---
title: "Epidermoid Cyst"
docid: "704c5ddf-e1f7-4a5d-a1b8-5b0e603170d9"
authors:
- key: "5cff4116-3654-4b3a-bb75-5ebe0b8c9850"
value: "Anne G. Osborn, MD, FACR"
breadcrumbs:
-
name: "Brain"
slug: "brain"
treeNodeId: "6d8829f1-14d7-45af-8675-255189aa526a"
-
name: "Diagnosis"
slug: "diagnosis"
treeNodeId: "51c00394-446e-4a38-94af-d3b1d14d34e8"
-
name: "Pathology-Based Diagnoses"
slug: "pathology-based-diagnoses"
treeNodeId: "d9d3a8ed-f21b-4831-8c77-591a3500ef77"
-
name: "Primary Nonneoplastic Cysts"
slug: "primary-nonneoplastic-cysts"
treeNodeId: "8037bffe-f61e-4433-b841-a263bcfbe056"
-
name: "Epidermoid Cyst"
slug: "epidermoid-cyst"
treeNodeId: null
category: "Brain"
documentVersionId: "4092685b-a22f-42ca-b14b-6a21122b651f"
imageCount: 22
lastUpdated: "06/12/20"
pageDescription: "Epidermoid Cyst"
pageKeywords: "Brain, Diagnosis, Pathology-Based Diagnoses, Primary Nonneoplastic Cysts, Epidermoid Cyst"
pageTitle: "Epidermoid Cyst | STATdx"
enhancedTitle: "Epidermoid Cyst"
type: "DX"
references: true
breadcrumbs:
- "Brain"
- "Diagnosis"
- "Pathology-Based Diagnoses"
- "Primary Nonneoplastic Cysts"
- "Epidermoid Cyst"
---
# KEY FACTS
- ## Terminology
- Intracranial epidermoids ("pearly" tumor)
- Congenital ectodermal inclusion cysts, not true neoplasm
- ## Imaging
- CSF-like mass that insinuates cisterns and encases neurovascular structures
- Morphology: Lobulated, irregular, cauliflower-like mass with "fronds"
- FLAIR: Usually does not completely null
- DWI: Diffusion restriction definitively distinguishes from arachnoid cyst
- ## Top Differential Diagnoses
- Arachnoid cyst
- Inflammatory cyst (i.e., neurocysticercosis)
- Cystic neoplasm
- Dermoid cyst
- ## Pathology
- Arise from ectodermal inclusions during neural tube closure, 3rd to 5th week of embryogenesis
- ## Clinical Issues
- Symptoms depend on location and effect on adjacent neurovascular structures
- Most common symptom: Headache
- Cranial nerves V, VII, VIII neuropathy common
- 0.2-1.8% of all primary intracranial tumors
- Rare malignant degeneration into squamous cell carcinoma
- Treatment: Microsurgical resection
- Recurrence common if incompletely removed
- ## Diagnostic Checklist
- Insinuates CSF spaces, surrounds arteries, CNs with minimal displacement
- Incomplete nulling on FLAIR; DWI hyperintense
# TERMINOLOGY
- ## Synonyms
- Ectodermal inclusion cyst
- "Pearly" tumor
- ## Definitions
- Intracranial epidermoids are congenital inclusion cysts (not "tumors")
- Benign, slow-growing congenital lesions derived from ectodermal remnants sequestrated during embryogenesis
# IMAGING
- ## General Features
- ### Best diagnostic clue
- CSF-like mass that insinuates cisterns and encases neurovascular structures
- ### Location
- Intradural (90%), strong predilection for basal cisterns
- Cerebellopontine angle (CPA) (40-50%)
- 4th ventricle (17%)
- Parasellar/middle cranial fossa/sylvian fissure (10-15%)
- Parenchymal (i.e., cerebral hemispheres) rare (1.5%)
- Brainstem exceedingly rare
- Extradural (10%)
- Skull (intradiploic within frontal, parietal, occipital, sphenoid skull) as well as spine
- ### Size
- Variable; extradural intradiploic variants can become huge with minimal/no neurologic deficits
- Grow slowly by desquamation of normal cells into cystic cavity
- ### Morphology
- Lobulated, irregular, cauliflower-like excrescences
- Insinuates without mass effect unless large
- ## Radiographic Findings
- ### Radiography
- Diploic space epidermoids
- May alter scalp, outer/inner skull tables, and epidural space appearance
- Typically round or lobulated
- Well delineated with sclerotic rim
- ## CT Findings
- ### NECT
- Round/lobulated mass
- > 95% hypodense, resembling CSF
- 10-25% contain calcifications
- Rare variant = "dense" epidermoid
- 3% of intracranial epidermoids
- Secondary to hemorrhage, high protein, saponification of cyst debris to calcium soaps or iron-containing pigment
- ### CECT
- Usually none, though margin of cyst may show minimal enhancement
- ### Bone CT
- May have bony erosion; sharply corticated margins when intradiploic
- ## MR Findings
- ### T1WI
- Often (~ 75%) slightly hyperintense to CSF
- Lobulated periphery may be slightly more hyperintense than center
- Uncommonly hyperintense to brain ("white epidermoid") due to high triglycerides and unsaturated fatty acids
- Uncommonly hypointense to CSF ("black epidermoid")
- Presence of solid crystal cholesterol and keratin
- Lack of triglycerides and unsaturated fatty acids
- ### T2WI
- Often isointense (65%) to slightly hyperintense (35%) to CSF
- Very rarely hypointense due to calcification, ↓ hydration, viscous secretions, and iron pigments
- ### FLAIR
- Usually does not completely null
- ### DWI
- Characteristic hyperintensity
- High fractional anisotropy due to diffusion along 2D geometric plane
- Attributed to microstructure of parallel-layered keratin filaments and flakes
- In comparison to white matter, which also shows high fractional anisotropy, due to diffusion along single direction
- ADC = brain parenchyma
- ### T1WI C+
- Usually none, though margin of cyst may show minimal enhancement (25%)
- Enhancing tumor is sign of malignant degeneration
- ### MRS
- Resonances from lactate
- No NAA, choline, or lipid
- ## Angiographic Findings
- Conventional
- Depending on location and size, may show avascular mass effect
- ## Nonvascular Interventions
- ### Myelography
- Cisternography contrast delineates irregular lobulated tumor borders, extends into interstices
- ## Imaging Recommendations
- ### Best imaging tool
- MR
- ### Protocol advice
- FLAIR will often distinguish, whereas conventional sequences may not
- Diffusion restriction definitively distinguishes from arachnoid cyst
# DIFFERENTIAL DIAGNOSIS
- [Arachnoid Cyst](/document/arachnoid-cyst/d25aaeb3-5b3c-4483-99dc-2757468eedb9)
- Usually isointense to CSF on all standard sequences
- Completely nulls on FLAIR
- Hypointense diffusion: Contains highly mobile CSF, ADC = stationary water
- Rather than insinuate and engulf local structures, arachnoid cysts displace them
- Smooth surface, unlike lobulations of epidermoids
- [Inflammatory Cyst](/document/neurocysticercosis/6a45835f-6d7c-443e-874a-f33131d3def1)
- i.e., neurocysticercosis
- Often enhances
- Density/signal intensity usually not precisely like CSF
- Adjacent edema, gliosis common
- [Cystic Neoplasm](/document/pilocytic-astrocytoma/7eca92f5-6caa-4300-9afe-1b733b4473b2)
- Attenuation/signal intensity not that of CSF
- Often enhances
- [Dermoid Cyst](/document/dermoid-cyst/9b7aeb04-2cb3-405d-8c51-dd13297dd67c)
- Usually at or near midline
- Resembles fat, not CSF, and contains dermal appendages; often ruptured
# PATHOLOGY
- ## General Features
- ### Etiology
- Congenital: Embryology
- Arise from ectodermal inclusions during neural tube closure, 3rd to 5th week of embryogenesis
- Congenital intradural CPA epidermoids derived from cells of 1st branchial groove
- Acquired: Develop as result of trauma
- Uncommon etiology for intracranial tumors
- More common as spine etiology following LP
- ### Genetics
- Sporadic
- ### Associated abnormalities
- May have occipital/nasofrontal dermal sinus tract
- ## Gross Pathologic & Surgical Features
- Outer surface often has shiny, glistening, mother-of-pearl appearance ("beautiful tumor")
- Soft and pliable
- Conforms to shape of adjacent local structures/spaces
- Lobulated excrescences
- May invaginate into brain
- Insinuating growth pattern, extends through cisterns, surrounds and encases vessels/nerves
- Cyst filled with soft, waxy, creamy, or flaky keratinaceous material
- ## Microscopic Features
- Cyst wall = internal layer of simple stratified cuboidal squamous epithelium covered by fibrous capsule
- Cyst contents = solid crystalline cholesterol, keratinaceous debris; no dermal appendages
- Grows by progressive desquamation with conversion to keratin/cholesterol crystals, forming concentric lamellae
# CLINICAL ISSUES
- ## Presentation
- ### Most common signs/symptoms
- Symptoms depend on location and effect on adjacent neurovascular structures
- Most common symptom: Headache
- Cranial nerves V, VII, VIII neuropathy common
- 4th ventricular cerebellar signs common, yet increased intracranial pressure rare
- Less commonly hypopituitarism, diabetes insipidus
- Seizures if in sylvian fissure/temporal lobe
- May remain clinically silent for many years
- ## Demographics
- ### Age
- Presents between 20-60 years with peak at 40 years
- Presentation is uncommon in childhood
- ### Sex
- M = F
- CT hyperdense variant lesions have female predominance (M:F = 1:2.5)
- ### Epidemiology
- Epidermoids make up 0.2-1.8% of all primary intracranial tumors
- Much more common than dermoid cyst (4-9x higher incidence)
- Most common congenital intracranial tumor
- 3rd most common CPA/IAC mass, after vestibular schwannoma and meningioma
- ## Natural History & Prognosis
- Grows slowly: Epithelial component growth rate commensurate to that of normal epithelium
- Chemical meningitis possible from content leakage
- Rare malignant degeneration into squamous cell carcinoma (SCCa) reported
- Postulated prolonged or reparative process from foreign material leads to cellular atypia and neoplasia
- Often predated by frequent recurrences
- May occur years after surgical resection
- Mean age at presentation: 52 years with male preponderance
- ## Treatment
- Microsurgical resection
- Complicated by investment of local structures
- Recurrence common if cyst capsule incompletely removed
- Subarachnoid dissemination of contents may occur during operative/postoperative course
- May cause chemical meningitis
- CSF seeding and implantation reported
- Rare malignant degeneration of resection bed into SCCa reported
# DIAGNOSTIC CHECKLIST
- ## Consider
- Epidermoid if insinuates CSF spaces, surrounds arteries/CNs with minimal displacement
- ## Image Interpretation Pearls
- Resembles CSF on imaging studies, except usually incomplete nulling on FLAIR
- DWI hyperintensity is diagnostic
da5731a9-6c09-4bf5-99d9-fdefe09d5800
## References
# Selected References
1. [Pons Escoda A et al: Imaging of skull vault tumors in adults. Insights Imaging. 11(1):23, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=32056014%5Bpmid%5D)
1. [Bobeff EJ et al: Suprasellar Epidermoid Cyst: Case Report of Extended Endoscopic Transsphenoidal Resection and Systematic Review of the Literature. World Neurosurg. 128:514-26, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=31121364%5Bpmid%5D)
1. [Hitti FL et al: Endoscopic Resection of a Cerebellopontine Angle Epidermoid Cyst via a Retrosigmoid Approach. J Neurol Surg B Skull Base. 80(Suppl 3):S330, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=31143618%5Bpmid%5D)
1. [Ma J et al: Primary intradiploic epidermoid cyst: a case report with literature review. Clin Neuropathol. 38(1):28-32, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30526818%5Bpmid%5D)
1. [Badat N et al: Malignant transformation of epidermoid cyst with diffuse leptomeningeal carcinomatosis on skull base and trigeminal perineural spread. J Neuroradiol. 45(5):337-40, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=30036548%5Bpmid%5D)
1. [Gollapudi PR et al: A frontal giant intradiploic giant pearl (epidermoid cyst) with intracranial and extracranial extension: a rare entity. J Pediatr Neurosci. 13(4):480-2, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=30937095%5Bpmid%5D)
1. [Twede JV et al: Intraosseous epidermoid cyst of the skull: case study and radiological imaging considerations. Dermatol Online J. 24(7), 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=30261578%5Bpmid%5D)
1. [Vaz-Guimaraes F et al: Endoscopic endonasal surgery for epidermoid and dermoid cysts: a 10-year experience. J Neurosurg. 1-11, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=29547084%5Bpmid%5D)
1. [Aboud E et al: Giant intracranial epidermoids: is total removal feasible? J Neurosurg. 1-14, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=25594324%5Bpmid%5D)
1. [Law EK et al: Atypical intracranial epidermoid cysts: rare anomalies with unique radiological features. Case Rep Radiol. 2015:528632, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=25667778%5Bpmid%5D)
1. [Demir MK et al: Rare and challenging extra-axial brain lesions: CT and MRI findings with clinico-radiological differential diagnosis and pathological correlation. Diagn Interv Radiol. 20(5):448-52, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=25010368%5Bpmid%5D)
1. [Vellutini EA et al: Malignant transformation of intracranial epidermoid cyst. Br J Neurosurg. 28(4):507-9, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24345076%5Bpmid%5D)
1. [Velamati R et al: Meningitis secondary to ruptured epidermoid cyst: case-based review. Pediatr Ann. 42(6):248-51, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=23718247%5Bpmid%5D)
1. [Ren X et al: Clinical, radiological, and pathological features of 24 atypical intracranial epidermoid cysts. J Neurosurg. 116(3):611-21, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22175719%5Bpmid%5D)
1. [Li F et al: Hyperdense intracranial epidermoid cysts: a study of 15 cases. Acta Neurochir (Wien). 149(1):31-9; discussion 39, 2007](http://www.ncbi.nlm.nih.gov/pubmed/?term=17151831%5Bpmid%5D)
## Images
### Selected Images
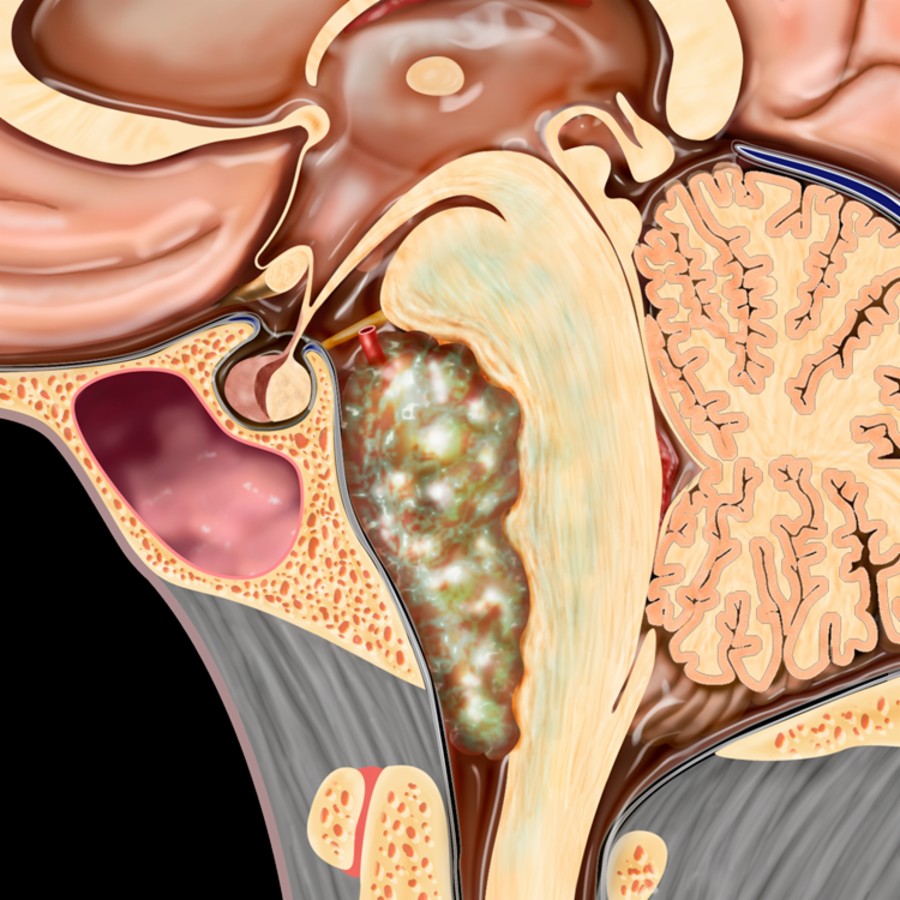
*Sagittal graphic shows a multilobulated epidermoid primarily within the prepontine cistern. Significant mass effect displaces the pons, cervicomedullary junction, and upper cervical spine.*
 . Note its typical pearly appearance. (Courtesy E. Hedley-Whyte, MD.)](images/app.statdx.com_image_thumbnail_69c8e599-c4d6-4096-8762-d50c4ff210a7_annotated_true_size_900_quality_90_ab2a4510.jpg)
*Gross pathology shows an epidermoid cyst extending anterosuperiorly from the cerebellopontine angle (CPA) cistern, insinuating within the prepontine cistern and encasing the basilar artery . Note its typical pearly appearance. (Courtesy E. Hedley-Whyte, MD.)*

*Gross pathology shows an epidermoid cyst extending anterosuperiorly from the cerebellopontine angle (CPA) cistern, insinuating within the prepontine cistern and encasing the basilar artery . Note its typical pearly appearance. (Courtesy E. Hedley-Whyte, MD.)*
 is slightly more dense than the adjacent CSF
is slightly more dense than the adjacent CSF  and has a frothy, cauliflower-like surface.](images/app.statdx.com_image_thumbnail_0e8c9ff7-efdd-4f6b-953d-f9c6005d0d3b_annotated_true_size_900_quality_90_53ed4f8a.jpg)
*Axial NECT shows a typical epidermoid cyst (EC) in an expanded right CPA cistern. Note that the EC is slightly more dense than the adjacent CSF and has a frothy, cauliflower-like surface.*

*Axial NECT shows a typical epidermoid cyst (EC) in an expanded right CPA cistern. Note that the EC is slightly more dense than the adjacent CSF and has a frothy, cauliflower-like surface.*
 .](images/app.statdx.com_image_thumbnail_9fe7a5f9-a971-4bfa-a40d-71b4c44a98a1_annotated_true_size_900_quality_90_d3fb2e8a.jpg)
*MR shows CPA epidermoid cyst that resembles CSF on T1 and T2 but typically does not suppress on FLAIR and demonstrates moderate restricted diffusion .*

*Sagittal T1 MR in a 39-year-old woman with a history of attempted resection of a posterior fossa EC shows a large mass infiltrating the prepontine cistern and wrapping around the cervicomedullary junction . The mass is nearly isointense with CSF.*

*MR shows CPA epidermoid cyst that resembles CSF on T1 and T2 but typically does not suppress on FLAIR and demonstrates moderate restricted diffusion .*

*Sagittal T1 MR in a 39-year-old woman with a history of attempted resection of a posterior fossa EC shows a large mass infiltrating the prepontine cistern and wrapping around the cervicomedullary junction . The mass is nearly isointense with CSF.*
 in the right CPA cistern that is nearly isointense with CSF in the cistern and 4th ventricle .](images/app.statdx.com_image_thumbnail_8cda8365-0903-4b43-b366-135ee0875419_annotated_true_size_900_quality_90_a50364f4.jpg)
*Axial PD MR in the same patient shows a lobulated mass in the right CPA cistern that is nearly isointense with CSF in the cistern and 4th ventricle .*

*Axial T2 MR in the same patient shows the mass is nearly as hyperintense as fluid in the CPA cistern and 4th ventricle .*

*Coronal T2 MR shows the lobulated, hyperintense mass encases and displaces the basilar artery . CSF in the right middle fossa is a cavity from prior attempted resection.*

*Axial FLAIR MR demonstrates that the lobulated, cauliflower-like mass in the right CPA and prepontine cistern does not suppress.*

*The mass restricts on DWI MR. This is a classic EC that infiltrates and insinuates CSF cisterns, encasing vessels (like the basilar artery) and cranial nerves (in this case, cranial nerves VII and VIII).*
### Additional Images

*Gross pathology nicely shows the typical shiny, glistening, pearly appearance of an epidermoid residing within the prepontine cistern, which was also encasing the basilar artery (not shown).*

*Axial T2 MR shows a nearly CSF isointense epidermoid within the left anterior middle cranial fossa.*

*Axial DWI MR shows restricted diffusion within a left anterior middle cranial fossa epidermoid.*

*Axial T2 MR shows an extraaxial left occipital mass that scallops the skull and displaces the dura inwardly .*

*Axial T1 C+ FS MR in the same patient shows the mass does not enhance . DWI (not shown) clinched the diagnosis as an EC. This is an atypical location for epidermoid.*

*Axial bone CT in the same patient reveals significant yet benign-appearing remodeling and scalloping of the inner calvarial table .*

*Bone CT in a 16-year-old girl with nonspecific headaches shows a smoothly marginated, lytic, expansile mass centered on the diploic space of the calvarium.*

*Axial NECT in the same patient shows the calvarial cyst is hypodense relative to cortex. This is a classic EC of the skull and was an incidental finding in this asymptomatic patient.*

*Axial bone CT demonstrates the typical appearance of a large intradiploic epidermoid as an expansile lesion with sharply corticated margins .*

*Axial T2 MR in the same patient shows the lobulated, hyperintense mass scallops the skull . Intradiploic EC was removed at surgery.*

*Axial T1 (upper left), T2 (upper right) and FLAIR (lower left) MR show an extensive intradiploid EC. Coronal T1 C+ MR (lower right) shows mild enhancement around the cyst margin.*

*Axial T2 (upper left), FLAIR (upper right), T1 C+ (lower left), and DWI (lower right) MR show a recurrent EC that appears intraaxial, but the original surgery 24 years prior disclosed an EC of the quadrigeminal cistern.*
in the right CPA cistern that is nearly isointense with CSF in the cistern and 4th ventricle .](images/app.statdx.com_image_thumbnail_8cda8365-0903-4b43-b366-135ee0875419_annotated_true_size_900_quality_90_a50364f4.jpg)
*Axial PD MR in the same patient shows a lobulated mass in the right CPA cistern that is nearly isointense with CSF in the cistern and 4th ventricle .*

*Axial T2 MR in the same patient shows the mass is nearly as hyperintense as fluid in the CPA cistern and 4th ventricle .*

*Coronal T2 MR shows the lobulated, hyperintense mass encases and displaces the basilar artery . CSF in the right middle fossa is a cavity from prior attempted resection.*

*Axial FLAIR MR demonstrates that the lobulated, cauliflower-like mass in the right CPA and prepontine cistern does not suppress.*

*The mass restricts on DWI MR. This is a classic EC that infiltrates and insinuates CSF cisterns, encasing vessels (like the basilar artery) and cranial nerves (in this case, cranial nerves VII and VIII).*
### Additional Images

*Gross pathology nicely shows the typical shiny, glistening, pearly appearance of an epidermoid residing within the prepontine cistern, which was also encasing the basilar artery (not shown).*

*Axial T2 MR shows a nearly CSF isointense epidermoid within the left anterior middle cranial fossa.*

*Axial DWI MR shows restricted diffusion within a left anterior middle cranial fossa epidermoid.*

*Axial T2 MR shows an extraaxial left occipital mass that scallops the skull and displaces the dura inwardly .*

*Axial T1 C+ FS MR in the same patient shows the mass does not enhance . DWI (not shown) clinched the diagnosis as an EC. This is an atypical location for epidermoid.*

*Axial bone CT in the same patient reveals significant yet benign-appearing remodeling and scalloping of the inner calvarial table .*

*Bone CT in a 16-year-old girl with nonspecific headaches shows a smoothly marginated, lytic, expansile mass centered on the diploic space of the calvarium.*

*Axial NECT in the same patient shows the calvarial cyst is hypodense relative to cortex. This is a classic EC of the skull and was an incidental finding in this asymptomatic patient.*

*Axial bone CT demonstrates the typical appearance of a large intradiploic epidermoid as an expansile lesion with sharply corticated margins .*

*Axial T2 MR in the same patient shows the lobulated, hyperintense mass scallops the skull . Intradiploic EC was removed at surgery.*

*Axial T1 (upper left), T2 (upper right) and FLAIR (lower left) MR show an extensive intradiploid EC. Coronal T1 C+ MR (lower right) shows mild enhancement around the cyst margin.*

*Axial T2 (upper left), FLAIR (upper right), T1 C+ (lower left), and DWI (lower right) MR show a recurrent EC that appears intraaxial, but the original surgery 24 years prior disclosed an EC of the quadrigeminal cistern.*