---
title: "Adrenal Myelolipoma"
docid: "5813a554-06a4-4696-af71-7ce50693039d"
authors:
- key: "c3463c5c-31d3-4489-bbfe-6b895abdb86d"
value: "Mitchell Tublin, MD"
- key: "3d84d682-9451-4b02-99b2-e34970a5b440"
value: "Michael P. Federle, MD, FACR"
breadcrumbs:
-
name: "Genitourinary"
slug: "genitourinary"
treeNodeId: "bd0eb4fe-d465-4faa-a3b7-526e8f01802d"
-
name: "Diagnosis"
slug: "diagnosis"
treeNodeId: "e82a3e55-c0be-4ed1-acd6-b03ae9167c31"
-
name: "Adrenal"
slug: "adrenal"
treeNodeId: "d3b85dea-43cb-4be3-b103-902e38d0336e"
-
name: "Benign Neoplasms"
slug: "benign-neoplasms"
treeNodeId: "eeebc0ba-f71a-4ae6-8daf-525d0d18fa16"
-
name: "Adrenal Myelolipoma"
slug: "adrenal-myelolipoma"
treeNodeId: null
category: "Genitourinary"
documentVersionId: "20712ef4-2a32-41f1-913a-2a1e492778cd"
imageCount: 14
lastUpdated: "09/09/21"
pageDescription: "Adrenal Myelolipoma"
pageKeywords: "Genitourinary, Diagnosis, Adrenal, Benign Neoplasms, Adrenal Myelolipoma"
pageTitle: "Adrenal Myelolipoma | STATdx"
enhancedTitle: "Adrenal Myelolipoma"
type: "DX"
references: true
breadcrumbs:
- "Genitourinary"
- "Diagnosis"
- "Adrenal"
- "Benign Neoplasms"
- "Adrenal Myelolipoma"
---
# KEY FACTS
- ## Terminology
- Uncommon benign tumor composed of mature fat tissue and hematopoietic elements (myeloid and erythroid cells)
- ## Imaging
- Benign, nonfunctioning adrenal tumor
- Accounts for 7-15% of incidental adrenal masses, usually in older population
- Typically unilateral and very rarely bilateral
- Large tumors can mimic retroperitoneal lipomas, liposarcomas
- Asymptomatic, though larger tumors may hemorrhage
- CT
- Lesion containing fat attenuation (-30 to -90 HU)
- Usually well-defined mass with recognizable pseudocapsule (remaining adrenal)
- Punctate calcifications seen in 24% of cases
- Coronal reconstruction helpful to differentiate from exophytic renal angiomyolipoma
- MR
- Tumor with major fat component
- T1WI in phase: Typically hyperintense
- FS sequences: Loss of signal
- ## Top Differential Diagnoses
- Adrenal adenoma
- Intracellular lipid vs. macroscopic fat
- Adrenal metastases and lymphoma
- Retroperitoneal liposarcoma
- Involving perirenal space, may simulate adrenal (or renal) fatty tumor
- Pheochromocytoma
- Highly vascular, prone to hemorrhage and necrosis
- Adrenal carcinoma
- Renal angiomyelolipoma
- Coronal CT reconstruction or MR useful to determine organ of origin
# TERMINOLOGY
- ## Definitions
- Uncommon benign tumor composed of mature adipose tissue and hematopoietic elements
# IMAGING
- ## General Features
- ### Best diagnostic clue
- Suprarenal mass containing fat
- ### Location
- Suprarenal
- Rare extraadrenal myelolipomas (presacral, retroperitoneal)
- ### Size
- Usually 2-10 cm, rarely 10-20 cm
- Key concepts
- Benign neoplasm of adrenal gland
- Autopsy prevalence rate of 0.2-0.4%
- Accounts for 7-15% of adrenal "incidentalomas"
- Usually unilateral incidental finding in older patient
- Larger tumors can bleed spontaneously
- Most are nonfunctioning (do not secrete hormones)
- Large myelolipomas can mimic retroperitoneal lipoma or liposarcoma
- ## CT Findings
- CT appearance depends on histologic composition
- Most tumors are heterogeneous adrenal masses composed of varying percentages of fat
- Low-attenuation suprarenal lesion containing fat density (-30 to -90 HU)
- Average NECT attenuation value of tumor: -74 HU in one series
- Interspersed soft tissue attenuation components: Myeloid elements, hemorrhage
- Presence of macroscopic fat within tumor is diagnostic
- Punctate calcifications seen in 24% of cases
- Usually well-defined mass with recognizable pseudocapsule (remnant adrenal)
- Coronal reconstructions may help determine organ of origin: Adrenal myelolipoma vs. exophytic renal angiomyelolipoma
- ## MR Findings
- MR appearance depends on histologic composition
- Tumor with major fat component
- T1WI in phase: Typically hyperintense
- T1WI out phase: Persistent hyperintensity of macroscopic fat
- T1WI FS: Confirmatory suppression of signal
- Bone marrow elements (myeloid and erythroid cells)
- Low signal on T1WI, moderate signal on T2WI
- Hemorrhage: Varying T1, T2 signal depending on age of blood
- ## Ultrasonographic Findings
- ### Grayscale ultrasound
- Well-defined, echogenic mass (↑ fat tissue)
- Often overlooked: Lack of mass effect and isoechogenicity relative to retroperitoneal fat
- Heterogeneous mass (↑ myeloid cells)
- ## Angiographic Findings
- Conventional
- Differentiate myelolipoma from retroperitoneal liposarcoma by determining origin of blood supply and vascularity of tumors
- ## Nuclear Medicine Findings
- Typically not metabolically active, though uptake reported at FDG PET
- ## Imaging Recommendations
- Helical NECT or MR with FS sequence
# DIFFERENTIAL DIAGNOSIS
- [Adrenal Adenoma](/document/adrenal-adenoma/e2916d86-5f9f-4dd3-9576-1a7b89d8dda0)
- Lipid-rich adenoma: ↓ attenuation (< 10 HU) at NECT
- Can contain small amounts of macroscopic fat due to lipomatous metaplasia
- CECT: Washout 15 minutes post injection: > 50%
- Relative washout: > 40%
- Absolute washout: > 60%
- [Metastases and Lymphoma, Adrenal](/document/adrenal-lymphoma/44639c90-bd04-4e2a-a470-2c28a0e2ff78)
- Bilateral lesions: Clinical history paramount
- Metastases: Soft tissue attenuation (signal)
- Lymphoma: May maintain adreniform shape, adjacent retroperitoneal adenopathy
- [Liposarcoma, Retroperitoneal](/document/retroperitoneal-sarcoma/c1466b30-b730-41c4-a065-2c2de018a5f7)
- Retroperitoneal primary sarcoma involving perirenal space may simulate adrenal (or renal) fatty tumor
- [Pheochromocytoma](/document/pheochromocytoma/7d3c4062-643c-4030-8783-f85184ad8132)
- Highly vascular, prone to hemorrhage and necrosis
- Hyperintense on T2WI, bilateral in multiple endocrine neoplasia syndromes (MEN) syndromes
- Clinical history (labile hypertension) and urinary catecholamines
- [Adrenal Carcinoma](/document/adrenal-cortical-carcinoma/bdc7a08b-a64f-4bd2-9dfc-24331728e85e)
- Rare, unilateral, invasive, enhancing mass
- Venous invasion, distant metastases
- May contain fat: Engulfed retroperitoneal fat vs. lipomatous metaplasia
- ## Renal Angiomyelolipoma
- Exophytic upper pole angiomyolipoma may mimic
- Coronal reconstruction/MR helpful to determine organ of origin
# PATHOLOGY
- ## General Features
- ### Etiology
- Unknown
- Best hypothesis: Reticuloendothelial cell metaplasia of capillaries in adrenal (stress/infection/necrosis)
- Secondary hypothesis: Myelolipoma represents site of extramedullary hematopoiesis
- ### Associated abnormalities
- Adrenal collision tumors (coexistent myelolipoma and adenoma typical)
- Large, bilateral myelolipomas reported with longstanding, poorly treated congenital adrenal hyperplasia
- ## Gross Pathologic & Surgical Features
- Cut section: Fat, soft tissue components
- ## Microscopic Features
- Mature fat cells and megakaryocytes; no malignant cells
- Calcification
- Hemorrhage within larger lesions
# CLINICAL ISSUES
- ## Presentation
- ### Most common signs/symptoms
- Asymptomatic
- Usually incidental finding on CT, MR
- Typically biochemically nonfunctioning
- Symptomatic
- Acute abdomen: Flank pain due to rupture and hemorrhage
- Case reports of hormonally active tumors: Cushing, Conn syndromes, virilization
- Diagnosis: Pathognomonic MR/CT features
- Biopsy reserved for larger, atypical lesions, though prone to sampling error
- ## Demographics
- ### Age
- Usually older patients (50-70 years old)
- ### Epidemiology
- Autopsy incidence: 0.2-0.4%
- ## Natural History & Prognosis
- Complication: Rupture with hemorrhage (rare)
- Prognosis: Excellent
- ## Treatment
- When diagnosis is certain, surgery not needed for lesions < 5-7 cm
- Surgery reserved for larger, symptomatic, or atypical lesions
- Surgical series have confirmed utility of laparoscopic resection
# DIAGNOSTIC CHECKLIST
- ## Consider
- Differentiate from other tumors (lipid-rich adenoma)
- Key is presence of imaging-apparent adipose tissue; avoid further work-up for incidental mass
- ## Image Interpretation Pearls
- Well-defined, heterogeneous, fat-attenuation tumor on CT
- T1 hyperintense, signal loss with fat suppression
81ce3ad3-c446-4b08-8b87-df9511f95360
## References
# Selected References
1. [Alshahrani MA et al: Bilateral adrenal abnormalities: imaging review of different entities. Abdom Radiol (NY). 44(1):154-79, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=29938331%5Bpmid%5D)
1. [Schieda N et al: Renal and adrenal masses containing fat at MRI: proposed nomenclature by the society of abdominal radiology disease-focused panel on renal cell carcinoma. J Magn Reson Imaging. 49(4):917-26, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30693607%5Bpmid%5D)
1. [Decmann Á et al: Adrenal myelolipoma: a comprehensive review. Endocrine. 59(1):7-15, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=29164520%5Bpmid%5D)
1. [Campbell MJ et al: The radiographically diagnosed adrenal myelolipoma: what do we really know? Endocrine. 58(2):289-94, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=28866749%5Bpmid%5D)
1. [Farrugia FA et al: Radiology of the adrenal incidentalomas. Review of the literature. Endocr Regul. 51(1):35-51, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=28222025%5Bpmid%5D)
1. [Littrell LA et al: Extra-adrenal myelolipoma and extramedullary hematopoiesis: imaging features of two similar benign fat-containing presacral masses that may mimic liposarcoma. Eur J Radiol. 93:185-94, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=28668414%5Bpmid%5D)
1. [Mendiratta-Lala M et al: Adrenal imaging. Endocrinol Metab Clin North Am. 46(3):741-59, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=28760236%5Bpmid%5D)
1. [Tanner J et al: Case 243: extramedullary hematopoiesis in an adrenal myelolipoma. Radiology. 284(1):292-6, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=28628416%5Bpmid%5D)
1. [Shaaban AM et al: Fat-containing retroperitoneal lesions: imaging characteristics, localization, and differential diagnosis. Radiographics. 36(3):710-34, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27163589%5Bpmid%5D)
1. [Yin L et al: A 10-year single-center experience with surgical management of adrenal myelolipoma. J Endourol. 28(2):252-5, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24044410%5Bpmid%5D)
1. [Schieda N et al: Pitfalls of adrenal imaging with chemical shift MRI. Clin Radiol. 69(11):1186-97, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=25062926%5Bpmid%5D)
1. [Katabathina VS et al: Adrenal collision tumors and their mimics: multimodality imaging findings. Cancer Imaging. 13(4):602-10, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=24434021%5Bpmid%5D)
1. [Castinetti F et al: Adrenal myelolipoma: an unusual cause of bilateral highly 18F-FDG-avid adrenal masses. J Clin Endocrinol Metab. 97(8):2577-8, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22622025%5Bpmid%5D)
1. [Giacinto J et al: Nonoperative management of adrenal myelolipoma hemorrhage resulting from trauma. Am Surg. 78(11):E463-4, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=23089419%5Bpmid%5D)
1. [Su HC et al: Adrenal myelolipoma associated with hyperandrogenemia. Int J Urol. 19(11):1026-8, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22788680%5Bpmid%5D)
1. [German-Mena E et al: Adrenal myelolipomas in patients with congenital adrenal hyperplasia: review of the literature and a case report. Endocr Pract. 7(3):441-7, 2011](http://www.ncbi.nlm.nih.gov/pubmed/?term=21324823%5Bpmid%5D)
1. [Daneshmand S et al: Adrenal myelolipoma: diagnosis and management. Urol J. 3(2):71-4, 2006](http://www.ncbi.nlm.nih.gov/pubmed/?term=17590837%5Bpmid%5D)
1. [Kenney PJ et al: Myelolipoma: CT and pathologic features. Radiology. 208(1):87-95, 1998](http://www.ncbi.nlm.nih.gov/pubmed/?term=9646797%5Bpmid%5D)
1. [Rao P et al: Imaging and pathologic features of myelolipoma. Radiographics. 17(6):1373-85, 1997](http://www.ncbi.nlm.nih.gov/pubmed/?term=9397452%5Bpmid%5D)
1. [Cyran KM et al: Adrenal myelolipoma. AJR Am J Roentgenol. 166(2):395-400, 1996](http://www.ncbi.nlm.nih.gov/pubmed/?term=8553954%5Bpmid%5D)
## Images
### Selected Images
 . Even large myelolipomas may not be perceived on US given their isoechogenicity relative to retroperitoneal fat.](images/app.statdx.com_image_thumbnail_442ee7e1-12f4-4447-8770-c20bc2232943_size_168_quality_85_799db510_20251017T212346Z.jpg)
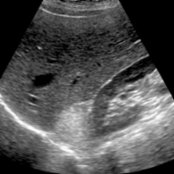
*Sagittal US in a 52-year-old woman with right upper quadrant pain shows a subtle, echogenic right suprarenal mass . Even large myelolipomas may not be perceived on US given their isoechogenicity relative to retroperitoneal fat.*
*Sagittal US in a 52-year-old woman with right upper quadrant pain shows a subtle, echogenic right suprarenal mass . Even large myelolipomas may not be perceived on US given their isoechogenicity relative to retroperitoneal fat.*
*Sagittal US in a 52-year-old woman with right upper quadrant pain shows a subtle, echogenic right suprarenal mass . Even large myelolipomas may not be perceived on US given their isoechogenicity relative to retroperitoneal fat.*

*Sagittal US in a 52-year-old woman with right upper quadrant pain shows a subtle, echogenic right suprarenal mass . Even large myelolipomas may not be perceived on US given their isoechogenicity relative to retroperitoneal fat.*
 . Macroscopic fat is the hallmark of myelolipomas, though the fat may be interspersed with soft tissue myeloid elements and hemorrhage.](images/app.statdx.com_image_thumbnail_7c5086cf-283b-4e1e-8a7c-72ba7a53567c_size_168_quality_85_6f2bf25a_20251017T212346Z.jpg)
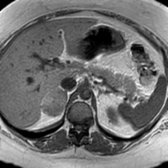
*Axial CECT in the same patient shows a fat-attenuation right adrenal lesion . Macroscopic fat is the hallmark of myelolipomas, though the fat may be interspersed with soft tissue myeloid elements and hemorrhage.*
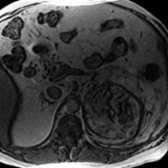
*Axial T1 MR for follow-up in the same patient shows a relatively intense right adrenal lesion . No significant signal loss was shown on out-phase imaging (not shown).*

*Axial CECT in the same patient shows a fat-attenuation right adrenal lesion . Macroscopic fat is the hallmark of myelolipomas, though the fat may be interspersed with soft tissue myeloid elements and hemorrhage.*

*Axial T1 MR for follow-up in the same patient shows a relatively intense right adrenal lesion . No significant signal loss was shown on out-phase imaging (not shown).*
 is composed of fat, a finding pathognomonic of a myelolipoma. Signal suppression with fat saturation and persistent signal on out-of-phase imaging indicate macroscopic fat, rather than the intracellular lipid characteristic of adrenal adenomas.](images/app.statdx.com_image_thumbnail_ae78b57e-1386-42d6-a184-15212a61ccc5_size_168_quality_85_c4020638_20251017T212346Z.jpg)
*Axial T1 FS MR in the same patient confirms that the right adrenal lesion is composed of fat, a finding pathognomonic of a myelolipoma. Signal suppression with fat saturation and persistent signal on out-of-phase imaging indicate macroscopic fat, rather than the intracellular lipid characteristic of adrenal adenomas.*

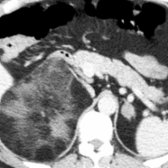
*Axial CECT in a 55-year-old man with left flank pain shows a large, fat-attenuation mass , soft tissue attenuation rim, and perinephric infiltration.*
*Axial out-of-phase MR in the same patient shows a low-signal rim (due to hemosiderin) and perinephric infiltration. Most myelolipomas are asymptomatic, but larger tumors may hemorrhage, as in this case. Adrenalectomy was performed given the large size of the tumor and evidence of repeated hemorrhage.*

*Axial CECT in a 53-year-old man shows an incidental myelolipoma containing calcifications .*

*Coronal NECT in a 71-year-old man with left flank pain shows an incidental collision tumor composed of a myelolipoma and an adenoma .*

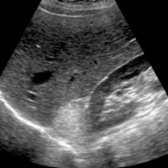
*Sagittal US in a 44-year-old woman with abdominal pain shows a large, echogenic suprarenal mass that displaces the kidney . CT was recommended given the size of the lesion.*

*Axial CECT in the same patient confirms a fat-attenuation suprarenal mass . Extrarenal angiomyolipoma was ultimately resected. The differential diagnosis of large myelolipomas includes retroperitoneal liposarcomas, angiomyolipomas, and adrenal carcinomas with lipomatous metaplasia.*
### Additional Images

*Axial CECT shows a heterogeneous, predominantly fatty right adrenal mass with calcified foci.*

*Axial CECT shows a predominantly fatty left adrenal mass.*

*Axial chemical shift (opposed-phase) MR shows a heterogeneous right adrenal mass with signal loss at fat/soft tissue interfaces.*
*Axial CECT shows a large, heterogeneous fatty myelolipoma in the right adrenal gland and an adenoma in the left adrenal gland.*
is composed of fat, a finding pathognomonic of a myelolipoma. Signal suppression with fat saturation and persistent signal on out-of-phase imaging indicate macroscopic fat, rather than the intracellular lipid characteristic of adrenal adenomas.](images/app.statdx.com_image_thumbnail_ae78b57e-1386-42d6-a184-15212a61ccc5_size_168_quality_85_c4020638_20251017T212346Z.jpg)
*Axial T1 FS MR in the same patient confirms that the right adrenal lesion is composed of fat, a finding pathognomonic of a myelolipoma. Signal suppression with fat saturation and persistent signal on out-of-phase imaging indicate macroscopic fat, rather than the intracellular lipid characteristic of adrenal adenomas.*

*Axial CECT in a 55-year-old man with left flank pain shows a large, fat-attenuation mass , soft tissue attenuation rim, and perinephric infiltration.*

*Axial out-of-phase MR in the same patient shows a low-signal rim (due to hemosiderin) and perinephric infiltration. Most myelolipomas are asymptomatic, but larger tumors may hemorrhage, as in this case. Adrenalectomy was performed given the large size of the tumor and evidence of repeated hemorrhage.*

*Axial CECT in a 53-year-old man shows an incidental myelolipoma containing calcifications .*

*Coronal NECT in a 71-year-old man with left flank pain shows an incidental collision tumor composed of a myelolipoma and an adenoma .*

*Sagittal US in a 44-year-old woman with abdominal pain shows a large, echogenic suprarenal mass that displaces the kidney . CT was recommended given the size of the lesion.*

*Axial CECT in the same patient confirms a fat-attenuation suprarenal mass . Extrarenal angiomyolipoma was ultimately resected. The differential diagnosis of large myelolipomas includes retroperitoneal liposarcomas, angiomyolipomas, and adrenal carcinomas with lipomatous metaplasia.*
### Additional Images

*Axial CECT shows a heterogeneous, predominantly fatty right adrenal mass with calcified foci.*

*Axial CECT shows a predominantly fatty left adrenal mass.*

*Axial chemical shift (opposed-phase) MR shows a heterogeneous right adrenal mass with signal loss at fat/soft tissue interfaces.*

*Axial CECT shows a large, heterogeneous fatty myelolipoma in the right adrenal gland and an adenoma in the left adrenal gland.*