T1 MR in the same patient 1 year after shunting shows a thinned & dysmorphic CC as well as numerous thin, pencil-like gyri (stenogyria) .*
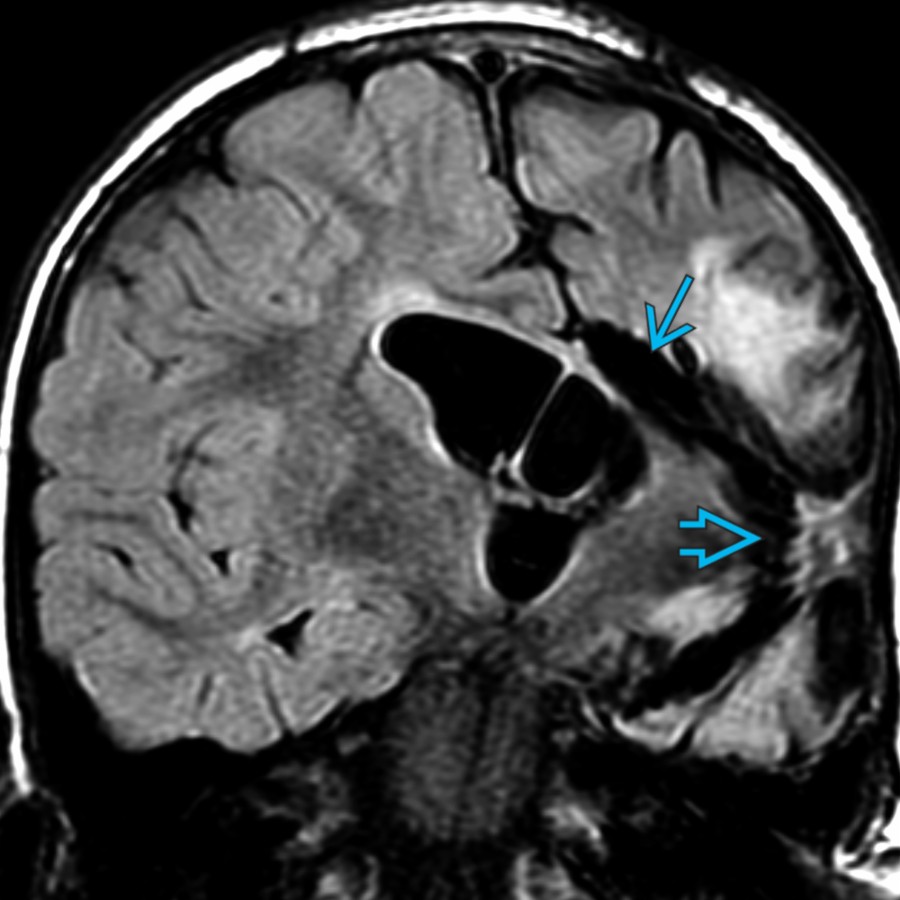
**Corpus Callosotomy**
*Coronal FLAIR MR shows changes of a left functional hemispherotomy with a WM disconnection & insular decortication . Corpus callosotomy may be performed in isolation or as part of a more extensive functional hemispherotomy, as in this patient.*
**Corpus Callosotomy**
*Coronal T2 MR shows absence of the midline CC with persistent paramidline callosal tissue , consistent with an isolated surgical callosotomy.*
**Ventricular Drainage Catheter Tract**
*Paramidline sagittal T1 MR in a 12 year old with Chiari 2 malformation shows a ventricular shunt catheter tract in the anterior body of the CC. Note the caudal migration of the cerebellum & brainstem , consistent with Chiari 2.*

**Endoscopic 3rd Ventriculostomy**
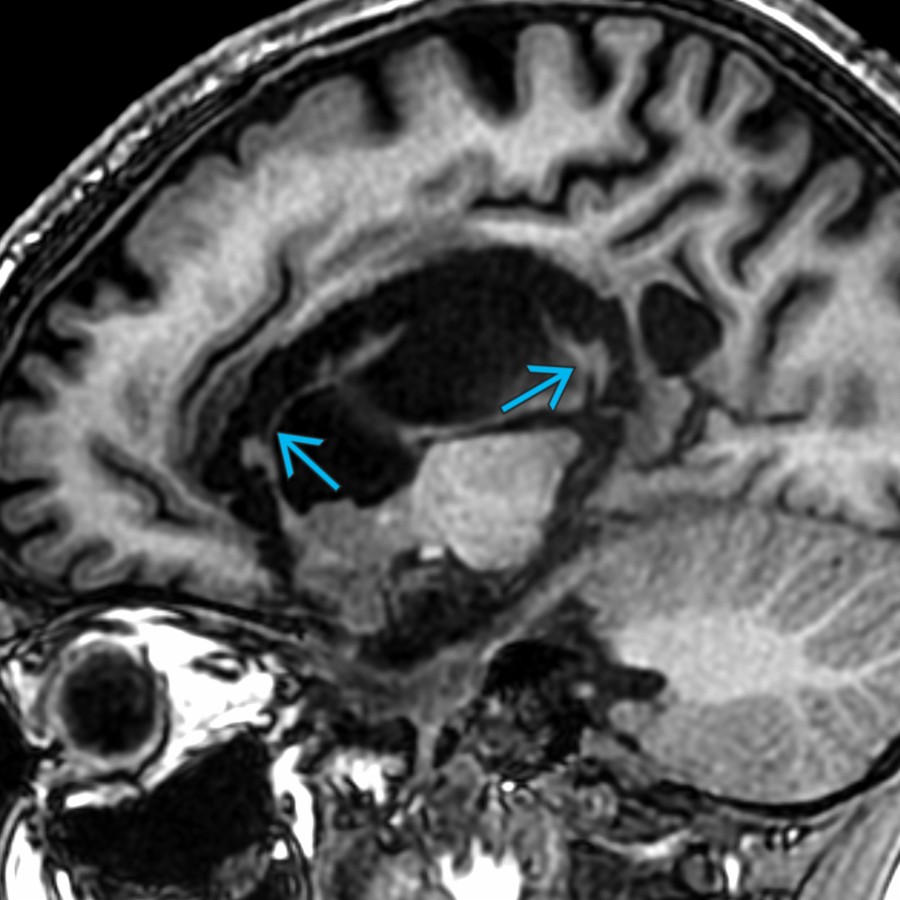
*Paramidline sagittal T2 MR in a teenager with a history of a prior endoscopic 3rd ventriculostomy shows a linear defect in the parasagittal body of the CC. The defect represents the site of surgical access for the scope to enter the 3rd ventricle.*
**Obstructive Hydrocephalus**
*Midline sagittal T2 MR in a neonate with posthemorrhagic hydrocephalus shows a stretched & thinned CC . Note the enlarged lateral , 3rd , & 4th ventricles as well as thin T2 hypointensity along the brainstem, consistent with hemosiderin deposition.*

**Obstructive Hydrocephalus**
*Midline sagittal T1 MR in the same patient 1 year after shunting shows a thinned & dysmorphic CC as well as numerous thin, pencil-like gyri (stenogyria) .*

**Corpus Callosotomy**
*Coronal FLAIR MR shows changes of a left functional hemispherotomy with a WM disconnection & insular decortication . Corpus callosotomy may be performed in isolation or as part of a more extensive functional hemispherotomy, as in this patient.*

**Corpus Callosotomy**
*Coronal T2 MR shows absence of the midline CC with persistent paramidline callosal tissue , consistent with an isolated surgical callosotomy.*

**Ventricular Drainage Catheter Tract**
*Paramidline sagittal T1 MR in a 12 year old with Chiari 2 malformation shows a ventricular shunt catheter tract in the anterior body of the CC. Note the caudal migration of the cerebellum & brainstem , consistent with Chiari 2.*

**Endoscopic 3rd Ventriculostomy**
*Paramidline sagittal T2 MR in a teenager with a history of a prior endoscopic 3rd ventriculostomy shows a linear defect in the parasagittal body of the CC. The defect represents the site of surgical access for the scope to enter the 3rd ventricle.*
 . Also note the extensive periventricular gray matter (GM) heterotopia .](images/app.statdx.com_image_thumbnail_82c23417-cc0d-47b9-a72c-9253390c8669_annotated_true_size_900_quality_90_7081e987_20251018T142242Z.jpg)
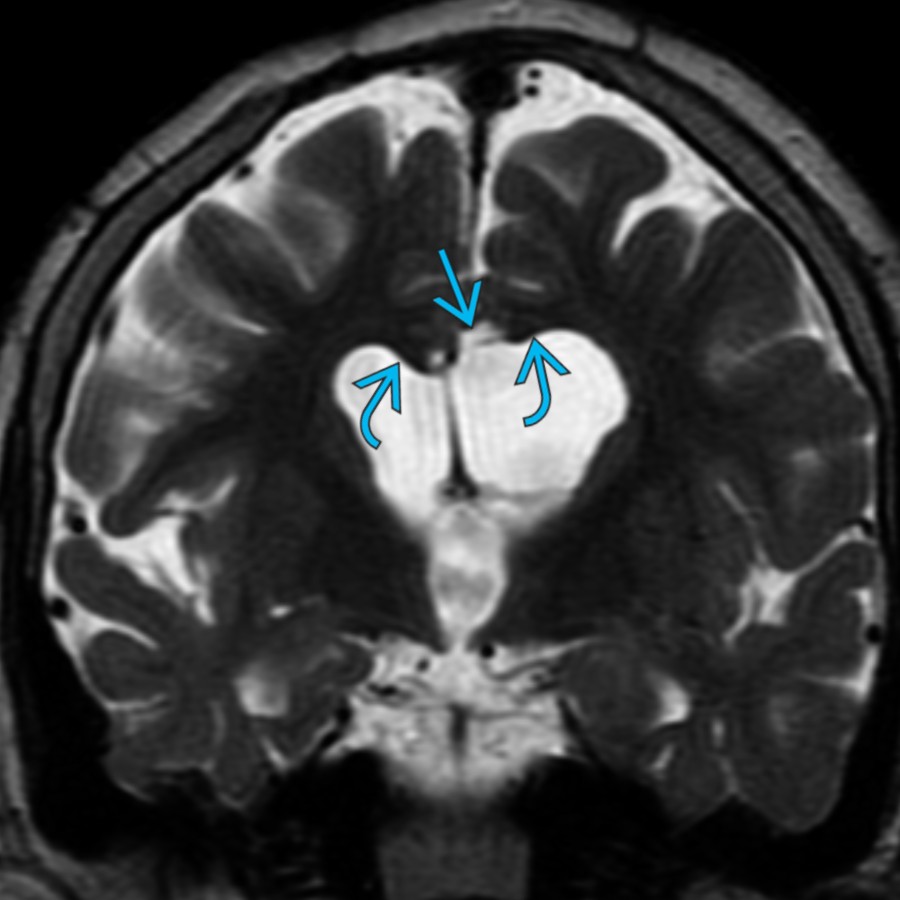
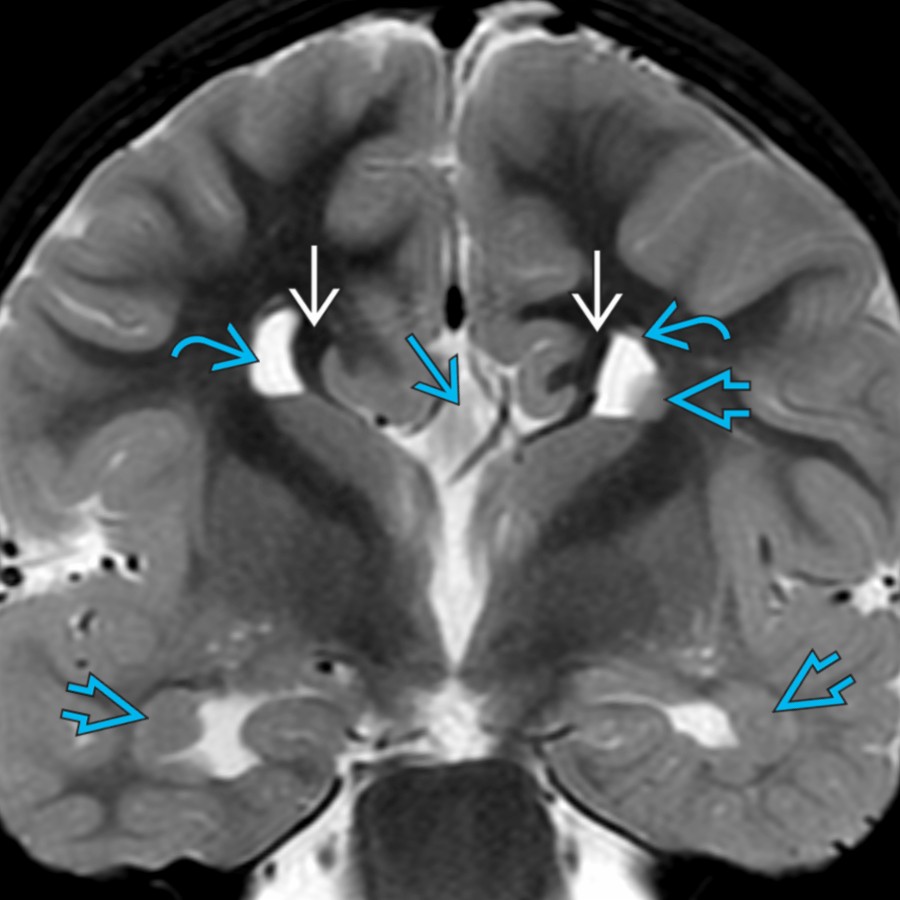
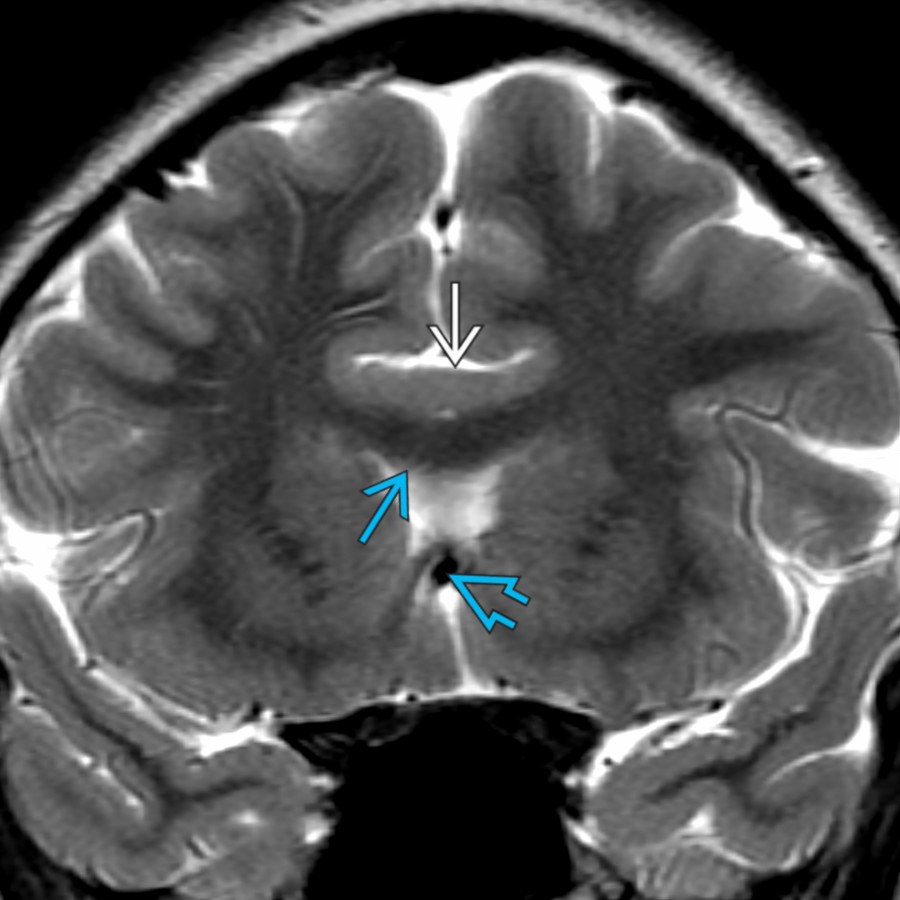
**Callosal Agenesis**
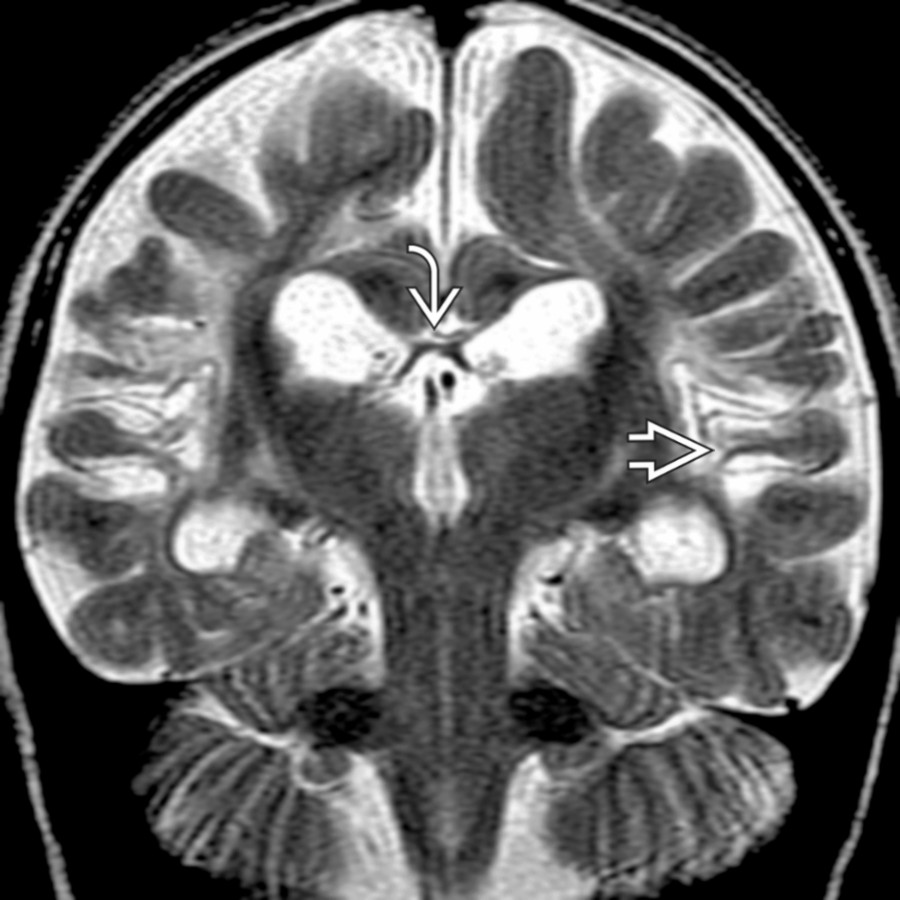
*Coronal T2 MR in a 4 year old with callosal agenesis shows widely spaced upturned lateral ventricular frontal horns , a high-riding 3rd ventricle , & bilateral Probst bundles . Also note the extensive periventricular gray matter (GM) heterotopia .*
**Callosal Agenesis**
*Coronal T2 MR in a 4 year old with callosal agenesis shows widely spaced upturned lateral ventricular frontal horns , a high-riding 3rd ventricle , & bilateral Probst bundles . Also note the extensive periventricular gray matter (GM) heterotopia .*
 with no evident rostrum or splenium. Isolated callosal dysgenesis is uncommon. Associated anomalies should be carefully sought.](images/app.statdx.com_image_thumbnail_5ba333fc-5752-4158-9879-eb9fba5607f7_annotated_true_size_900_quality_90_67a96337_20251018T142242Z.jpg)
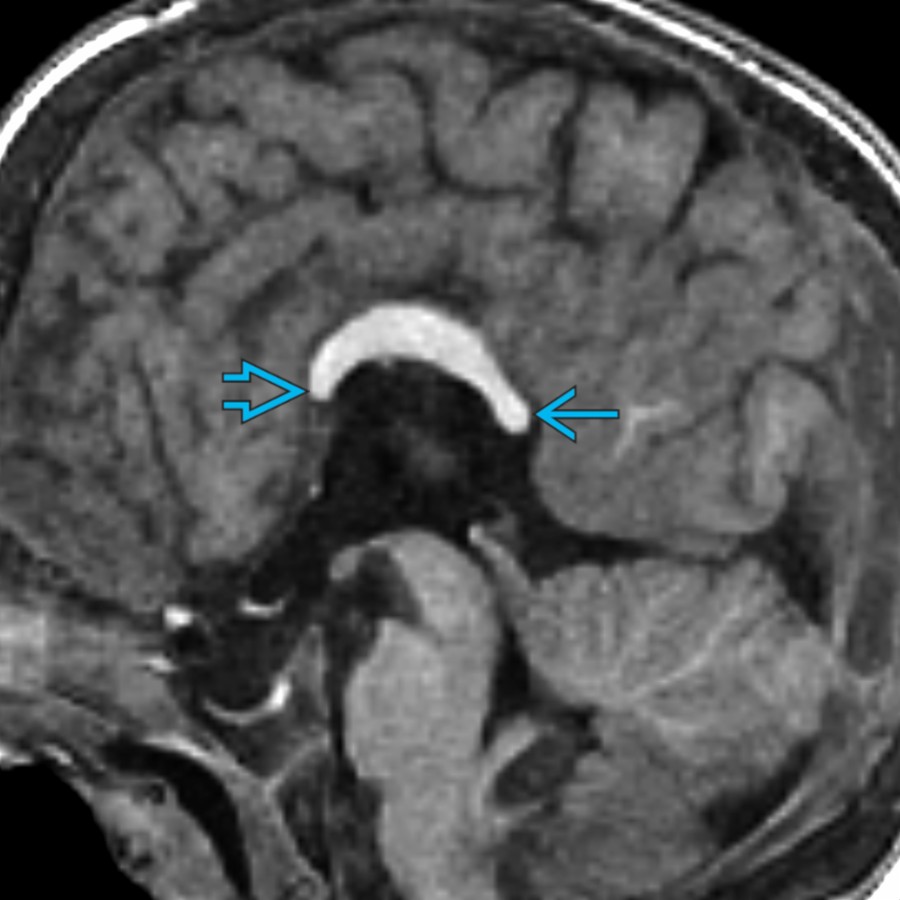
**Callosal Dysgenesis**
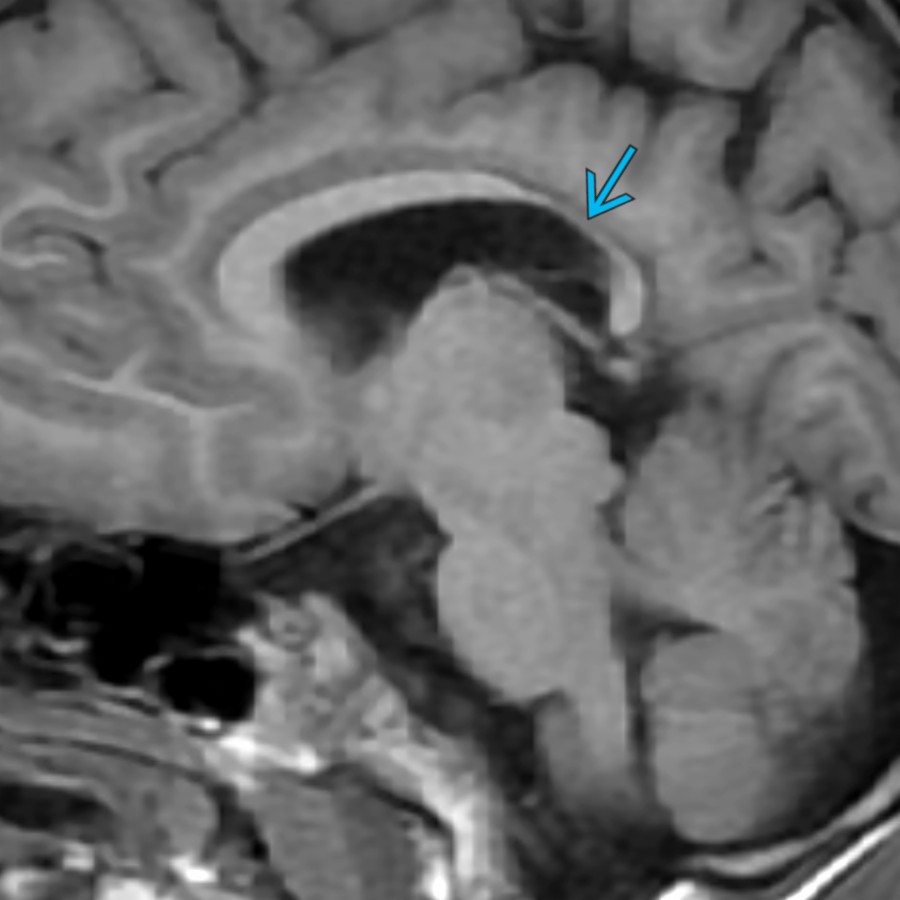
*Midline sagittal T1 MR in a 5 month old with isolated callosal dysgenesis shows a very short & thin CC with no evident rostrum or splenium. Isolated callosal dysgenesis is uncommon. Associated anomalies should be carefully sought.*
**Callosal Dysgenesis**
*Midline sagittal T1 MR in a 7 year old with multiple anomalies shows a short, thin, & dysmorphic CC with a poorly formed splenium & rostrum .*
**Chiari 2 Malformation**
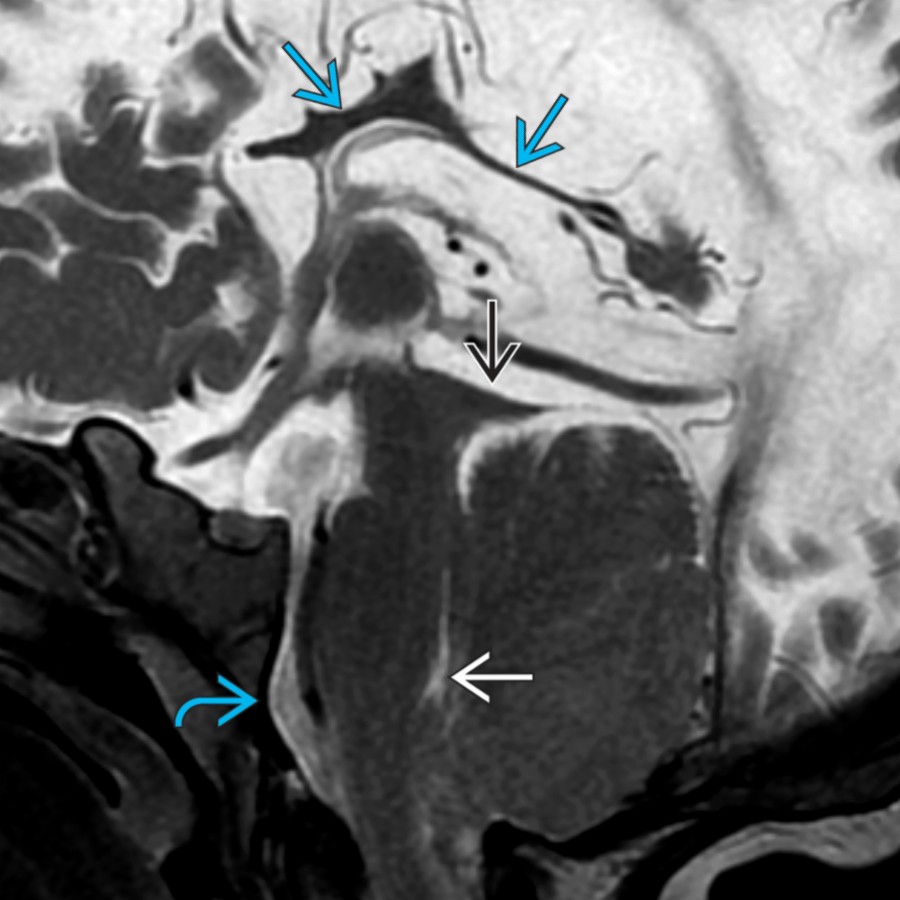
*Midline sagittal T2 MR in a child with a repaired myelomeningocele & Chiari 2 malformation (with beaked tectum , small 4th ventricle , & scalloped clivus ) shows a thinned & dysmorphic CC .*
**Glioblastoma**
*Coronal T2 MR in a 10 year old with glioblastoma shows mass-like infiltrative signal crossing the midline through an expanded CC. Infiltrative high-grade glial neoplasms should be considered whenever such a finding is encountered, as they commonly spread along WM tracts, such as the CC.*

**Lymphoma**
*Midline sagittal T2 MR shows expansion & increased signal in the rostrum & anterior genu of the CC , consistent with tumor infiltration/edema in this patient with CNS lymphoma.*
**Pericallosal Lipoma**
*Midline sagittal T1 MR in a 4 month old shows a T1-hyperintense lipoma along the dorsal CC with associated absence of the splenium .*
**Neurofibromatosis Type 1**
*Midline sagittal T1 MR in a 15 year old with neurofibromatosis type 1 (NF1) shows diffuse marked thickening of the entire CC, a finding that can be seen in NF1. Look for associated findings of NF1, such as nonenhancing signal abnormalities of the globus pallidus & medial cerebellum, optic pathway gliomas, & plexiform neurofibromas.*

**Holoprosencephaly**
*Midline sagittal T2 MR shows absence of the CC in a patient with alobar holoprosencephaly. There is continuity of frontal WM & GM across the midline with a large dorsal cyst that communicates with a monoventricle . Note the lack of a vermian primary fissure due to associated rhombencephalosynapsis.*
**Holoprosencephaly**
*Midline sagittal T1 MR in a 2 year old with semilobar holoprosencephaly shows absence of a normal CC & extension of cortical GM across the midline.*
**Holoprosencephaly**
*Midline sagittal T1 MR in a teenager with the middle interhemispheric variant of holoprosencephaly shows an intact CC anteriorly & posteriorly but abnormal extension of GM across the midline in the expected location of the CC body. The abnormal body of the CC typically "dips" down toward the interthalamic adhesion.*
**Holoprosencephaly**
*Coronal T2 MR in the same patient with syntelencephaly shows abnormal GM crossing the midline along the CC WM . Also note the azygous internal carotid artery (ICA) .*

**Metachromatic Leukodystrophy**
*Coronal T2 MR in a 13-year-old female patient with metachromatic leukodystrophy shows symmetric extensive WM signal abnormality with preservation of the subcortical WM . Note the marked thinning of the CC .*
**X-Linked Adrenoleukodystrophy**
*Axial FLAIR MR in a 14-year-old male patient with X-linked adrenoleukodystrophy (ALD) shows symmetric increased FLAIR signal intensity that crosses the splenium of the CC. This is the most common distribution of signal abnormality in X-linked ALD.*
### Additional Images
**Normal Variant**
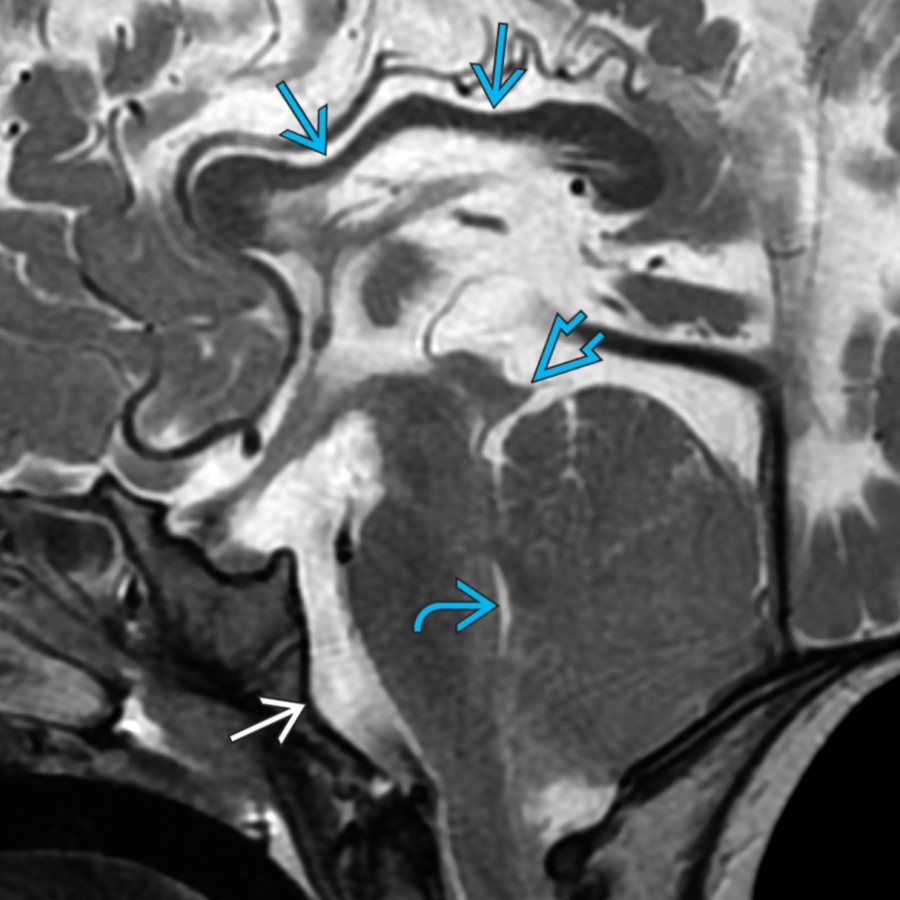
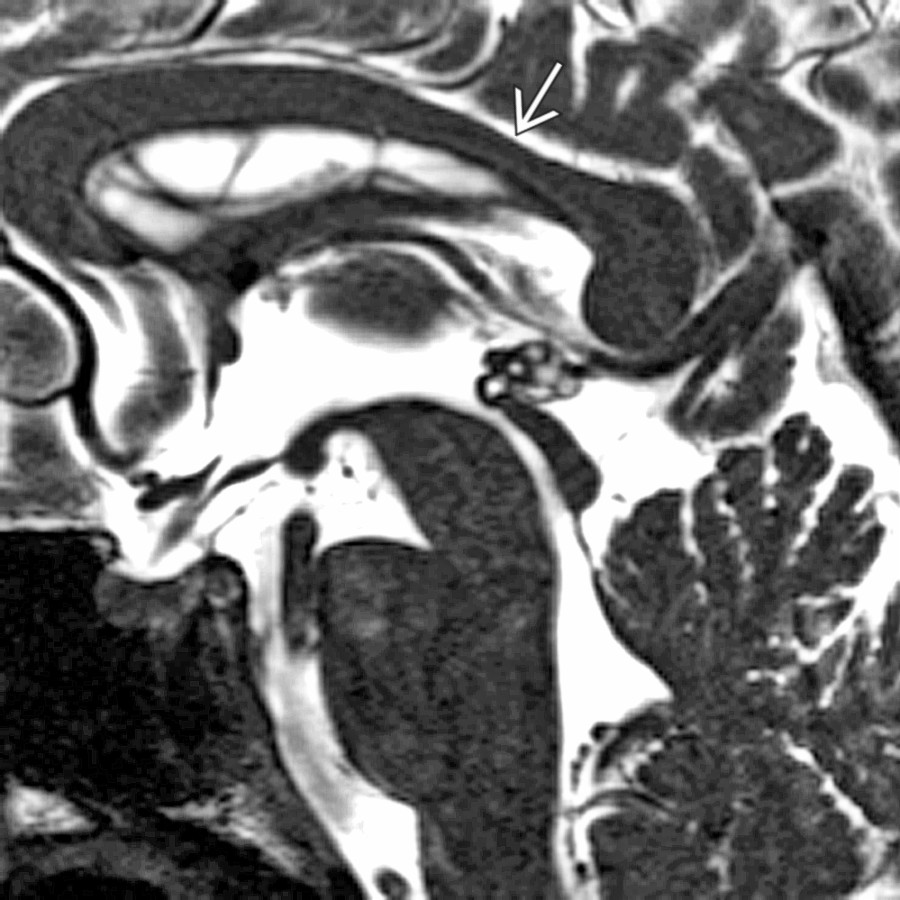
*Midline sagittal 3D SSFP MR with a close-up view of the corpus callosum shows normal "wavy" dorsal surface. Note the focal thinning along the posterior body , a common normal finding.*
**Callosal Dysgenesis**
*Midline sagittal T1 MR in a 5 month old with isolated callosal dysgenesis shows a very short & thin CC with no evident rostrum or splenium. Isolated callosal dysgenesis is uncommon. Associated anomalies should be carefully sought.*

**Callosal Dysgenesis**
*Midline sagittal T1 MR in a 7 year old with multiple anomalies shows a short, thin, & dysmorphic CC with a poorly formed splenium & rostrum .*

**Chiari 2 Malformation**
*Midline sagittal T2 MR in a child with a repaired myelomeningocele & Chiari 2 malformation (with beaked tectum , small 4th ventricle , & scalloped clivus ) shows a thinned & dysmorphic CC .*

**Glioblastoma**
*Coronal T2 MR in a 10 year old with glioblastoma shows mass-like infiltrative signal crossing the midline through an expanded CC. Infiltrative high-grade glial neoplasms should be considered whenever such a finding is encountered, as they commonly spread along WM tracts, such as the CC.*

**Lymphoma**
*Midline sagittal T2 MR shows expansion & increased signal in the rostrum & anterior genu of the CC , consistent with tumor infiltration/edema in this patient with CNS lymphoma.*

**Pericallosal Lipoma**
*Midline sagittal T1 MR in a 4 month old shows a T1-hyperintense lipoma along the dorsal CC with associated absence of the splenium .*

**Neurofibromatosis Type 1**
*Midline sagittal T1 MR in a 15 year old with neurofibromatosis type 1 (NF1) shows diffuse marked thickening of the entire CC, a finding that can be seen in NF1. Look for associated findings of NF1, such as nonenhancing signal abnormalities of the globus pallidus & medial cerebellum, optic pathway gliomas, & plexiform neurofibromas.*

**Holoprosencephaly**
*Midline sagittal T2 MR shows absence of the CC in a patient with alobar holoprosencephaly. There is continuity of frontal WM & GM across the midline with a large dorsal cyst that communicates with a monoventricle . Note the lack of a vermian primary fissure due to associated rhombencephalosynapsis.*

**Holoprosencephaly**
*Midline sagittal T1 MR in a 2 year old with semilobar holoprosencephaly shows absence of a normal CC & extension of cortical GM across the midline.*

**Holoprosencephaly**
*Midline sagittal T1 MR in a teenager with the middle interhemispheric variant of holoprosencephaly shows an intact CC anteriorly & posteriorly but abnormal extension of GM across the midline in the expected location of the CC body. The abnormal body of the CC typically "dips" down toward the interthalamic adhesion.*

**Holoprosencephaly**
*Coronal T2 MR in the same patient with syntelencephaly shows abnormal GM crossing the midline along the CC WM . Also note the azygous internal carotid artery (ICA) .*

**Metachromatic Leukodystrophy**
*Coronal T2 MR in a 13-year-old female patient with metachromatic leukodystrophy shows symmetric extensive WM signal abnormality with preservation of the subcortical WM . Note the marked thinning of the CC .*

**X-Linked Adrenoleukodystrophy**
*Axial FLAIR MR in a 14-year-old male patient with X-linked adrenoleukodystrophy (ALD) shows symmetric increased FLAIR signal intensity that crosses the splenium of the CC. This is the most common distribution of signal abnormality in X-linked ALD.*
### Additional Images

**Normal Variant**
*Midline sagittal 3D SSFP MR with a close-up view of the corpus callosum shows normal "wavy" dorsal surface. Note the focal thinning along the posterior body , a common normal finding.*
 is normal.](images/app.statdx.com_image_thumbnail_2148930a-f910-449f-8f04-9b59c8919068_annotated_true_size_900_quality_90_4e19bec0_20251018T142218Z.jpg)
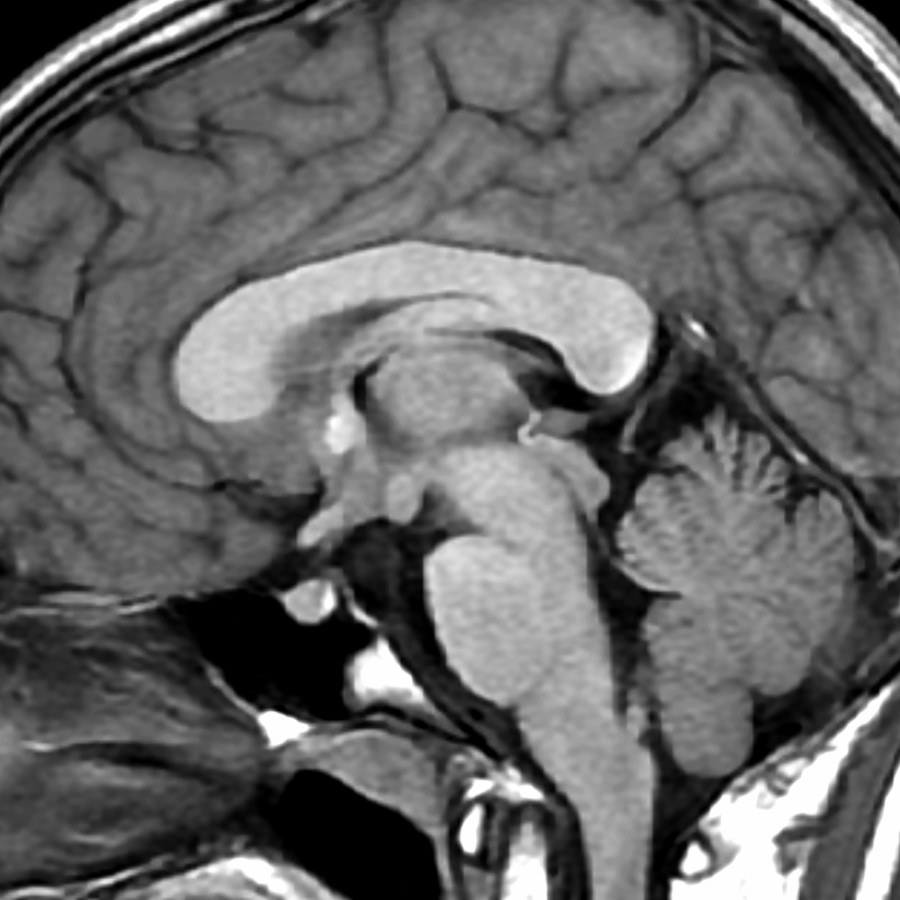
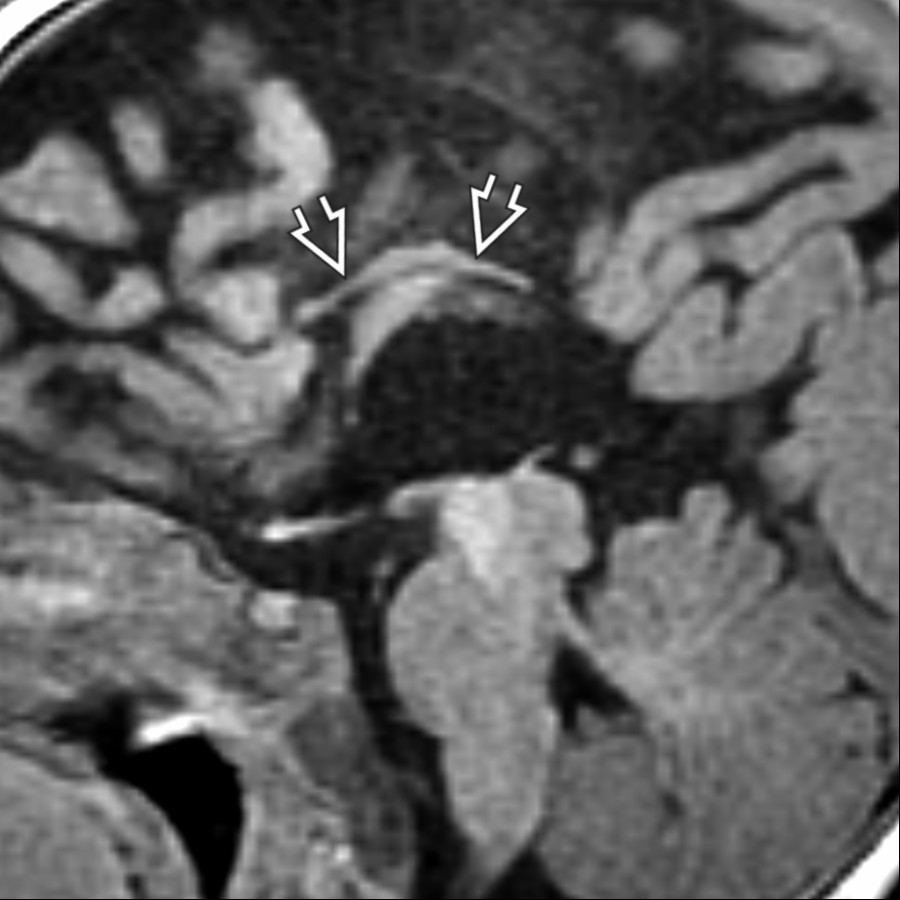
**Normal Variant**
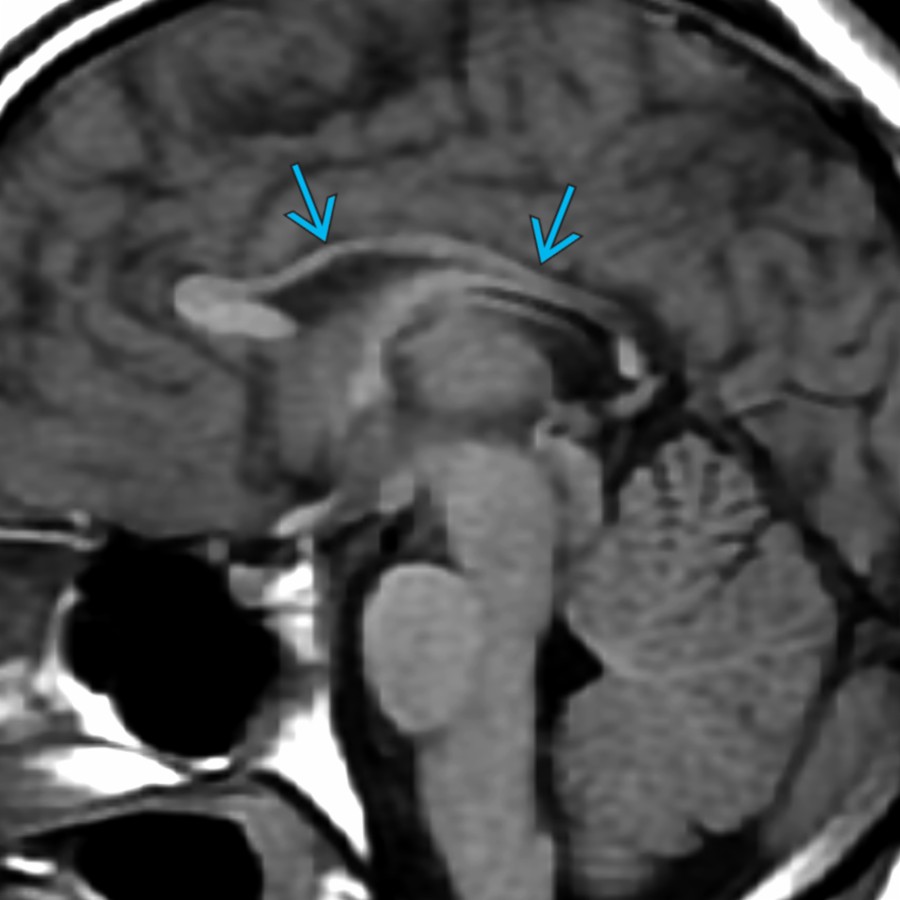
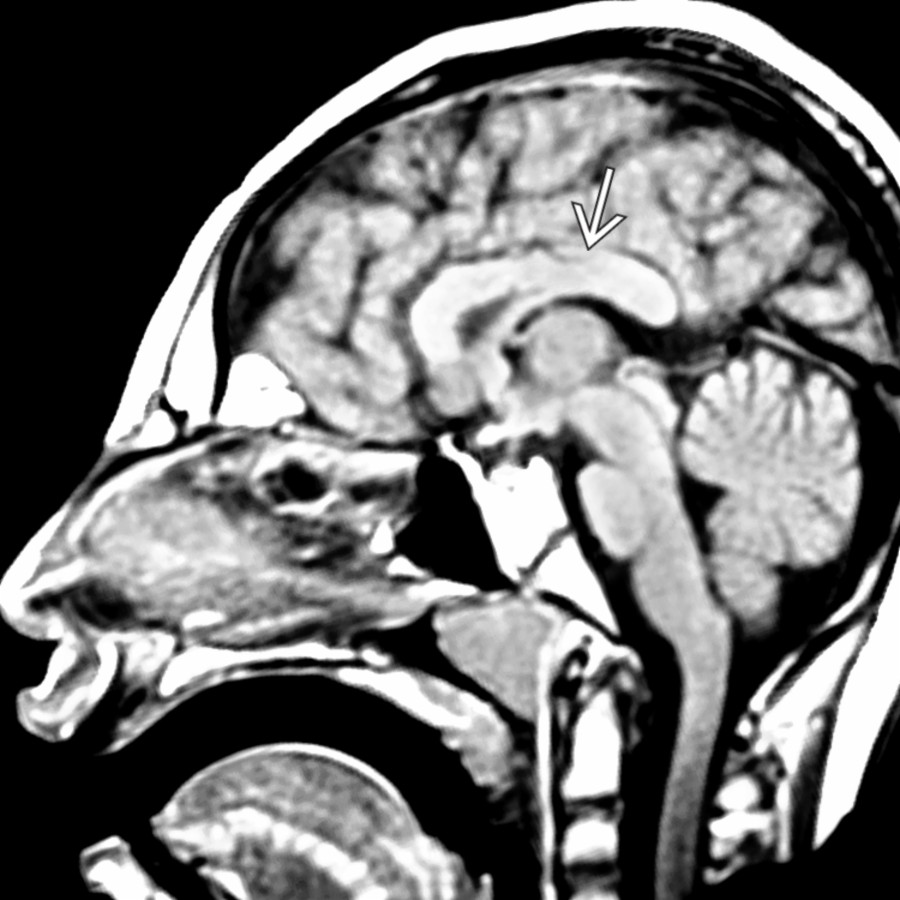
*Midline sagittal T1 MR shows a normal neonatal corpus callosum , thin due to an age-appropriate lack of myelin. The cingulate gyrus is normal.*
**Periventricular Leukomalacia**
*Midline sagittal T1 MR shows diffuse thinning of the posterior corpus callosum , greater than typically seen. The thinning of the corpus callosum is secondary to loss of commissural fibers, damaged by periventricular leukomalacia.*

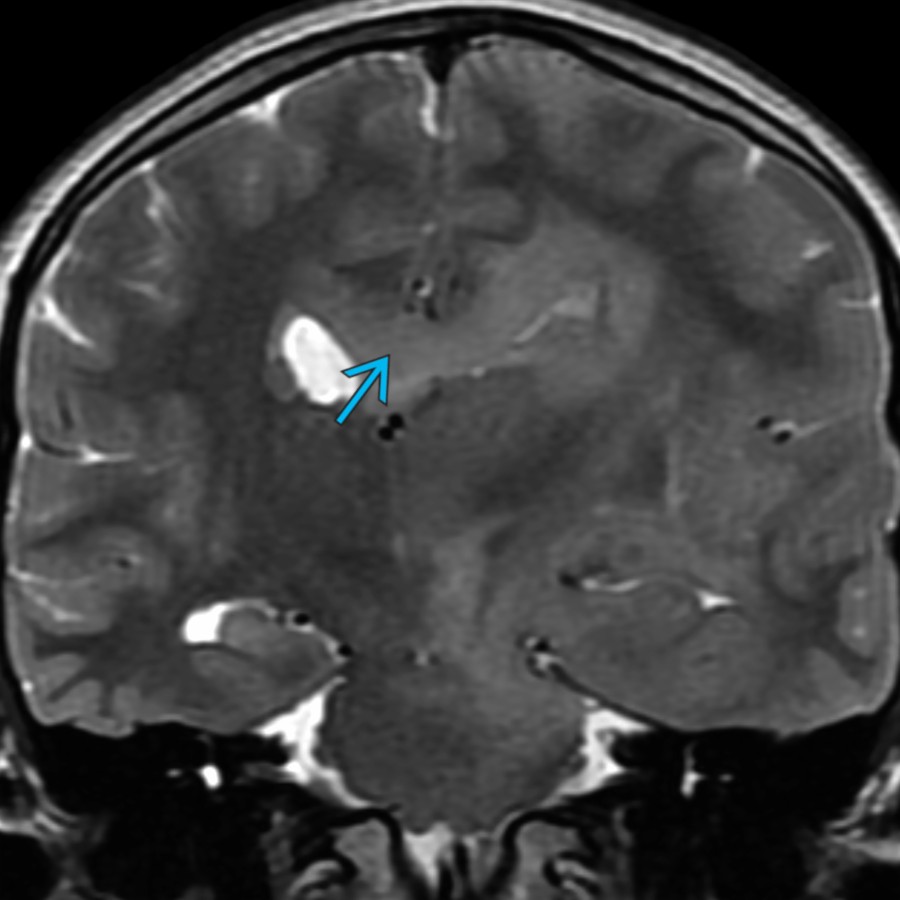
**Periventricular Leukomalacia**
*Axial T2 MR in the same child shows marked loss of the right periventricular parenchyma at the site of a prior grade 4 hemorrhage. The posterior white matter loss correlates with the focal corpus callosum atrophy .*
**Periventricular Leukomalacia**
*Midline sagittal T1 MR shows marked callosal thinning in a child whose hydrocephalus follows unilateral grade 4 intraventricular hemorrhage. Note the more severe callosal volume loss posteriorly .*

**Chronic Cerebral Infarction**
*Midline sagittal T1 MR shows thinning of the body & splenium of the corpus callosum following neonatal parietooccipital ischemia & gliosis from a combination of hypoxic ischemic encephalopathy & hypoglycemia.*
**Chronic Cerebral Infarction**
*Coronal T2 MR shows parietal ulegyria & marked thinning of the posterior corpus callosum .*

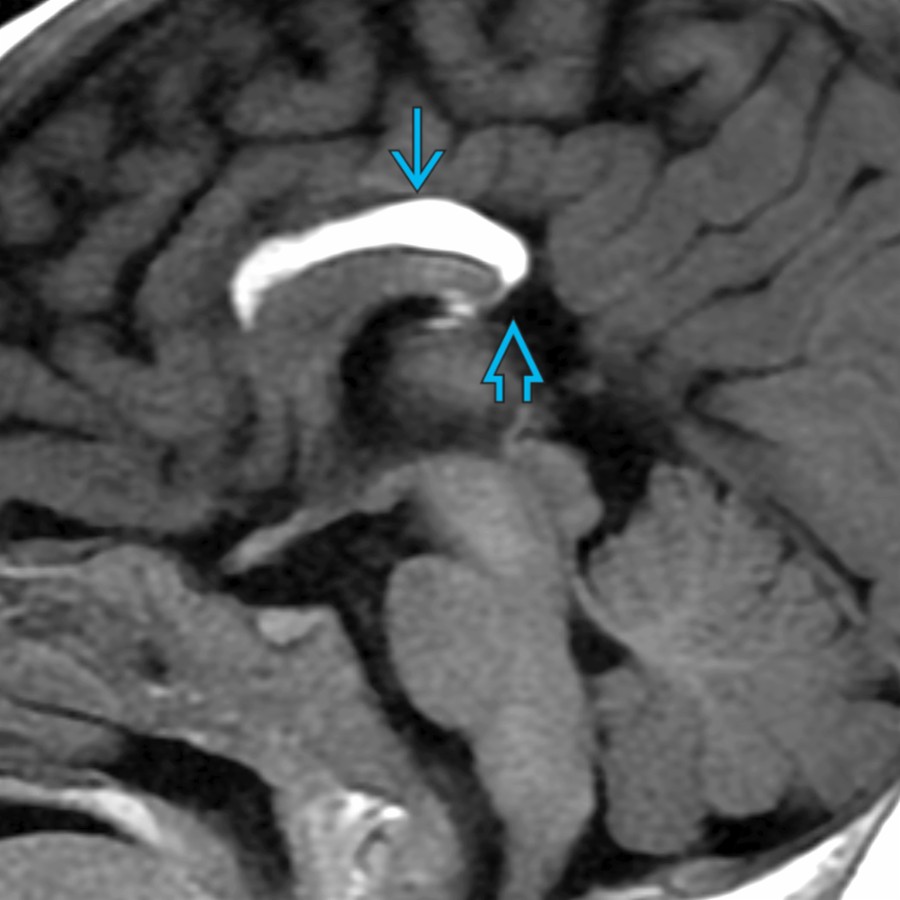
**Obstructive Hydrocephalus**
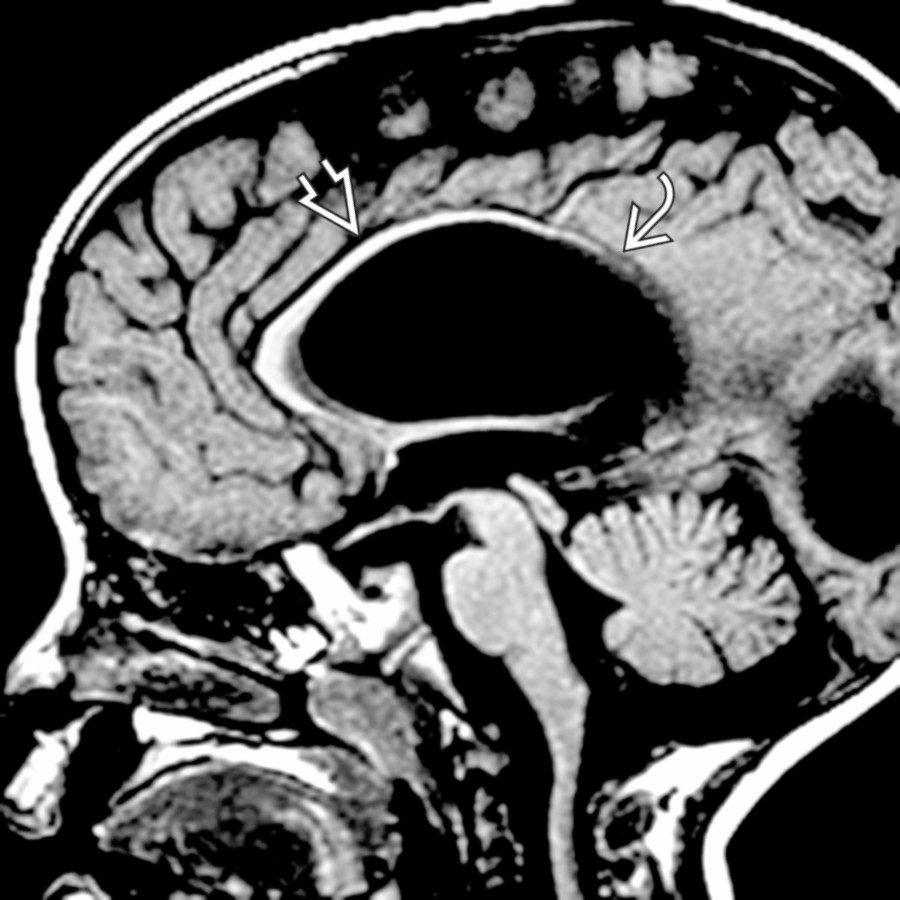
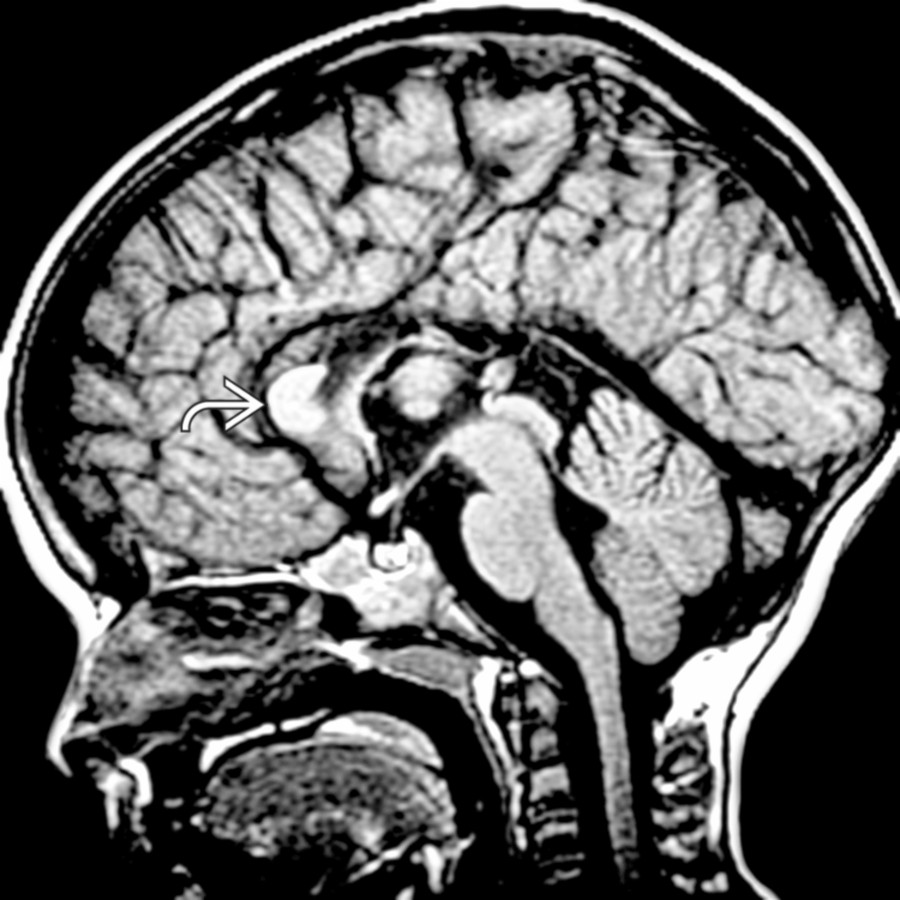
*Midline sagittal T2 MR shows mild stretching & thinning of the corpus callosum due to hydrocephalus. There is obstruction of the aqueduct of Sylvius by a tectal glioma .*

**Chemotherapy & Radiation Therapy**
*Coronal FLAIR MR shows thinning & gliosis of the corpus callosum & surrounding white matter following therapy for acute lymphoblastic leukemia (ALL).*
**Postsurgical Defects**
*Midline sagittal T1 MR shows a focal defect at the junction of the genu & body of the corpus callosum , which had been the site of a prior surgical approach to this child's suprasellar tumor .*
**Corpus Callosotomy**
*Paramidline sagittal T1 MR in a 7 year old with intractable epilepsy shows near-complete absence of the corpus callosum due to surgical discontinuity.*
**Corpus Callosotomy**
*Midline sagittal T2 MR in an 11 year old with intractable epilepsy who had undergone an isolated corpus callosotomy shows absence of the corpus callosum but presence of a cingulate gyrus . The presence of a cingulate gyrus would not be expected with congenital agenesis of the corpus callosum.*
**Callosal Agenesis**
*Midline sagittal T1 MR shows complete absence of the corpus callosum with associated absence of the cingulate gyrus. Note the radial arrangement of parasagittal gyri/sulci , which point toward the 3rd ventricle.*
**Callosal Agenesis**
*Axial T1 MR in a patient with callosal agenesis shows parallel lateral ventricles with colpocephaly , resulting in a typical tear-drop shape.*
**Primary Callosal Dysgenesis**
*Midline sagittal T1 MR shows only a residual genu of the corpus callosum with absence of the body & splenium as well as truncation of the rostrum.*
**Primary Callosal Dysgenesis**
*Midline sagittal T1 MR in a child with severe microcephaly shows a short, thick corpus callosum .*
**Chiari 2 Malformation**
*Midline sagittal T1 MR shows an abnormal corpus callosum with an absent rostrum, small deformed genu, thick body , & absent splenium in this child with a Chiari 2 malformation due to a myelomeningocele. Note the prominent massa intermedia , inferiorly beaked tectum , & caudally displaced elongated 4th ventricle with flattening of the fastigium .*

**Chiari 2 Malformation**
*Axial T2 MR shows a prominent massa intermedia & colpocephalic lateral ventricles with periventricular white matter deficiency in Chiari 2. The genu of the corpus callosum, usually seen on axial images, is absent.*
**Chiari 2 Malformation**
*Midline sagittal T2 MR in a 15 month old with Chiari 2 malformation shows a severely thinned & dysmorphic corpus callosum . Note the typical Chiari 2 features, including a small posterior fossa with caudal herniation of the brainstem & cerebellum, clival scalloping , elongated 4th ventricle , & beaked tectum .*
**Glioblastoma**
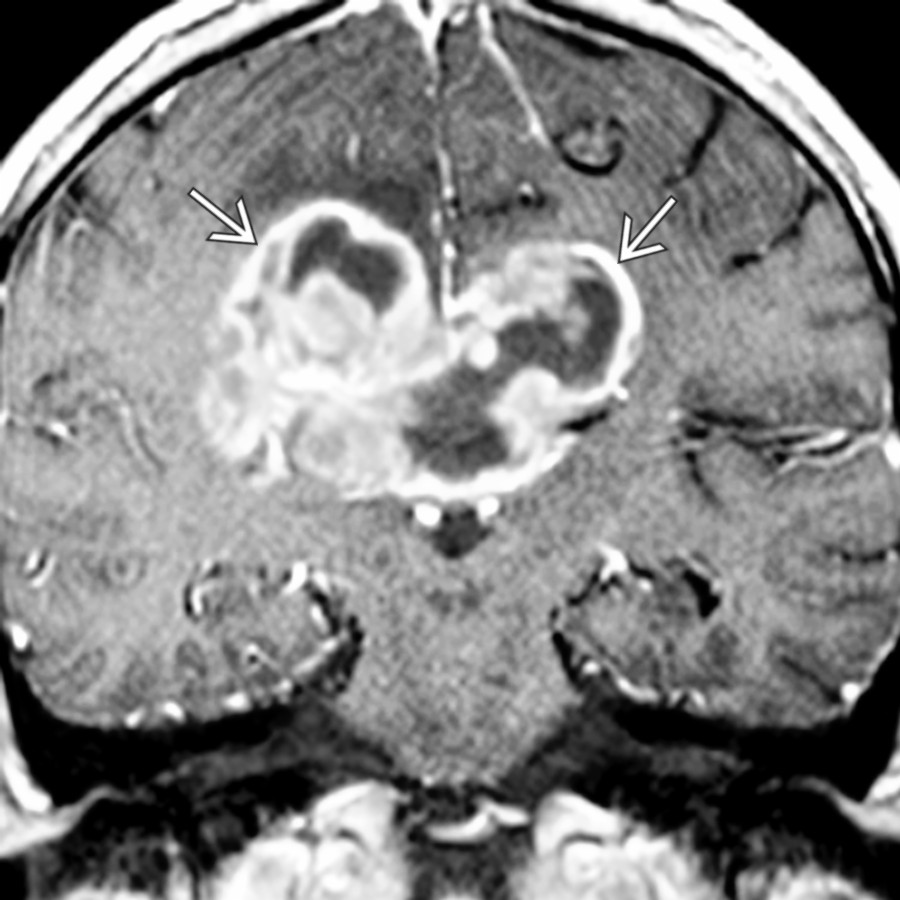
*Coronal T1 C+ MR shows a classic "butterfly" glioblastoma multiforme of the corpus callosum . Central necrosis with an irregular rind of enhancing tumor is typical.*
**Lymphoma**
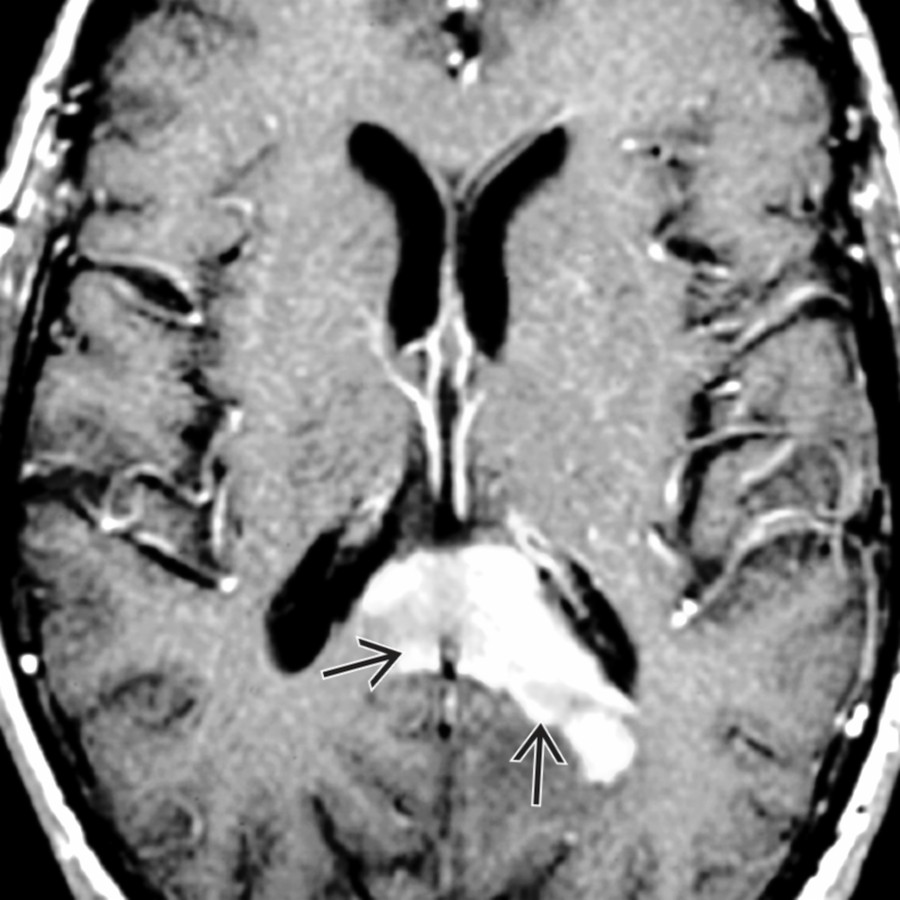
*Axial T1 C+ MR shows a primary CNS lymphoma involving the splenium of the corpus callosum. There is avid, solid enhancement of the tumor with extension into the adjacent parenchymal white matter.*
**Lymphoma**
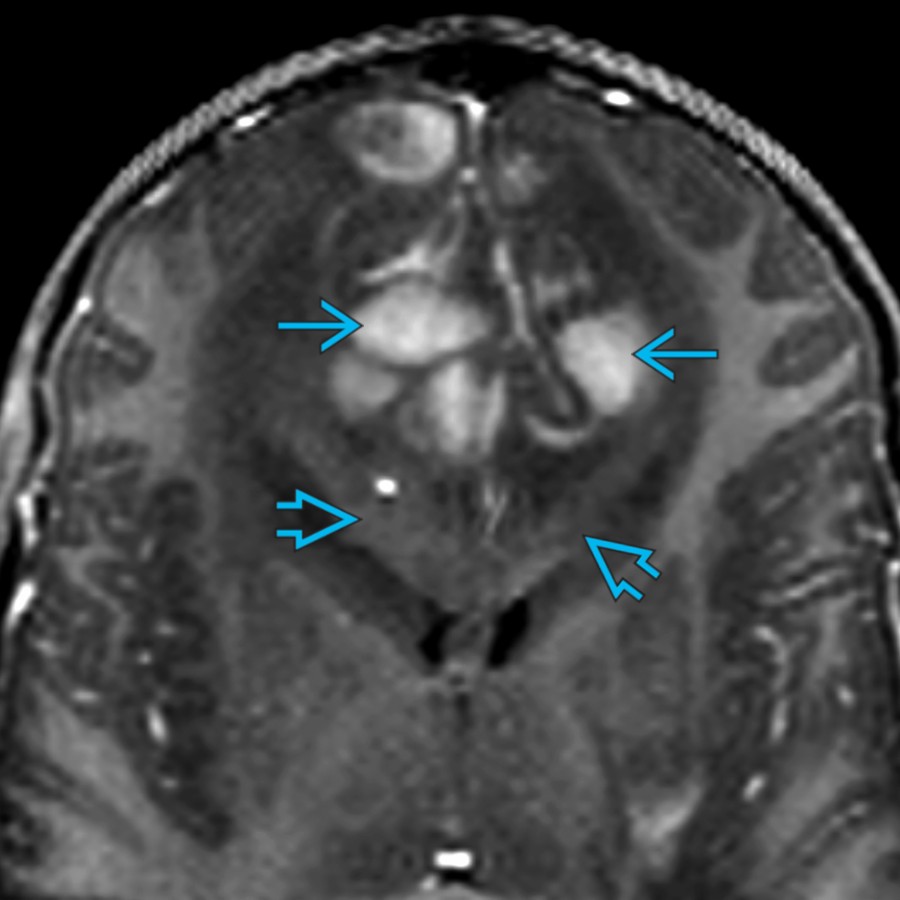
*Coronal oblique T1 C+ MR in an 11 year old with CNS lymphoma shows bifrontal areas of enhancement , which corresponded to hyperdense areas on CT (not shown). Note the abnormally thickened corpus callosum that is infiltrated by a nonenhancing tumor.*

**Pericallosal Lipoma**
*Midline sagittal T1 MR shows a large pericallosal lipoma with severe dysgenesis of the corpus callosum .*

**Pericallosal Lipoma**
*Axial FLAIR MR shows a large midline lipoma. Two smaller lipomatous masses protrude into the lateral ventricles.*
**Holoprosencephaly**
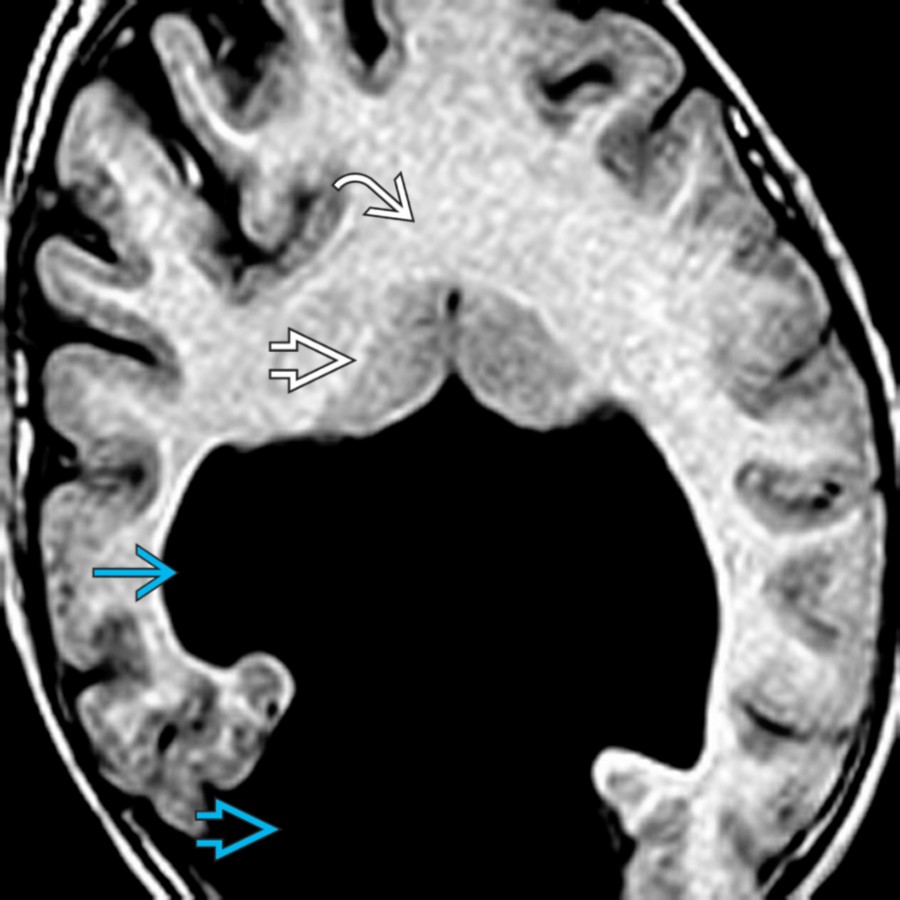
*Axial T1 MR in a patient with holoprosencephaly shows the lack of a midline fissure. White matter is in continuity across the midline. The small basal ganglia approximate each other. Note the monoventricle communicating with a dorsal cyst .*

**Holoprosencephaly**
*Midline sagittal T1 MR shows both white & gray matter crossing midline anterior & posterior to the "dip" in the corpus callosum, where only gray matter traverses. This is a middle interhemispheric variant of holoprosencephaly (syntelencephaly).*
**Holoprosencephaly**
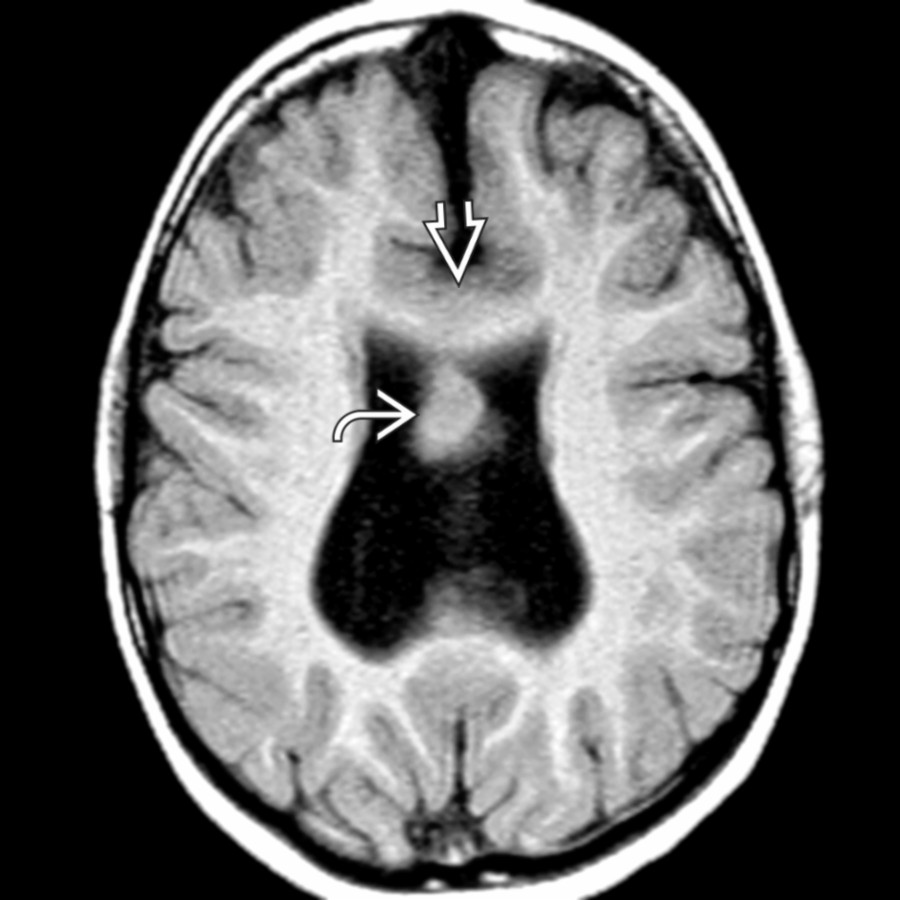
*Axial T1 MR in the same patient shows gray & white matter traversing the midline in the expected location of the splenium. Gray matter also protrudes into the ventricular system. The septum pellucidum is absent.*
is normal.](images/app.statdx.com_image_thumbnail_2148930a-f910-449f-8f04-9b59c8919068_annotated_true_size_900_quality_90_4e19bec0_20251018T142218Z.jpg)
**Normal Variant**
*Midline sagittal T1 MR shows a normal neonatal corpus callosum , thin due to an age-appropriate lack of myelin. The cingulate gyrus is normal.*

**Periventricular Leukomalacia**
*Midline sagittal T1 MR shows diffuse thinning of the posterior corpus callosum , greater than typically seen. The thinning of the corpus callosum is secondary to loss of commissural fibers, damaged by periventricular leukomalacia.*

**Periventricular Leukomalacia**
*Axial T2 MR in the same child shows marked loss of the right periventricular parenchyma at the site of a prior grade 4 hemorrhage. The posterior white matter loss correlates with the focal corpus callosum atrophy .*

**Periventricular Leukomalacia**
*Midline sagittal T1 MR shows marked callosal thinning in a child whose hydrocephalus follows unilateral grade 4 intraventricular hemorrhage. Note the more severe callosal volume loss posteriorly .*

**Chronic Cerebral Infarction**
*Midline sagittal T1 MR shows thinning of the body & splenium of the corpus callosum following neonatal parietooccipital ischemia & gliosis from a combination of hypoxic ischemic encephalopathy & hypoglycemia.*

**Chronic Cerebral Infarction**
*Coronal T2 MR shows parietal ulegyria & marked thinning of the posterior corpus callosum .*

**Obstructive Hydrocephalus**
*Midline sagittal T2 MR shows mild stretching & thinning of the corpus callosum due to hydrocephalus. There is obstruction of the aqueduct of Sylvius by a tectal glioma .*

**Chemotherapy & Radiation Therapy**
*Coronal FLAIR MR shows thinning & gliosis of the corpus callosum & surrounding white matter following therapy for acute lymphoblastic leukemia (ALL).*

**Postsurgical Defects**
*Midline sagittal T1 MR shows a focal defect at the junction of the genu & body of the corpus callosum , which had been the site of a prior surgical approach to this child's suprasellar tumor .*

**Corpus Callosotomy**
*Paramidline sagittal T1 MR in a 7 year old with intractable epilepsy shows near-complete absence of the corpus callosum due to surgical discontinuity.*

**Corpus Callosotomy**
*Midline sagittal T2 MR in an 11 year old with intractable epilepsy who had undergone an isolated corpus callosotomy shows absence of the corpus callosum but presence of a cingulate gyrus . The presence of a cingulate gyrus would not be expected with congenital agenesis of the corpus callosum.*

**Callosal Agenesis**
*Midline sagittal T1 MR shows complete absence of the corpus callosum with associated absence of the cingulate gyrus. Note the radial arrangement of parasagittal gyri/sulci , which point toward the 3rd ventricle.*

**Callosal Agenesis**
*Axial T1 MR in a patient with callosal agenesis shows parallel lateral ventricles with colpocephaly , resulting in a typical tear-drop shape.*

**Primary Callosal Dysgenesis**
*Midline sagittal T1 MR shows only a residual genu of the corpus callosum with absence of the body & splenium as well as truncation of the rostrum.*

**Primary Callosal Dysgenesis**
*Midline sagittal T1 MR in a child with severe microcephaly shows a short, thick corpus callosum .*

**Chiari 2 Malformation**
*Midline sagittal T1 MR shows an abnormal corpus callosum with an absent rostrum, small deformed genu, thick body , & absent splenium in this child with a Chiari 2 malformation due to a myelomeningocele. Note the prominent massa intermedia , inferiorly beaked tectum , & caudally displaced elongated 4th ventricle with flattening of the fastigium .*

**Chiari 2 Malformation**
*Axial T2 MR shows a prominent massa intermedia & colpocephalic lateral ventricles with periventricular white matter deficiency in Chiari 2. The genu of the corpus callosum, usually seen on axial images, is absent.*

**Chiari 2 Malformation**
*Midline sagittal T2 MR in a 15 month old with Chiari 2 malformation shows a severely thinned & dysmorphic corpus callosum . Note the typical Chiari 2 features, including a small posterior fossa with caudal herniation of the brainstem & cerebellum, clival scalloping , elongated 4th ventricle , & beaked tectum .*

**Glioblastoma**
*Coronal T1 C+ MR shows a classic "butterfly" glioblastoma multiforme of the corpus callosum . Central necrosis with an irregular rind of enhancing tumor is typical.*

**Lymphoma**
*Axial T1 C+ MR shows a primary CNS lymphoma involving the splenium of the corpus callosum. There is avid, solid enhancement of the tumor with extension into the adjacent parenchymal white matter.*

**Lymphoma**
*Coronal oblique T1 C+ MR in an 11 year old with CNS lymphoma shows bifrontal areas of enhancement , which corresponded to hyperdense areas on CT (not shown). Note the abnormally thickened corpus callosum that is infiltrated by a nonenhancing tumor.*

**Pericallosal Lipoma**
*Midline sagittal T1 MR shows a large pericallosal lipoma with severe dysgenesis of the corpus callosum .*

**Pericallosal Lipoma**
*Axial FLAIR MR shows a large midline lipoma. Two smaller lipomatous masses protrude into the lateral ventricles.*

**Holoprosencephaly**
*Axial T1 MR in a patient with holoprosencephaly shows the lack of a midline fissure. White matter is in continuity across the midline. The small basal ganglia approximate each other. Note the monoventricle communicating with a dorsal cyst .*

**Holoprosencephaly**
*Midline sagittal T1 MR shows both white & gray matter crossing midline anterior & posterior to the "dip" in the corpus callosum, where only gray matter traverses. This is a middle interhemispheric variant of holoprosencephaly (syntelencephaly).*

**Holoprosencephaly**
*Axial T1 MR in the same patient shows gray & white matter traversing the midline in the expected location of the splenium. Gray matter also protrudes into the ventricular system. The septum pellucidum is absent.*