---
title: "Fragile X-Associated Tremor/Ataxia (FXTAS)"
docid: "4778fafe-9873-4c28-8f4f-299c00c72b50"
authors:
- key: "a25c450b-3d34-4f64-bba3-cc0834813df6"
value: "Miral D. Jhaveri, MD, MBA"
breadcrumbs:
-
name: "Brain"
slug: "brain"
treeNodeId: "6d8829f1-14d7-45af-8675-255189aa526a"
-
name: "Diagnosis"
slug: "diagnosis"
treeNodeId: "51c00394-446e-4a38-94af-d3b1d14d34e8"
-
name: "Pathology-Based Diagnoses"
slug: "pathology-based-diagnoses"
treeNodeId: "d9d3a8ed-f21b-4831-8c77-591a3500ef77"
-
name: "Acquired Toxic/Metabolic/Degenerative Disorders"
slug: "acquired-toxicmetabolicdegenerativ-"
treeNodeId: "ba3cfeaf-64d9-4117-91e8-d2ce58783fc5"
-
name: "Dementias and Degenerative Disorders"
slug: "dementias-and-degenerative-disorde-"
treeNodeId: "6381104d-7a4c-4be5-bb19-3cd90837d547"
-
name: "Fragile X-Associated Tremor/Ataxia (FXTAS)"
slug: "fragile-x-associated-tremorataxia--"
treeNodeId: null
category: "Brain"
documentVersionId: "19e8e928-1533-4e9f-8293-80f21fba4e0a"
imageCount: 4
lastUpdated: "08/05/20"
pageDescription: "Fragile X-Associated Tremor/Ataxia (FXTAS)"
pageKeywords: "Brain, Diagnosis, Pathology-Based Diagnoses, Acquired Toxic/Metabolic/Degenerative Disorders, Dementias and Degenerative Disorders, Fragile X-Associated Tremor/Ataxia (FXTAS)"
pageTitle: "Fragile X-Associated Tremor/Ataxia (FXTAS) | STATdx"
enhancedTitle: "Fragile X-Associated Tremor/Ataxia (FXTAS)"
type: "DX"
references: true
breadcrumbs:
- "Brain"
- "Diagnosis"
- "Pathology-Based Diagnoses"
- "Acquired Toxic/Metabolic/Degenerative Disorders"
- "Dementias and Degenerative Disorders"
- "Fragile X-Associated Tremor/Ataxia (FXTAS)"
---
# KEY FACTS
- ## Terminology
- Fragile X-associated tremor/ataxia syndrome (FXTAS)
- X-linked progressive neurodegenerative disorder characterized by 55-200 CGG trinucleotide repeats in *FMR1* gene
- ## Imaging
- Ventricular and sulcal prominence: Global volume loss
- WM and brainstem hyperintensities
- MCP atrophy with symmetric hyperintensities: MCP sign
- Decreased MCP width may be first notable sign
- Splenium of corpus callosum atrophy with hyperintensity: Corpus callosum splenium sign
- High sensitivity but lower specificity than MCP sign
- ## Top Differential Diagnoses
- **Middle cerebellar peduncle sign**
- Neurodegenerative, metabolic, cerebrovascular, inflammatory and demyelinating disorders
- **Corpus callosum splenium sign**
- Normal aging, radiation therapy
- Cytotoxic/transient splenial lesions
- ## Pathology
- Premutation expansions (55-200 CGG repeats) in 5' untranslated region of *FMR1* gene, located on X-chromosome
- **Radiological criteria**
- Major: White matter lesions in brainstem or MCP sign
- Minor: Cerebral white matter lesions, moderate to severe generalized brain atrophy
- ## Clinical Issues
- Kinetic tremor, cerebellar gait ataxia, cognitive dysfunction
- Usually > age 50
- Diagnosis confirmed by molecular genetic testing
- Progressive and severe neurodegenerative disease
# TERMINOLOGY
- ## Abbreviations
- Fragile X-associated tremor/ataxia syndrome (FXTAS)
- ## Definitions
- X-linked progressive neurodegenerative disorder characterized by 55-200 CGG trinucleotide repeats in *FMR1* gene
# IMAGING
- ## General Features
- ### Best diagnostic clue
- Generalized brain atrophy with hyperintensities in brainstem or middle cerebellar peduncle (MCP)
- ### Location
- Brainstem and middle cerebellar peduncles
- Cerebral white matter (WM), corpus callosum
- ### Size
- MCP atrophy, global atrophy
- ## CT Findings
- ### NECT
- Moderate to severe generalized brain atrophy
- MCP atrophy with subtle hypodensities
- ## MR Findings
- ### T1WI
- Subtle hypointensity in MCP with atrophy
- Corpus callosum splenium hypointensity
- ### FLAIR
- Ventricular and sulcal prominence: Global volume loss
- WM and brainstem hyperintensities
- Putaminal rim hyperintensity
- MCP atrophy with symmetric hyperintensities: MCP sign
- Decreased MCP width may be first notable sign
- Splenium of corpus callosum atrophy with hyperintensity: Corpus callosum splenium sign
- High sensitivity but lower specificity than MCP sign
- ### T2* GRE
- No hemorrhage
- ### T1WI C+
- No enhancement
- ### MRS
- Decreased NAA/Cr and Ch/Cr in MCP
- DTI
- Reduced fractional anisotropy (FA) in corpus callosum
- Associated with increasing FXTAS symptom severity
- Reduced FA in MCP
- ## Imaging Recommendations
- ### Best imaging tool
- Brain MR without contrast
- ### Protocol advice
- Add coronal T2/FLAIR MR
# DIFFERENTIAL DIAGNOSIS
- ## Middle Cerebellar Peduncle Sign
- **Neurodegenerative**
- Multiple systemic atrophy (MSA), olivopontocerebellar atrophy, spinocerebellar ataxia
- **Metabolic**
- Adrenoleukodystrophy, Wilson disease, hypoglycemia
- **Cerebrovascular**
- Infarcts, PRES, pontine infarct with wallerian degeneration of MCPs
- **Inflammatory and demyelinating**
- Multiple sclerosis, ADEM, Behçet disease
- ## Corpus Callosum Splenium Sign
- Normal aging, radiation therapy
- Cytotoxic /transient splenial lesions
- Seizure- &/or drug-related, viral encephalitis, metabolic derangement
# PATHOLOGY
- ## General Features
- ### Genetics
- Premutation expansions (55-200 CGG repeats) in untranslated region of *FMR1* gene, located on X-chromosome
- Full mutation (> 200 CGG repeats) leads to neurodevelopmental disease fragile X syndrome (FXS)
- 2 main molecular mechanisms
- Toxic gain of function of expanded CGG-repeat *FMR1*mRNA → binding/sequestration of CGG-binding proteins
- CGG repeat-associated non-AUG-initiated (RAN) translation → polyglycine peptide toxic to cells
- ## Staging, Grading, & Classification
- Diagnostic criteria for FXTAS: Clinical, radiological, and pathological
- **Radiological criteria**
- Major criteria: WM lesions in brainstem or MCP sign
- Minor criteria: Cerebral WM lesions, moderate to severe generalized brain atrophy
- ## Microscopic Features
- Diffuse, spongy degeneration of WM
- Eosinophilic intranuclear inclusions in neurons and astrocytes with cortex and cerebellum
# CLINICAL ISSUES
- ## Presentation
- ### Most common signs/symptoms
- Kinetic tremor, cerebellar gait ataxia, cognitive dysfunction
- ### Other signs/symptoms
- Psychiatric disorders common
- ## Demographics
- Usually > age 50
- More common among male patients who are hemizygous for premutation (40%) than female patients who are heterozygous for premutation (8-16%)
- ## Natural History & Prognosis
- Diagnosis confirmed by molecular genetic testing
- Progressive and severe neurodegenerative disease
- ## Treatment
- Symptomatic and supportive
# DIAGNOSTIC CHECKLIST
- ## Consider
- Patient presenting with ataxia and tremor with symmetric middle cerebellar peduncle hyperintensities (MCP sign)
863ab378-3ef7-4994-a374-6fc4bb8249e5
## References
# Selected References
1. [Cvejic RC et al: Reduced caudate volume and cognitive slowing in men at risk of fragile X-associated tremor ataxia syndrome. Brain Imaging Behav. ePub, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=30046972%5Bpmid%5D)
1. [Famula JL et al: Presence of middle cerebellar peduncle sign in FMR1 premutation carriers without tremor and ataxia. Front Neurol. 9:695, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=30186228%5Bpmid%5D)
1. [Mascalchi M et al: Neuroimaging Applications in Chronic Ataxias. Int Rev Neurobiol. 143:109-162, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=30473193%5Bpmid%5D)
1. [Hall DA et al: The corpus callosum splenium sign in fragile X-associated tremor ataxia syndrome. Mov Disord Clin Pract. 4(3):383-8, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=30363360%5Bpmid%5D)
1. [Fasano A et al: MRI-guided focused ultrasound thalamotomy in fragile X-associated tremor/ataxia syndrome. Neurology. 87(7):736-8, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27440151%5Bpmid%5D)
1. [Filley CM: Fragile X tremor ataxia syndrome and white matter dementia. Clin Neuropsychol. 30(6):901-12, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27356088%5Bpmid%5D)
## Images
### Selected Images
 , brainstem
, brainstem  , and cerebellum
, and cerebellum  .](images/app.statdx.com_image_thumbnail_bd354cab-3b2c-4a44-834d-8a782f46ee4d_size_168_quality_85_ce881543_20251014T204705Z.jpg)
*Sagittal T1 MR in a 56-year-old man with fragile X-associated tremor/ataxia syndrome (FXTAS) demonstrates atrophy of the corpus callosum , brainstem , and cerebellum .*
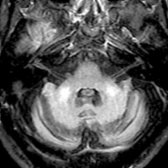
*Axial FLAIR MR in the same patient shows decreased width of the middle cerebellar peduncles with symmetric hyperintensities , consistent with the MCP sign. This sign can be seen in a number of conditions, particularly neurodegenerative diseases, and is most commonly associated with FXTAS.*
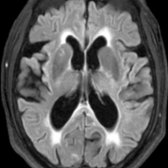
*Axial FLAIR MR in a patient with tremor, cerebellar ataxia, and cognitive decline shows diffuse parenchymal volume loss, WM hyperintensities , and hyperintensity in the splenium of the corpus callosum (corpus callosum splenium sign).*
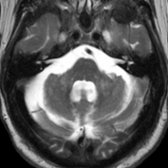
*Axial T2 MR in the same patient shows atrophy of the middle cerebellar peduncles with symmetric hyperintensities (MCP sign). The patient was diagnosed with definite FXTAS and had 166 CGG repeats on molecular genetic testing.*
.](images/app.statdx.com_image_thumbnail_bd354cab-3b2c-4a44-834d-8a782f46ee4d_size_168_quality_85_ce881543_20251014T204705Z.jpg)
*Sagittal T1 MR in a 56-year-old man with fragile X-associated tremor/ataxia syndrome (FXTAS) demonstrates atrophy of the corpus callosum , brainstem , and cerebellum .*

*Axial FLAIR MR in the same patient shows decreased width of the middle cerebellar peduncles with symmetric hyperintensities , consistent with the MCP sign. This sign can be seen in a number of conditions, particularly neurodegenerative diseases, and is most commonly associated with FXTAS.*

*Axial FLAIR MR in a patient with tremor, cerebellar ataxia, and cognitive decline shows diffuse parenchymal volume loss, WM hyperintensities , and hyperintensity in the splenium of the corpus callosum (corpus callosum splenium sign).*

*Axial T2 MR in the same patient shows atrophy of the middle cerebellar peduncles with symmetric hyperintensities (MCP sign). The patient was diagnosed with definite FXTAS and had 166 CGG repeats on molecular genetic testing.*