---
title: "Brain Tumor in Newborn/Infant"
docid: "12b32579-c99b-41c0-95fd-f2ad1fc4a4fd"
authors:
- key: "f184750a-90b4-47a7-907b-23b05d70357a"
value: "Chang Yueh Ho, MD"
breadcrumbs:
-
name: "Brain"
slug: "brain"
treeNodeId: "6d8829f1-14d7-45af-8675-255189aa526a"
-
name: "Differential Diagnosis"
slug: "differential-diagnosis"
treeNodeId: "a7fdd139-664e-4bb8-8d18-400e4733ff60"
-
name: "Brain Parenchyma, General"
slug: "brain-parenchyma-general"
treeNodeId: "e79be97b-28c0-4023-be87-334c0579d35d"
-
name: "Clinically Based Differentials"
slug: "clinically-based-differentials"
treeNodeId: "108519f7-93d7-4662-85dd-2239f2422821"
-
name: "Brain Tumor in Newborn/Infant"
slug: "brain-tumor-in-newborninfant"
treeNodeId: null
category: "Brain"
documentVersionId: "6d309907-eb33-42ec-abac-50970b8269ba"
imageCount: 71
lastUpdated: "01/25/23"
pageDescription: "Brain Tumor in Newborn/Infant"
pageKeywords: "Brain, Differential Diagnosis, Brain Parenchyma, General, Clinically Based Differentials, Brain Tumor in Newborn/Infant"
pageTitle: "Brain Tumor in Newborn/Infant | STATdx"
enhancedTitle: "Brain Tumor in Newborn/Infant"
type: "DDX"
references: true
breadcrumbs:
- "Brain"
- "Differential Diagnosis"
- "Brain Parenchyma, General"
- "Clinically Based Differentials"
- "Brain Tumor in Newborn/Infant"
---
# ESSENTIAL INFORMATION
- ## Key Differential Diagnosis Issues
- Newborn/infant brain tumors
- Typically large, bulky, inhomogeneous
- 60-70% supratentorial
- Infratentorial more common in older children
- Immature, high-grade tumors more common
- ## Helpful Clues for Common Diagnoses
- **Teratoma**
- Most common fetal and congenital brain tumor
- Midline, supratentorial
- Small, lobular or holocranial
- Contents
- Ca⁺⁺, cysts
- Fat in mature teratoma, less commonly in immature teratoma; enhancing soft tissue
- Look for associated congenital brain anomalies
- **Infant-Type Hemispheric Glioma**
- Large, heterogeneous, hemispheric
- High-grade cellular astrocytoma
- Better outcome than other histone-associated pediatric high-grade gliomas
- **Medulloblastoma**
- SHH-activated and non-WNT/non-SHH (group 3) more common in infants
- Posterior fossa mass with hydrocephalus
- Restricts on DWI (best MR clue)
- Enhancement usual (may be late/slow)
- Sparse Ca⁺⁺: ~ 20%; hemorrhage rare
- Hypercellularity reflected on imaging
- Hyperdense (NECT), hypointense (T2)
- SHH-activated
- Cerebellar hemisphere, not centered in 4th ventricle
- Intense enhancement
- Additional *TP53* mutation carries poor prognosis
- Group 3
- Classic 4th ventricular location
- Enhancement common, group 4 has less enhancement
- Poor prognosis when presenting with dissemination
- **Ependymoma,****Posterior Fossa Type A**
- Posterior fossa A ependymomas characterized by ↓ H3 K27 expression
- Younger children, poor outcome
- Lateral in 4th ventricle, extends through foramina of Luschka
- Heterogeneous enhancement
- Ca⁺⁺ ± hemorrhage
- **Supratentorial Ependymoma**
- Periventricular/extraventricular > intraventricular
- Derived from periventricular ependymal rests
- Large, bulky; Ca⁺⁺: ~ 50%
- Variable necrosis, hemorrhage
- *ZFTA* fusion-positive: Seen in infants and older children, poor prognosis
- *YAP1* fusion-positive: Usually seen in infants, good prognosis
- **Choroid Plexus Papilloma**
- Choroid plexus papilloma (CPP): Lobulated intraventricular mass
- Lateral > 4th > 3rd
- NECT: Isointense to dense
- Isointense to slightly hyperintense on T2WI
- Vividly enhancing
- Hydrocephalus common
- ## Helpful Clues for Less Common Diagnoses
- **Pilocytic Astrocytoma, Pilomyxoid Variant**
- Younger age presentation than typical pilocytic astrocytoma (PA)
- Often presents as large, enhancing, infiltrative mass involving optic pathway
- Despite low-grade tumor, it can have leptomeningeal seeding
- **Atypical Teratoid-Rhabdoid Tumor**
- Medulloblastoma-like, +
- Metastases at diagnosis more common
- Cysts, hemorrhage more common
- Variable contrast enhancement
- Cerebellopontine angle cistern location more common
- Seeding via CSF pathway common
- **CNS Embryonal Tumor**
- Previously primitive neuroectodermal tumor (PNET)
- Large, complex mass
- Restricts on DWI
- Heterogeneous signal enhancement
- Ca⁺⁺ more common than in posterior fossa PNETs
- Hemorrhage, necrosis common
- Hemispheric
- Mean diameter: 5 cm
- Especially newborn/infants
- Minimal peritumoral edema
- Suprasellar: Early neuroendocrine, visual disturbances
- **Desmoplastic Infantile Ganglioglioma/Astrocytoma**
- Desmoplastic infantile gangliogliomas(DIGs)/astrocytoma often have large cyst
- Cortically based, enhancing tumor nodule
- Enhancing adjacent pia and dura; low grade
- Good outcome with complete surgical resection
- ## Helpful Clues for Rare Diagnoses
- **Choroid Plexus Carcinoma**
- Similar to CPP, +
- Brain invasion; Ca⁺⁺, cysts, bleed
- Ependymal, subarachnoid space seeding (can be seen with both CPP, choroid plexus carcinoma)
- **Embryonal Tumor With Multilayered Rosettes**
- Rare malignant embryonal brain tumor
- Young children (< 5 years)
- Histologic differentiation varies
- Neuronal, astrocytic, ependymal, melanotic, etc.
- Imaging appearance reflects variable differentiation
- Medulloepithelioma, ependymoblastoma, and embryonal tumor with abundant neuropil and true rosettes (ETANTR) all have similar molecular features and are grouped as embryonal tumor with multilayered rosettes (ETMR)
- **Neurocutaneous Melanosis (Melanoma/Melanocytoma)**
- Giant or multiple cutaneous melanocytic nevi, +
- Melanosis: Bright T1 lesions in amygdala, cerebellum without fat saturation
- T2 hypointense to isointense, no enhancement
- Melanoma: Melanosis + diffuse leptomeningeal enhancement
- Degeneration into malignant melanoma common
## References
# Selected References
1. [Louis DN et al: The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 23(8):1231-51, 2021](http://www.ncbi.nlm.nih.gov/pubmed/?term=34185076%5Bpmid%5D)
1. [Clarke M et al: Infant high-grade gliomas comprise multiple subgroups characterized by novel targetable gene fusions and favorable outcomes. Cancer Discov. 10(7):942-63, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=32238360%5Bpmid%5D)
1. [Lambo S et al: ETMR: a tumor entity in its infancy. Acta Neuropathol. 140(3):249-66, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=32601913%5Bpmid%5D)
1. [Gessi M et al: Medulloblastoma with extensive nodularity: a tumor exclusively of infancy? Neuropathol Appl Neurobiol. 43(3):267-70, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=26990710%5Bpmid%5D)
1. [Shekdar KV et al: Brain tumors in the neonate. Neuroimaging Clin N Am. 27(1):69-83, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=27889024%5Bpmid%5D)
1. [Munjal S et al: Infant brain tumours: a tale of two cities. Childs Nerv Syst. 32(9):1633-40, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27299432%5Bpmid%5D)
1. [Kralik SF et al: Diffusion imaging for tumor grading of supratentorial brain tumors in the first year of life. AJNR Am J Neuroradiol. 35(4):815-23, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24200900%5Bpmid%5D)
## Images
### Selected Images
 in a neonate with maximal hydrocephalus and layering blood products
in a neonate with maximal hydrocephalus and layering blood products  as well as cellular debris
as well as cellular debris  .](images/app.statdx.com_image_thumbnail_e9986857-8a55-4f23-bb55-fe7c4110e35f_size_168_quality_85_cf9d7859_20251014T202907Z.jpg)
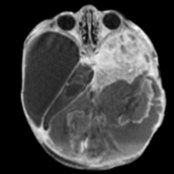
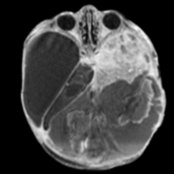
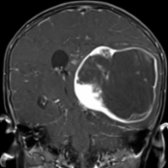
**Teratoma**
*Axial T1 C+ MR shows a large, enhancing mass in a temporal off-midline location in a neonate with maximal hydrocephalus and layering blood products as well as cellular debris .*
**Teratoma**
*Axial T1 C+ MR shows a large, enhancing mass in a temporal off-midline location in a neonate with maximal hydrocephalus and layering blood products as well as cellular debris .*
**Teratoma**
*Axial T1 C+ MR shows a large, enhancing mass in a temporal off-midline location in a neonate with maximal hydrocephalus and layering blood products as well as cellular debris .*

**Teratoma**
*Axial T1 C+ MR shows a large, enhancing mass in a temporal off-midline location in a neonate with maximal hydrocephalus and layering blood products as well as cellular debris .*

**Teratoma**
*Coronal T2 MR shows the heterogeneous mass in the left middle cranial fossa with severe hydrocephalus and a thinned brain mantle . Fetal teratomas often have poor outcome due to compression of the brain.*

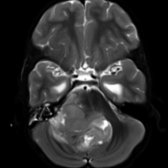
**Infant-Type Hemispheric Glioma**
*Axial T2 MR shows a large, heterogeneous mass with central necrosis and blood products causing midline shift and hydrocephalus .*

**Infant-Type Hemispheric Glioma**
*Axial T1 C+ MR shows heterogeneous enhancement of the large left frontal lobe. In an infant, this is consistent with an infant-type hemispheric glioma, a high-grade tumor characterized by NTRK, ROS1, ALK, or MET alteration of tyrosine kinases.*
**Medulloblastoma**
*Axial T1 C+ MR shows multiple nodules in the right middle cerebellar peduncle and vermis in an infant. This was an SHH desmoplastic medulloblastoma. Desmoplastic histology is associated with SHH pathway alteration and can be nodular in appearance.*

**Medulloblastoma**
*Axial b=1000 DWI MR shows the nodular masses have decreased diffusion compatible with high-grade neoplasm. SHH medulloblastomas have variable outcomes with a TP53 mutation associated with poor outcome.*
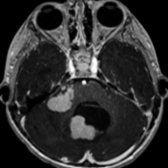
**Ependymoma, Posterior Fossa Type A**
*Axial T2 MR shows a heterogeneous mass in the 4th ventricle extending laterally through the left foramen of Luschka . This was a posterior fossa type A (PFA) ependymoma at resection. Ependymomas have a "toothpaste" propensity to extend through the 4th ventricular foramina.*

**Ependymoma, Posterior Fossa Type A**
*Axial T1 C+ MR shows the heterogeneous enhancement of the PFA ependymoma. PFA ependymomas tend to occur in young children and carry a worse prognosis than posterior fossa type B (PFB) ependymomas.*

**Supratentorial Ependymoma**
*Axial T2 TSE FS MR shows a heterogeneous mass in a periventricular location . Supratentorial ependymomas are thought to arise from periventricular ependymal rests.*

**Supratentorial Ependymoma**
*Axial T1 C+ MR shows cystic and heterogeneous enhancement in this ZFTA fusion supratentorial ependymoma. This subtype has a worse prognosis than the more rare YAP1 subgroup, which tends to present in younger children.*

**Choroid Plexus Papilloma**
*Axial T2 MR shows a large intraventricular mass coinciding with the left lateral choroid plexus glomus . The mass has decreased T2 signal, which may represent Ca⁺⁺ or blood products. There is obstructive hydrocephalus, which is common in choroid plexus tumors.*

**Choroid Plexus Papilloma**
*Coronal T1 C+ MR shows a heterogeneous, lobular, enhancing mass in the left lateral ventricle causing obstructive hydrocephalus. At resection, there was an atypical choroid plexus papilloma (CPP), WHO grade 2.*
**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Coronal T1 C+ MR shows a large left hemispheric mass with solid enhancement centrally and cystic component peripherally. Pilomyxoid variant of pilocytic astrocytomas may present in younger patients, involve the optic pathway, and are more locally aggressive.*

**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Axial T2 MR shows the mass centered in the central gray nuclei with midline shift . The solid component has relative increased T2 content , suggesting a low-grade neoplasm.*

**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Axial b=1000 DWI MR shows increased diffusion of the solid tumor portions , consistent with the low-grade nature of pilomyxoid astrocytoma. In infants, DWI is helpful in differentiating high- vs. low-grade tumors that tend to be large, heterogeneous, and hemispheric.*
**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T1 C+ MR shows 3 nodular masses in the posterior fossa within the cisterna magna , 4th ventricle , and premedullary cistern .*

**Atypical Teratoid-Rhabdoid Tumor**
*Axial b=1000 DWI shows the multiple posterior fossa masses have decreased diffusion compatible with high-grade neoplasm. Consider atypical teratoid-rhabdoid tumor in infants.*

**CNS Embryonal Tumor**
*Axial b=1000 DWI shows the peripheral solid component has decreased diffusion consistent with a hypercellular high-grade tumor . CNS embryonal tumors were previously termed primitive neuroectodermal tumors (PNETs).*

**CNS Embryonal Tumor**
*Axial T1 C+ MR shows a large left hemispheric mass with a large central proteinaceous cyst with intrinsic T1 shortening . The solid peripheral component has minimal enhancement .*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial T1 C+ MR shows a heterogeneous mass with solid enhancement peripherally with a broad dural base and cysts medially in an infant. Desmoplastic infantile tumors have a broad dural base as a characteristic appearance.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial T2 TSE MR shows the solid component has a hypointense appearance .*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial b=1000 DWI MR shows the solid components do not have decreased diffusion , correlating with the low-grade nature of this tumor. Infants that have a complete resection have a good outcome.*

**Choroid Plexus Carcinoma**
*Axial T1 C+ MR shows a large, heterogeneous mass centered in the left atria of the lateral ventricle , consistent with a choroid plexus tumor. This was a carcinoma at resection.*

**Choroid Plexus Carcinoma**
*Axial T2 TSE MR shows the large, isointense lateral ventricular mass. Radiographic size, invasion, and dissemination are not helpful to distinguish between a low-grade papilloma and a high-grade carcinoma. Carcinomas have a propensity to present in younger children.*

**Embryonal Tumor With Multilayered Rosettes**
*Axial T2 MR demonstrates a homogeneous cortical mass in a young child presenting with seizures. A dysembryoplastic neuroepithelial tumor (DNET) was the favored differential, but this was an embryonal tumor with multilayered rosettes (ETMR) at resection.*

**Embryonal Tumor With Multilayered Rosettes**
*Axial ADC map shows an area of decreased diffusion within the cortically based tumor, consistent with a high-grade neoplasm. ETMR is typically an aggressive and large high-grade tumor, with this tumor having an atypical early presentation.*

**Neurocutaneous Melanosis (Melanoma/Melanocytoma)**
*Coronal T1 MR in this neonate with large segmental cutaneous nevus shows an area of intrinsic T1 shortening in the left cerebellum , consistent with neurocutaneous melanosis.*

**Neurocutaneous Melanosis (Melanoma/Melanocytoma)**
*Coronal T1 C+ MR shows 2 masses in the amygdala with intrinsic T1 shortening compared to precontrast T1 (not shown). Amygdala involvement is a common location for neurocutaneous melanosis.*
### Additional Images
**Teratoma**
*Axial T1 C+ MR shows a large, enhancing mass in a temporal off-midline location in a neonate with maximal hydrocephalus and layering blood products as well as cellular debris .*

**Teratoma**
*Axial T1 C+ MR shows a large, enhancing mass in a temporal off-midline location in a neonate with maximal hydrocephalus and layering blood products as well as cellular debris .*

**Teratoma**
*Axial T1 C+ MR shows a large, enhancing mass in a temporal off-midline location in a neonate with maximal hydrocephalus and layering blood products as well as cellular debris .*

**Teratoma**
*Axial T1 C+ MR shows a large, enhancing mass in a temporal off-midline location in a neonate with maximal hydrocephalus and layering blood products as well as cellular debris .*

**Teratoma**
*Coronal T2 MR shows the heterogeneous mass in the left middle cranial fossa with severe hydrocephalus and a thinned brain mantle . Fetal teratomas often have poor outcome due to compression of the brain.*

**Infant-Type Hemispheric Glioma**
*Axial T2 MR shows a large, heterogeneous mass with central necrosis and blood products causing midline shift and hydrocephalus .*

**Infant-Type Hemispheric Glioma**
*Axial T1 C+ MR shows heterogeneous enhancement of the large left frontal lobe. In an infant, this is consistent with an infant-type hemispheric glioma, a high-grade tumor characterized by NTRK, ROS1, ALK, or MET alteration of tyrosine kinases.*

**Medulloblastoma**
*Axial T1 C+ MR shows multiple nodules in the right middle cerebellar peduncle and vermis in an infant. This was an SHH desmoplastic medulloblastoma. Desmoplastic histology is associated with SHH pathway alteration and can be nodular in appearance.*

**Medulloblastoma**
*Axial b=1000 DWI MR shows the nodular masses have decreased diffusion compatible with high-grade neoplasm. SHH medulloblastomas have variable outcomes with a TP53 mutation associated with poor outcome.*

**Ependymoma, Posterior Fossa Type A**
*Axial T2 MR shows a heterogeneous mass in the 4th ventricle extending laterally through the left foramen of Luschka . This was a posterior fossa type A (PFA) ependymoma at resection. Ependymomas have a "toothpaste" propensity to extend through the 4th ventricular foramina.*

**Ependymoma, Posterior Fossa Type A**
*Axial T1 C+ MR shows the heterogeneous enhancement of the PFA ependymoma. PFA ependymomas tend to occur in young children and carry a worse prognosis than posterior fossa type B (PFB) ependymomas.*

**Supratentorial Ependymoma**
*Axial T2 TSE FS MR shows a heterogeneous mass in a periventricular location . Supratentorial ependymomas are thought to arise from periventricular ependymal rests.*

**Supratentorial Ependymoma**
*Axial T1 C+ MR shows cystic and heterogeneous enhancement in this ZFTA fusion supratentorial ependymoma. This subtype has a worse prognosis than the more rare YAP1 subgroup, which tends to present in younger children.*

**Choroid Plexus Papilloma**
*Axial T2 MR shows a large intraventricular mass coinciding with the left lateral choroid plexus glomus . The mass has decreased T2 signal, which may represent Ca⁺⁺ or blood products. There is obstructive hydrocephalus, which is common in choroid plexus tumors.*

**Choroid Plexus Papilloma**
*Coronal T1 C+ MR shows a heterogeneous, lobular, enhancing mass in the left lateral ventricle causing obstructive hydrocephalus. At resection, there was an atypical choroid plexus papilloma (CPP), WHO grade 2.*

**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Coronal T1 C+ MR shows a large left hemispheric mass with solid enhancement centrally and cystic component peripherally. Pilomyxoid variant of pilocytic astrocytomas may present in younger patients, involve the optic pathway, and are more locally aggressive.*

**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Axial T2 MR shows the mass centered in the central gray nuclei with midline shift . The solid component has relative increased T2 content , suggesting a low-grade neoplasm.*

**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Axial b=1000 DWI MR shows increased diffusion of the solid tumor portions , consistent with the low-grade nature of pilomyxoid astrocytoma. In infants, DWI is helpful in differentiating high- vs. low-grade tumors that tend to be large, heterogeneous, and hemispheric.*

**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T1 C+ MR shows 3 nodular masses in the posterior fossa within the cisterna magna , 4th ventricle , and premedullary cistern .*

**Atypical Teratoid-Rhabdoid Tumor**
*Axial b=1000 DWI shows the multiple posterior fossa masses have decreased diffusion compatible with high-grade neoplasm. Consider atypical teratoid-rhabdoid tumor in infants.*

**CNS Embryonal Tumor**
*Axial b=1000 DWI shows the peripheral solid component has decreased diffusion consistent with a hypercellular high-grade tumor . CNS embryonal tumors were previously termed primitive neuroectodermal tumors (PNETs).*

**CNS Embryonal Tumor**
*Axial T1 C+ MR shows a large left hemispheric mass with a large central proteinaceous cyst with intrinsic T1 shortening . The solid peripheral component has minimal enhancement .*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial T1 C+ MR shows a heterogeneous mass with solid enhancement peripherally with a broad dural base and cysts medially in an infant. Desmoplastic infantile tumors have a broad dural base as a characteristic appearance.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial T2 TSE MR shows the solid component has a hypointense appearance .*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial b=1000 DWI MR shows the solid components do not have decreased diffusion , correlating with the low-grade nature of this tumor. Infants that have a complete resection have a good outcome.*

**Choroid Plexus Carcinoma**
*Axial T1 C+ MR shows a large, heterogeneous mass centered in the left atria of the lateral ventricle , consistent with a choroid plexus tumor. This was a carcinoma at resection.*

**Choroid Plexus Carcinoma**
*Axial T2 TSE MR shows the large, isointense lateral ventricular mass. Radiographic size, invasion, and dissemination are not helpful to distinguish between a low-grade papilloma and a high-grade carcinoma. Carcinomas have a propensity to present in younger children.*

**Embryonal Tumor With Multilayered Rosettes**
*Axial T2 MR demonstrates a homogeneous cortical mass in a young child presenting with seizures. A dysembryoplastic neuroepithelial tumor (DNET) was the favored differential, but this was an embryonal tumor with multilayered rosettes (ETMR) at resection.*

**Embryonal Tumor With Multilayered Rosettes**
*Axial ADC map shows an area of decreased diffusion within the cortically based tumor, consistent with a high-grade neoplasm. ETMR is typically an aggressive and large high-grade tumor, with this tumor having an atypical early presentation.*

**Neurocutaneous Melanosis (Melanoma/Melanocytoma)**
*Coronal T1 MR in this neonate with large segmental cutaneous nevus shows an area of intrinsic T1 shortening in the left cerebellum , consistent with neurocutaneous melanosis.*

**Neurocutaneous Melanosis (Melanoma/Melanocytoma)**
*Coronal T1 C+ MR shows 2 masses in the amygdala with intrinsic T1 shortening compared to precontrast T1 (not shown). Amygdala involvement is a common location for neurocutaneous melanosis.*
### Additional Images
 scattered throughout the lesion.](80c8cb35-b67f-44a8-8914-e9501e1ff3c3)
**Teratoma**
*Axial T1 MR in this 7-day-old infant shows T1-bright signal from fat scattered throughout the lesion.*

**Teratoma**
*Axial T1 MR in this 7-day-old infant shows T1-bright signal from fat scattered throughout the lesion.*
 , solid tissue , and calcification
, solid tissue , and calcification  .](f8ea3a8c-397a-4c6c-b1e7-46d4392d1af9)
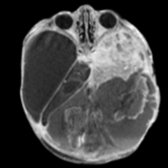
**Teratoma**
*Axial NECT in the same child at 15 months old shows a complicated pineal region mass consisting of fat , solid tissue , and calcification .*

**Teratoma**
*Axial NECT in the same child at 15 months old shows a complicated pineal region mass consisting of fat , solid tissue , and calcification .*
 that fills the posterior fossa. Note peripheral myxoid or cystic tumor components .](cbf02da7-2d98-4d58-a930-d740148699f1)
**Medulloblastoma**
*Axial CECT in a 1-year-old infant with macrocrania and vomiting shows a giant enhancing posterior fossa mass that fills the posterior fossa. Note peripheral myxoid or cystic tumor components .*

**Medulloblastoma**
*Axial T2 MR in a 10-month-old shows a giant isointense posterior fossa mass with distinct, thick, nodular morphology . PNET-medulloblastoma with extensive nodularity, a subtype of medulloblastoma, has a somewhat better prognosis.*

**Medulloblastoma**
*Axial T2 MR in a 4-month-old shows an intermediate- to low-signal mass that splays and encases posterior communicating and superior cerebellar arteries.*

**Medulloblastoma**
*Axial DWI MR shows diffusion restriction in this tumor involving mesencephalon, circummesencephalic cistern, and mesial temporal lobe.*

**Medulloblastoma**
*Coronal T1 C+ MR in this 10-month-old shows grape-like nodular enhancement . Medulloblastoma with extensive nodularity is a PNET-medulloblastoma variant that has somewhat better prognosis.*

**Supratentorial Ependymoma**
*Axial T2 MR in a 12-week-old infant shows a mixed heterogeneity left temporal lobe mass.*

**Supratentorial Ependymoma**
*Axial T2* GRE MR shows multifocal hemosiderin and calcific foci .*

**Choroid Plexus Papilloma**
*Coronal T1 C+ MR shows bilateral choroid plexus papillomas. The left is bulky and frond-like, while the right is stretched by the associated cyst.*

**Medulloblastoma**
*Axial CECT in a 1-year-old infant with macrocrania and vomiting shows a giant enhancing posterior fossa mass that fills the posterior fossa. Note peripheral myxoid or cystic tumor components .*

**Medulloblastoma**
*Axial T2 MR in a 10-month-old shows a giant isointense posterior fossa mass with distinct, thick, nodular morphology . PNET-medulloblastoma with extensive nodularity, a subtype of medulloblastoma, has a somewhat better prognosis.*

**Medulloblastoma**
*Axial T2 MR in a 4-month-old shows an intermediate- to low-signal mass that splays and encases posterior communicating and superior cerebellar arteries.*

**Medulloblastoma**
*Axial DWI MR shows diffusion restriction in this tumor involving mesencephalon, circummesencephalic cistern, and mesial temporal lobe.*

**Medulloblastoma**
*Coronal T1 C+ MR in this 10-month-old shows grape-like nodular enhancement . Medulloblastoma with extensive nodularity is a PNET-medulloblastoma variant that has somewhat better prognosis.*

**Supratentorial Ependymoma**
*Axial T2 MR in a 12-week-old infant shows a mixed heterogeneity left temporal lobe mass.*

**Supratentorial Ependymoma**
*Axial T2* GRE MR shows multifocal hemosiderin and calcific foci .*

**Choroid Plexus Papilloma**
*Coronal T1 C+ MR shows bilateral choroid plexus papillomas. The left is bulky and frond-like, while the right is stretched by the associated cyst.*
 , coloboma , and temporal lobe subependymal heterotopia in a 4-day-old girl with Aicardi syndrome.](790089eb-201f-4ff7-924d-7cd43d00d488)
**Choroid Plexus Papilloma**
*Axial T2 MR shows a large cyst , coloboma , and temporal lobe subependymal heterotopia in a 4-day-old girl with Aicardi syndrome.*

**Supratentorial Ependymoma**
*Sagittal ultrasound shows a bulky subependymal giant cell astrocytoma at the foramen of Monro in this newborn with cardiac rhabdomyoma and tuberous sclerosis. There are multiple additional tubers on the same image.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Coronal T1 C+ MR in a 7-month-old infant shows a massive right frontal cystic tumor with a solid enhancing component that involves the medial frontal cortex and falx.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial DWI MR shows a lack of diffusion restriction in the medial cortical tumor rind , which enhanced following contrast administration in this infant (not shown).*

**Choroid Plexus Papilloma**
*Axial T2 MR shows a large cyst , coloboma , and temporal lobe subependymal heterotopia in a 4-day-old girl with Aicardi syndrome.*

**Supratentorial Ependymoma**
*Sagittal ultrasound shows a bulky subependymal giant cell astrocytoma at the foramen of Monro in this newborn with cardiac rhabdomyoma and tuberous sclerosis. There are multiple additional tubers on the same image.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Coronal T1 C+ MR in a 7-month-old infant shows a massive right frontal cystic tumor with a solid enhancing component that involves the medial frontal cortex and falx.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial DWI MR shows a lack of diffusion restriction in the medial cortical tumor rind , which enhanced following contrast administration in this infant (not shown).*
 .](a7f4ea18-34f8-4e08-8ceb-695f627b70b1)
**Choroid Plexus Carcinoma**
*Axial T1 C+ MR in this 9-month-old infant shows a large, bulky, avidly enhancing left intraventricular tumor with invasion of the overlying brain . There are multiple intraventricular metastases .*

**Choroid Plexus Carcinoma**
*AP angiography performed as a part of preoperative embolization shows hypervascularity and multiple areas of contrast puddling .*

**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T2 MR in this 7-month-old infant shows hydrocephalus and a complicated solid and cystic tumor filling the 4th ventricle, supravermian cistern, and extending through the tentorial incisura .*

**Atypical Teratoid-Rhabdoid Tumor**
*Coronal T1 C+ MR in the same 7-month-old shows a right frontal metastatic deposit .*

**Neurocutaneous Melanosis (Melanoma/Melanocytoma)**
*Sagittal T1 MR shows increased signal intensity of the hippocampus in this 10-month-old with a large cutaneous nevus. Pachymeningeal thickening is present prior to contrast administration.*

**Embryonal Tumor With Multilayered Rosettes**
*Sagittal T1 MR in a 5-day-old infant shows a massive hemorrhagic tumor replacing and expanding the upper cervical spinal cord, the brainstem, and the cerebellum. The tumor protrudes through the incisura and displaces the straight sinus .*

**Embryonal Tumor With Multilayered Rosettes**
*Axial T2 MR shows a well-circumscribed, heterogeneous mass asymmetrically expanding the pons and the right middle cerebellar peduncle.*

**Embryonal Tumor With Multilayered Rosettes**
*Axial DWI of the well-circumscribed pontine tumor shows intense increased signal from decreased diffusion, suggesting this is a high-grade neoplasm. Medulloepithelioma is a highly primitive and aggressive tumor with a dismal prognosis.*

**Atypical Teratoid-Rhabdoid Tumor**
*Axial T1 C+ MR shows heterogeneous enhancement of the cerebellopontine angle tumor. Posterior fossa atypical teratoid-rhabdoid tumors can be difficult to distinguish from medulloblastomas, and both high-grade tumors have decreased diffusion.*

**Atypical Teratoid-Rhabdoid Tumor**
*Axial T2 MR shows a heterogeneous mass with cystic change and low T2 signal in the left cerebellopontine angle with invasion into the left internal auditory canal .*

**Choroid Plexus Carcinoma**
*Axial T1 C+ MR shows heterogeneous enhancement of the large intraventricular mass. While hemorrhage and parenchymal invasion are more likely with choroid plexus carcinoma, no particular imaging sign is able to specifically differentiate a papilloma from a carcinoma.*

**Choroid Plexus Carcinoma**
*Axial T2 MR shows a large lobular, heterogeneous mass centered in the left lateral ventricle. There are fluid-fluid levels from layering blood products.*

**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Axial T2 MR shows a mass expanding the chiasm and optic tracts with mass effect on the medial temporal lobes and midbrain. The T2 hyperintensity suggests a low-grade neoplasm.*

**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Sagittal T1 C+ MR shows intense enhancement with central hypointensity from infiltration of the optic chiasm and hypothalamus. In very young children, pilomyxoid astrocytomas often present very large in the optic pathway.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial T2 MR shows a heterogeneous mass with central cysts and a hypointense peripheral solid component with broad dural attachment . There is adjacent left frontal lobe edema and midline shift.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Coronal T1 C+ MR shows intense enhancement of the peripheral solid component of the left frontal heterogeneous mass. This peripheral, broad dural attachment of a solid, enhancing nodule is a specific sign of a desmoplastic infantile ganglioglioma or astrocytoma in the appropriate age range.*

**Choroid Plexus Papilloma**
*Axial CT shows an isodense, lobular, frond-like mass centered in the right atria of the lateral ventricle. There are layering blood products within enlarged lateral ventricles, indicating hydrocephalus.*

**Choroid Plexus Papilloma**
*Coronal T1 C+ MR shows an intensely enhancing lobular mass centered in the right choroid plexus glomus consistent with a choroid plexus tumor. There is associated hydrocephalus.*

**Supratentorial Ependymoma**
*Axial T1 C+ MR shows heterogeneous peripheral enhancement of mass surrounding central cystic necrosis. Supratentorial ependymomas arise most commonly in a periventricular location from ependymal rest cells.*

**Supratentorial Ependymoma**
*Axial T2 MR shows a heterogeneous mass with central necrosis in a periventricular location in this infant's frontal lobe. There is a peripheral hypointense T2 component indicating blood products . There is ventricular enlargement from hydrocephalus.*

**Medulloblastoma**
*Axial T2 MR shows a nodular and invasive mass within the superior 4th ventricle and cerebellar vermis . There is severe hydrocephalus and transependymal interstitial edema. Note susceptibility artifact from a ventriculostomy reservoir .*

**Medulloblastoma**
*Sagittal T1 C+ MR shows nodular, grape-like enhancement of the posterior fossa mass filling the superior 4th ventricle and invading the vermis . This appearance is suggestive of medulloblastoma with extensive nodularity, which has a favorable prognosis.*

**CNS Embryonal Tumor**
*Axial ADC map shows decreased diffusion surrounding the central necrosis. This was a WHO grade 4 CNS embryonal tumor, not otherwise specified. This was previously called PNET. The 2016 WHO CNS tumor classification has removed the term PNET.*

**CNS Embryonal Tumor**
*Axial T1 C+ MR shows a heterogeneous mass in the right cerebral hemisphere, which causes midline shift and ipsilateral ventricular effacement. There is central necrosis with surrounding ring enhancement .*

**Medulloblastoma**
*Axial DWI MR shows increased signal from decreased diffusion of the 4th ventricular tumor, consistent with a high-grade, hypercellular tumor, such as medulloblastoma. Decreased DWI can be seen in many high-grade neoplasms.*

**Medulloblastoma**
*Axial T2 MR shows a heterogeneous tumor within the 4th ventricle consistent with a classic medulloblastoma. Note the CSF cleft with the dorsal pons (floor) suggesting attachment to the roof of the 4th ventricle (vermis) .*

**Teratoma**
*Axial CT shows a midline lobular mass with solid and cystic components with focal coarse calcifications . There is extreme hydrocephalus, leaving only a small rind of brain parenchyma .*

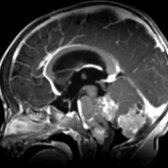
**Teratoma**
*Sagittal T1 MR shows a heterogeneous, lobular midline mass with an area of T1 hyperintensity consistent with areas of fat . There is extreme hydrocephalus with macrocrania. Although mature teratomas are low grade, they present very large with poor prognosis due to massive hydrocephalus.*

**Neurocutaneous Melanosis (Melanoma/Melanocytoma)**
*Coronal T1 C+ MR in a child with a large congenital nevi shows diffuse patchy and leptomeningeal enhancement from metastatic melanoma. The leptomeningeal form of neurocutaneous melanosis portends a poor prognosis.*
.](a7f4ea18-34f8-4e08-8ceb-695f627b70b1)
**Choroid Plexus Carcinoma**
*Axial T1 C+ MR in this 9-month-old infant shows a large, bulky, avidly enhancing left intraventricular tumor with invasion of the overlying brain . There are multiple intraventricular metastases .*

**Choroid Plexus Carcinoma**
*AP angiography performed as a part of preoperative embolization shows hypervascularity and multiple areas of contrast puddling .*

**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T2 MR in this 7-month-old infant shows hydrocephalus and a complicated solid and cystic tumor filling the 4th ventricle, supravermian cistern, and extending through the tentorial incisura .*

**Atypical Teratoid-Rhabdoid Tumor**
*Coronal T1 C+ MR in the same 7-month-old shows a right frontal metastatic deposit .*

**Neurocutaneous Melanosis (Melanoma/Melanocytoma)**
*Sagittal T1 MR shows increased signal intensity of the hippocampus in this 10-month-old with a large cutaneous nevus. Pachymeningeal thickening is present prior to contrast administration.*

**Embryonal Tumor With Multilayered Rosettes**
*Sagittal T1 MR in a 5-day-old infant shows a massive hemorrhagic tumor replacing and expanding the upper cervical spinal cord, the brainstem, and the cerebellum. The tumor protrudes through the incisura and displaces the straight sinus .*

**Embryonal Tumor With Multilayered Rosettes**
*Axial T2 MR shows a well-circumscribed, heterogeneous mass asymmetrically expanding the pons and the right middle cerebellar peduncle.*

**Embryonal Tumor With Multilayered Rosettes**
*Axial DWI of the well-circumscribed pontine tumor shows intense increased signal from decreased diffusion, suggesting this is a high-grade neoplasm. Medulloepithelioma is a highly primitive and aggressive tumor with a dismal prognosis.*

**Atypical Teratoid-Rhabdoid Tumor**
*Axial T1 C+ MR shows heterogeneous enhancement of the cerebellopontine angle tumor. Posterior fossa atypical teratoid-rhabdoid tumors can be difficult to distinguish from medulloblastomas, and both high-grade tumors have decreased diffusion.*

**Atypical Teratoid-Rhabdoid Tumor**
*Axial T2 MR shows a heterogeneous mass with cystic change and low T2 signal in the left cerebellopontine angle with invasion into the left internal auditory canal .*

**Choroid Plexus Carcinoma**
*Axial T1 C+ MR shows heterogeneous enhancement of the large intraventricular mass. While hemorrhage and parenchymal invasion are more likely with choroid plexus carcinoma, no particular imaging sign is able to specifically differentiate a papilloma from a carcinoma.*

**Choroid Plexus Carcinoma**
*Axial T2 MR shows a large lobular, heterogeneous mass centered in the left lateral ventricle. There are fluid-fluid levels from layering blood products.*

**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Axial T2 MR shows a mass expanding the chiasm and optic tracts with mass effect on the medial temporal lobes and midbrain. The T2 hyperintensity suggests a low-grade neoplasm.*

**Pilocytic Astrocytoma, Pilomyxoid Variant**
*Sagittal T1 C+ MR shows intense enhancement with central hypointensity from infiltration of the optic chiasm and hypothalamus. In very young children, pilomyxoid astrocytomas often present very large in the optic pathway.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Axial T2 MR shows a heterogeneous mass with central cysts and a hypointense peripheral solid component with broad dural attachment . There is adjacent left frontal lobe edema and midline shift.*

**Desmoplastic Infantile Ganglioglioma/Astrocytoma**
*Coronal T1 C+ MR shows intense enhancement of the peripheral solid component of the left frontal heterogeneous mass. This peripheral, broad dural attachment of a solid, enhancing nodule is a specific sign of a desmoplastic infantile ganglioglioma or astrocytoma in the appropriate age range.*

**Choroid Plexus Papilloma**
*Axial CT shows an isodense, lobular, frond-like mass centered in the right atria of the lateral ventricle. There are layering blood products within enlarged lateral ventricles, indicating hydrocephalus.*

**Choroid Plexus Papilloma**
*Coronal T1 C+ MR shows an intensely enhancing lobular mass centered in the right choroid plexus glomus consistent with a choroid plexus tumor. There is associated hydrocephalus.*

**Supratentorial Ependymoma**
*Axial T1 C+ MR shows heterogeneous peripheral enhancement of mass surrounding central cystic necrosis. Supratentorial ependymomas arise most commonly in a periventricular location from ependymal rest cells.*

**Supratentorial Ependymoma**
*Axial T2 MR shows a heterogeneous mass with central necrosis in a periventricular location in this infant's frontal lobe. There is a peripheral hypointense T2 component indicating blood products . There is ventricular enlargement from hydrocephalus.*

**Medulloblastoma**
*Axial T2 MR shows a nodular and invasive mass within the superior 4th ventricle and cerebellar vermis . There is severe hydrocephalus and transependymal interstitial edema. Note susceptibility artifact from a ventriculostomy reservoir .*

**Medulloblastoma**
*Sagittal T1 C+ MR shows nodular, grape-like enhancement of the posterior fossa mass filling the superior 4th ventricle and invading the vermis . This appearance is suggestive of medulloblastoma with extensive nodularity, which has a favorable prognosis.*

**CNS Embryonal Tumor**
*Axial ADC map shows decreased diffusion surrounding the central necrosis. This was a WHO grade 4 CNS embryonal tumor, not otherwise specified. This was previously called PNET. The 2016 WHO CNS tumor classification has removed the term PNET.*

**CNS Embryonal Tumor**
*Axial T1 C+ MR shows a heterogeneous mass in the right cerebral hemisphere, which causes midline shift and ipsilateral ventricular effacement. There is central necrosis with surrounding ring enhancement .*

**Medulloblastoma**
*Axial DWI MR shows increased signal from decreased diffusion of the 4th ventricular tumor, consistent with a high-grade, hypercellular tumor, such as medulloblastoma. Decreased DWI can be seen in many high-grade neoplasms.*

**Medulloblastoma**
*Axial T2 MR shows a heterogeneous tumor within the 4th ventricle consistent with a classic medulloblastoma. Note the CSF cleft with the dorsal pons (floor) suggesting attachment to the roof of the 4th ventricle (vermis) .*

**Teratoma**
*Axial CT shows a midline lobular mass with solid and cystic components with focal coarse calcifications . There is extreme hydrocephalus, leaving only a small rind of brain parenchyma .*

**Teratoma**
*Sagittal T1 MR shows a heterogeneous, lobular midline mass with an area of T1 hyperintensity consistent with areas of fat . There is extreme hydrocephalus with macrocrania. Although mature teratomas are low grade, they present very large with poor prognosis due to massive hydrocephalus.*

**Neurocutaneous Melanosis (Melanoma/Melanocytoma)**
*Coronal T1 C+ MR in a child with a large congenital nevi shows diffuse patchy and leptomeningeal enhancement from metastatic melanoma. The leptomeningeal form of neurocutaneous melanosis portends a poor prognosis.*