---
title: "Interrupted/Hypoplastic Aorta"
docid: "100ba59a-24e8-47b4-b2b2-bbfdc0a21e92"
authors:
- key: "770e1d77-2287-436e-910b-48232afc7842"
value: "Prabhakar Rajiah, MBBS, MD, FACR, FRCR, FACC, FAHA, FSCCT"
- key: "e915766e-8102-46e4-a33e-c83f8ae12f29"
value: "Harold Goerne, MD"
breadcrumbs:
-
name: "Cardiac"
slug: "cardiac"
treeNodeId: "fa90100b-619c-430e-8074-b5b9789bab39"
-
name: "Diagnosis"
slug: "diagnosis"
treeNodeId: "5c92cf4f-e9d5-4059-9c13-22255c51c121"
-
name: "Aorta"
slug: "aorta"
treeNodeId: "4d206a6b-1a82-467c-9199-0df25ab749d7"
-
name: "Interrupted/Hypoplastic Aorta"
slug: "interruptedhypoplastic-aorta"
treeNodeId: null
category: "Cardiac"
documentVersionId: "00b8d951-9dbc-40d4-9499-c8705f77762e"
imageCount: 15
lastUpdated: "01/28/25"
pageDescription: "Interrupted/Hypoplastic Aorta"
pageKeywords: "Cardiac, Diagnosis, Aorta, Interrupted/Hypoplastic Aorta"
pageTitle: "Interrupted/Hypoplastic Aorta | STATdx"
enhancedTitle: "Interrupted/Hypoplastic Aorta"
type: "DX"
references: true
breadcrumbs:
- "Cardiac"
- "Diagnosis"
- "Aorta"
- "Interrupted/Hypoplastic Aorta"
---
# KEY FACTS
- ## Terminology
- Interrupted aortic arch
- Complete luminal and anatomic wall discontinuity between ascending aorta and descending aorta
- Hypoplastic aortic arch
- Tubular narrowing without luminal discontinuity
- ## Imaging
- CTA
- Best noninvasive modality to assess aortic arch and supraaortic vessels pattern
- US
- 1st-line modality to assess aortic arch abnormalities
- Best diagnostic clue
- Interrupted aortic arch
- Blind ends in distal ascending aorta and proximal descending aorta with luminal discontinuity in between
- Hypoplastic aortic arch
- Tubular narrowing of aortic arch; proximal aortic arch < 60% &/or distal aortic arch < 50% of diameter of ascending aorta
- ## Top Differential Diagnoses
- Coarctation of aorta
- ## Pathology
- Type A (13%)
- Interruption distal to left subclavian artery
- Type B (84%)
- Interruption between left common carotid artery and left subclavian artery
- Type C (3%)
- Interruption between brachiocephalic trunk and left common carotid artery
- ## Clinical Issues
- Rare condition
- 1% of congenital heart disease
# TERMINOLOGY
- ## Abbreviations
- Interrupted aortic arch (IAA)
- Hypoplastic aortic arch (HAA)
- ## Synonyms
- Atresia of aortic arch
- ## Definitions
- IAA
- Complete luminal discontinuity between ascending aorta and descending aorta
- Not true interruption, as there is fibrotic continuity between blind ends
- HAA
- Tubular narrowing of aortic arch without luminal discontinuity
# IMAGING
- ## General Features
- ### Best diagnostic clue
- IAA
- Blind-ending distal ascending aorta and proximal descending aorta with luminal discontinuity in between
- HAA
- Tubular narrowing of aortic arch
- Proximal arch < 60% &/or distal aortic arch < 50% of diameter of ascending aorta
- Transverse aortic arch z-score usually < -3
- ### Location
- Aortic arch: Proximal or distal
- ### Size
- Variable
- ### Morphology
- IAA: Complete anatomic discontinuity between ascending aorta and descending aorta
- HAA: Tubular narrowing of aortic arch
- ## CT Findings
- ### CTA
- Interruption: Blind ending ascending and descending aorta without luminal opacification of arch
- Type, site, and length of interruption
- Type A: Distal to left subclavian artery
- Type B: Between left common carotid and subclavian arteries
- Type C: Between right brachiocephalic and left common carotid arteries
- Hypoplasia: Small caliber of aortic arch
- Best modality for measuring vessel diameters
- Best noninvasive modality to assess aortic arch and supraaortic vessels pattern
- New-generation scanners provide faster acquisition without sedation or ECG gating
- High-resolution 3D reconstructions provides roadmap for surgery
- ## MR Findings
- ### MRA
- High-resolution images of aorta without radiation; can be performed ± contrast
- Types of interrupted arch
- Shows diameters of each aortic segment and length of HAA
- Hypoplasia: External diameter of proximal arch, distal arch, or isthmus measuring < 60%, < 50%, or < 40% of that of ascending aorta
- Transverse aortic arch z-score usually < -3
- This assumes that ascending aorta diameter is normal
- Dynamic MRA shows multiple vascular phases, providing information about aorta, pulmonary arteries and veins, and systemic venous return pattern with single gadolinium injection
- Associated anomalies can be evaluated
- ### MR cine
- Biventricular function assessment, including ejection fraction, end-diastolic, and end-systolic volumes
- Wall motion abnormalities
- Evaluation of additional intracardiac abnormalities (such as septal defects)
- ## Ultrasonographic Findings
- 1st modality to assess aortic arch abnormalities in children
- Define true interruption or HAA and type of IAA by looking at pattern of supraaortic trunks
- Associated patent ductus arteriosus (PDA)
- Size, flow, aortic and pulmonary ostial diameters
- Associated cardiac abnormalities: Atrial septal defect (ASD), ventricular septal defect (VSD), left ventricular outflow tract (LVOT) obstruction, aorticopulmonary window defect
- ## Imaging Recommendations
- ### Best imaging tool
- CTA or MRA
- ### Protocol advice
- Newborn and infants: Contrast injection based on body weight
- Bolus tracking position and HU threshold are variable and depend on scanner speed to start acquisition
- Newborn and infants: Acquisition can be started immediately after contrast injection
# DIFFERENTIAL DIAGNOSIS
- [Coarctation of Aorta](/document/coarctation-of-aorta/c0b23d8c-05e3-4373-b5d9-2de1590414a7)
- Focal narrowing at aortic isthmus
- Same location as type A interruption
- Usually short segment of luminal narrowing
- No complete loss of continuity, like interruption
- Occasionally, extremely tight stenosis may be seen
- More pronounced poststenotic dilation
- In interruption, arch is smaller caliber, and branch vessels are straighter than normal
- With advanced cases, distinguishing features may disappear
- ## Focal Atresia of Aortic Arch
- Most common at aortic isthmus, similar to type A interruption
- Lumen is interrupted, but aortic wall is present
- Fibrous strand between ascending and descending aorta
# PATHOLOGY
- ## General Features
- ### Etiology
- Type A
- Abnormal regression of left 4th aortic arch late in development after left subclavian artery is in position
- Reduced blood flow through 4th aortic arch during embryologic phase
- Insufficient development of aortic arch with spectrum from coarctation to atresia to IAA
- Conal septum not malaligned or deviated; no subaortic stenosis
- Type B
- High association with chromosome 22q11.2 microdeletion
- Abnormal regression of left 4th arch, early in development, before cephalad migration of left subclavian artery
- Malalignment of infundibular septum with muscular septum → LVOT narrowing → decreased growth, hypoplasia, and interruption of arch due to absolute decrease in cardiac output
- Type C
- Abnormal regression of ventral portion of left 3rd and 4th arches
- ### Genetics
- 50% of patients with IAA have chromosome 22q11.2 deletion
- 42% of patients with DiGeorge syndrome have IAA
- ### Associated abnormalities
- IAA
- PDA is essential for life in all patients (seen in 97% of cases)
- VSD in 90% of IAA
- Other congenital heart abnormalities are present in 98%
- Subaortic stenosis
- Bicuspid aortic valve
- Truncus arteriosus
- Aortopulmonary window
- Transposition of great arteries
- Double-outlet right ventricle
- Functional single ventricle
- Persistent 5th arch
- Anomalous origin of subclavian artery
- HAA
- ASD
- VSD
- PDA
- ## Staging, Grading, & Classification
- Type A (13%)
- Interruption distal to left subclavian artery
- Type B (84%)
- Interruption between left common carotid artery and left subclavian artery
- Type C (3%)
- Interruption between right brachiocephalic trunk and left common carotid artery
- In any of these types, 3 subtypes may be seen depending on origin of right subclavian artery
- Subtype 1: Normal subclavian artery origin
- Subtype 2: Aberrant right subclavian artery distal to origin of left subclavian artery
- Subtype 3: Isolated right subclavian artery originating from right ductus arteriosus
# CLINICAL ISSUES
- ## Presentation
- ### Most common signs/symptoms
- Differential cyanosis (ductal right-to-left shunt)
- Type A
- Normal saturation in both arms and head, desaturated legs
- Type B
- Normal saturation in right arm and head, desaturated left arm and legs
- Type C
- Normal saturation in right arm and right carotid artery, desaturated left carotid artery, left arm and legs
- ### Other signs/symptoms
- When ductus arteriosus begins to close, neonate develops signs of hypoperfusion and cardiogenic shock
- Death usually occurs 4-10 days after closure of ductus arteriosus
- By 1 month, 76% of untreated infants are dead; by 1 year, > 90% are dead
- ## Demographics
- ### Age
- Neonates
- ### Sex
- Male patients: 59%
- Female patients: 41%
- ### Epidemiology
- Rare condition
- 1% of congenital heart disease
- 2/100,000 live births
- ## Natural History & Prognosis
- When untreated and ductus arteriosus closes, distal hypoperfusion leads to renal failure, lactic acidosis, and eventually death in few days
- ## Treatment
- Surgical correction is only treatment; goal is to establish continuity in aortic arch
- Prostaglandin E₁ is given to maintain patency of ductus arteriosus until neonate is stable for surgical correction
4e578d09-68e6-4af7-8a56-23527ab96783
## References
# Selected References
1. [Evans WN et al: Prenatal diagnosis of hypoplastic aortic arch without intracardiac malformations: the nevada experience. J Card Surg. 37(11):3705-10, 2022](http://www.ncbi.nlm.nih.gov/pubmed/?term=36047366%5Bpmid%5D)
1. [LaPar DJ et al: Surgical considerations in interrupted aortic arch. Semin Cardiothorac Vasc Anesth. 22(3):278-84, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=29774793%5Bpmid%5D)
1. [Hanneman K et al: Congenital variants and anomalies of the aortic arch. Radiographics. 37(1):32-51, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=27860551%5Bpmid%5D)
1. [Goudar SP et al: Echocardiography of coarctation of the aorta, aortic arch hypoplasia, and arch interruption: strategies for evaluation of the aortic arch. Cardiol Young. 26(8):1553-62, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=28148317%5Bpmid%5D)
1. [Roubertie F et al: Aortopulmonary window and the interrupted aortic arch: midterm results with use of the single-patch technique. Ann Thorac Surg. 99(1):186-91, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=25440264%5Bpmid%5D)
1. [Ramos-Duran L et al: Developmental aortic arch anomalies in infants and children assessed with CT angiography. AJR Am J Roentgenol. 198(5):W466-74, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22528928%5Bpmid%5D)
1. [Hellinger JC et al: Congenital thoracic vascular anomalies: evaluation with state-of-the-art MR imaging and MDCT. Radiol Clin North Am. 49(5):969-96, 2011](http://www.ncbi.nlm.nih.gov/pubmed/?term=21889017%5Bpmid%5D)
1. [Frank L et al: Cardiovascular MR imaging of conotruncal anomalies. Radiographics. 30(4):1069-94, 2010](http://www.ncbi.nlm.nih.gov/pubmed/?term=20631369%5Bpmid%5D)
1. [Kimura-Hayama ET et al: Uncommon congenital and acquired aortic diseases: role of multidetector CT angiography. Radiographics. 30(1):79-98, 2010](http://www.ncbi.nlm.nih.gov/pubmed/?term=20083587%5Bpmid%5D)
1. [Dillman JR et al: Interrupted aortic arch: spectrum of MRI findings. AJR Am J Roentgenol. 190(6):1467-74, 2008](http://www.ncbi.nlm.nih.gov/pubmed/?term=18492893%5Bpmid%5D)
1. [Yang DH et al: Multislice CT angiography of interrupted aortic arch. Pediatr Radiol. 38(1):89-100, 2008](http://www.ncbi.nlm.nih.gov/pubmed/?term=17965856%5Bpmid%5D)
1. [Loffredo CA et al: Interrupted aortic arch: an epidemiologic study. Teratology. 61(5):368-75, 2000](http://www.ncbi.nlm.nih.gov/pubmed/?term=10777832%5Bpmid%5D)
1. [Kaulitz R et al: Echocardiographic assessment of interrupted aortic arch. Cardiol Young. 9(6):562-71, 1999](http://www.ncbi.nlm.nih.gov/pubmed/?term=10593265%5Bpmid%5D)
1. [Reardon MJ et al: Interrupted aortic arch: brief review and summary of an eighteen-year experience. Tex Heart Inst J. 11(3):250-9, 1984](http://www.ncbi.nlm.nih.gov/pubmed/?term=15227058%5Bpmid%5D)
1. [CELORIA GC et al: Congenital absence of the aortic arch. Am Heart J. 58:407-13, 1959](http://www.ncbi.nlm.nih.gov/pubmed/?term=13808756%5Bpmid%5D)
## Images
### Selected Images
 with an aberrant right subclavian artery
with an aberrant right subclavian artery  . Also note the collateral vessel
. Also note the collateral vessel  with right carotid artery
with right carotid artery  . Left carotid artery
. Left carotid artery  and left subclavian artery (LSA)
and left subclavian artery (LSA)  are also shown.](images/app.statdx.com_image_thumbnail_f2636f4c-961f-4d6f-956c-ddc9cb319a6c_annotated_true_size_900_quality_90_248c7a5708a7b6d2e556e82809d8117dc7bb3f46.jpg)
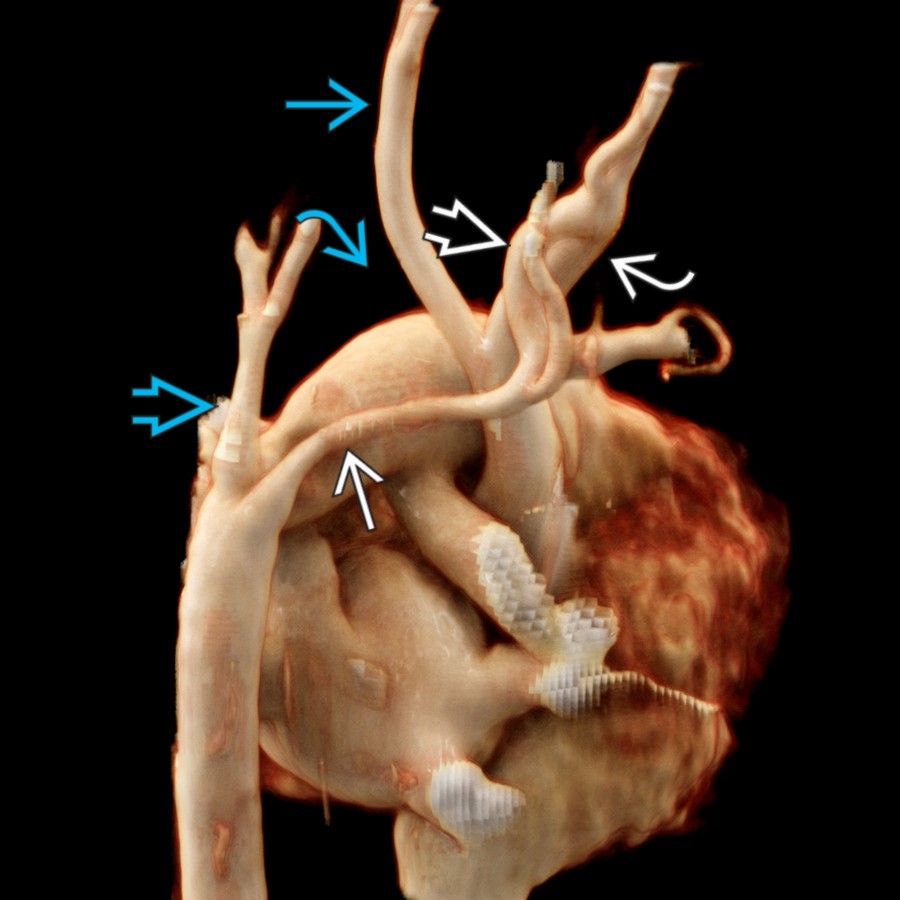
*Posterior oblique CTA cinematic rendering shows type B interrupted aortic arch with an aberrant right subclavian artery . Also note the collateral vessel with right carotid artery . Left carotid artery and left subclavian artery (LSA) are also shown.*

*Posterior oblique CTA cinematic rendering shows type B interrupted aortic arch with an aberrant right subclavian artery . Also note the collateral vessel with right carotid artery . Left carotid artery and left subclavian artery (LSA) are also shown.*

*Anterosuperior oblique CTA cinematic rendering shows type B interrupted aortic arch (IAA) with aberrant right subclavian artery . Patent ductus arteriosus (PDA) provides blood flow to both subclavian arteries and the distal descending aorta (DA).*

*Sagittal oblique MIP CTA shows a hypoplastic aortic arch and PDA .*
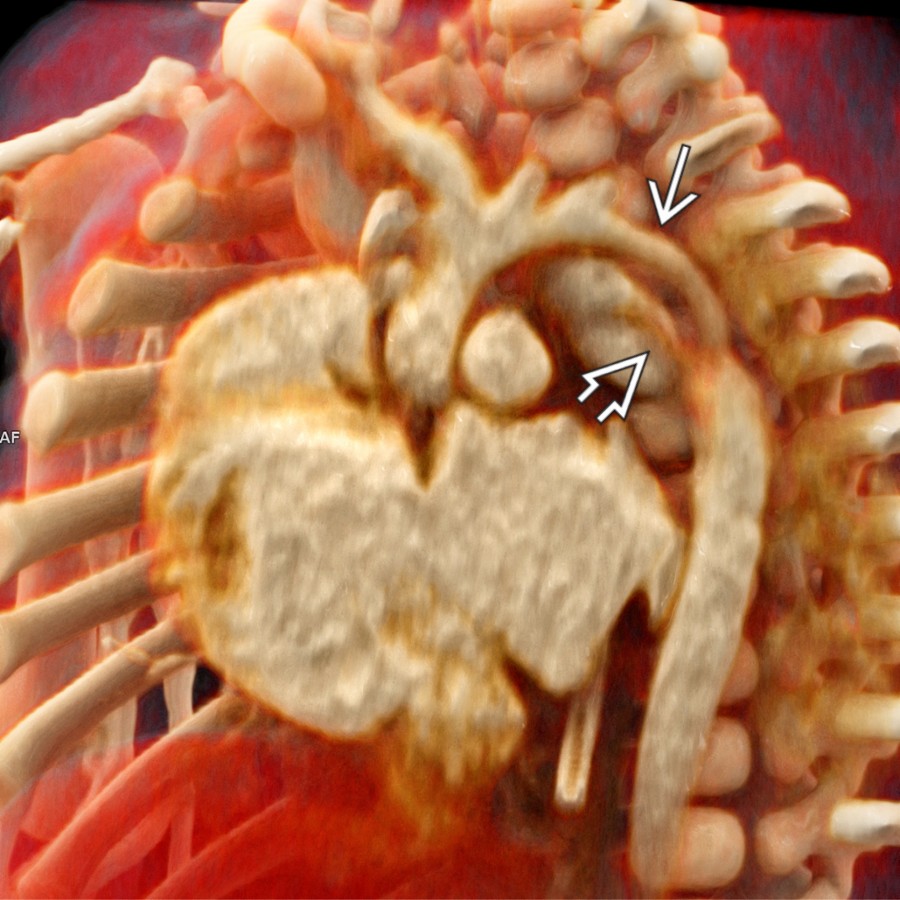
*Sagittal oblique CTA cinematic rendering in the same patient shows a hypoplastic aortic arch and PDA . CT is the best noninvasive imaging modality to assess aortic arch and supraaortic vessel patterns as well as to measure vessel diameters.*

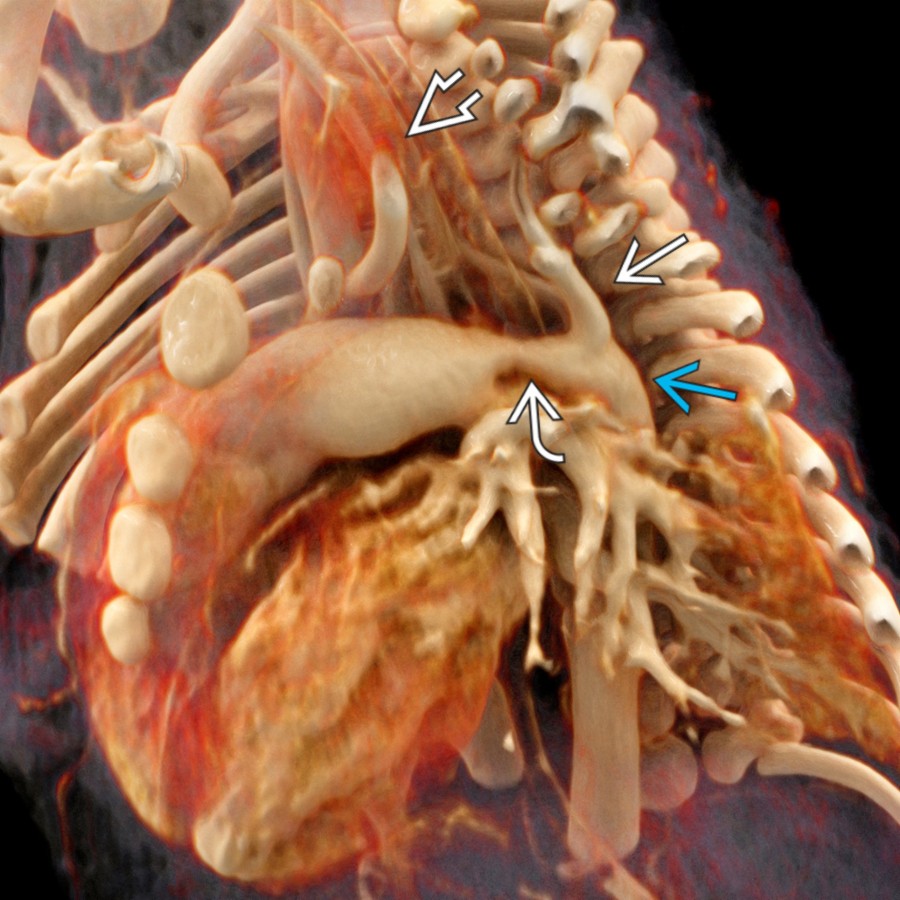
*Anterosuperior oblique CTA cinematic rendering shows type B IAA. The brachiocephalic trunk (BCT) and left carotid artery originate from the proximal aorta. The LSA originates from the ductal arch.*
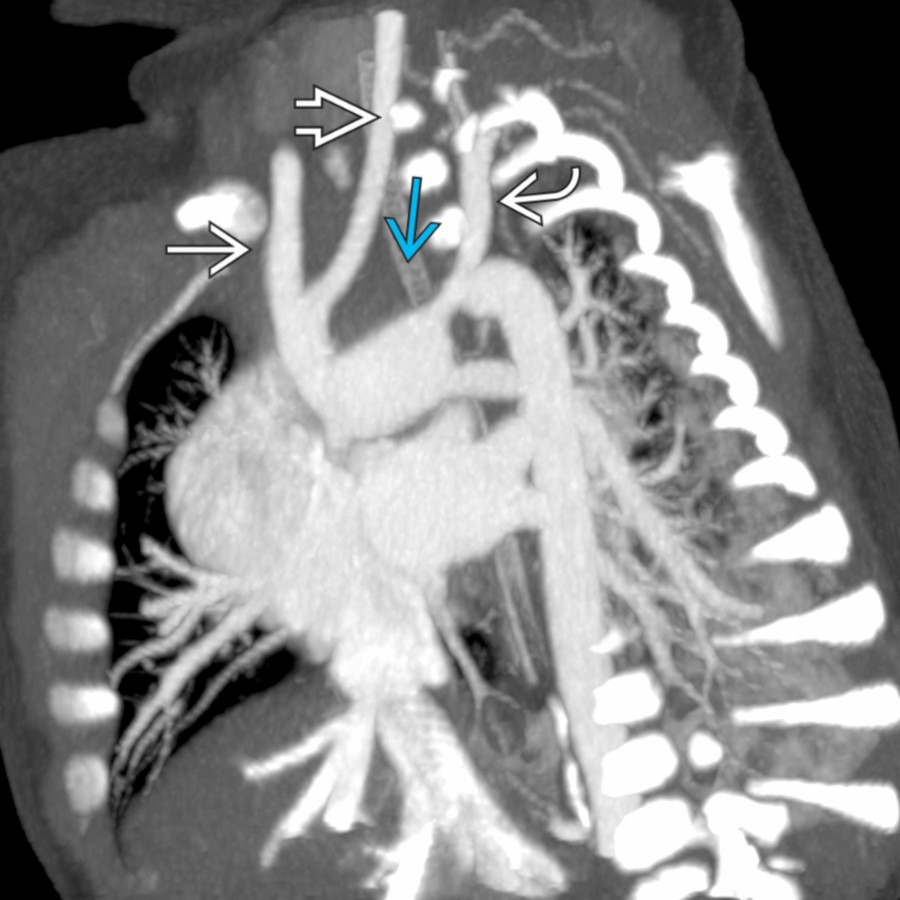
*Sagittal oblique MIP CTA shows type B IAA . The BCT and left common carotid artery (LCC) originate from the proximal aorta. The LSA originates from the ductal arch.*
*CTA cinematic rendering demonstrates type B IAA. The LSA originates from the DA . The BCT and LCC originate from the proximal ascending aorta (AA). The PDA provides blood flow to both the LSA and DA.*

*Sagittal oblique CTA cinematic rendering shows a hypoplastic distal aortic arch involving the isthmus and proximal DA .*
*Posterior oblique CTA cinematic rendering shows type B interrupted aortic arch with an aberrant right subclavian artery . Also note the collateral vessel with right carotid artery . Left carotid artery and left subclavian artery (LSA) are also shown.*

*Posterior oblique CTA cinematic rendering shows type B interrupted aortic arch with an aberrant right subclavian artery . Also note the collateral vessel with right carotid artery . Left carotid artery and left subclavian artery (LSA) are also shown.*

*Anterosuperior oblique CTA cinematic rendering shows type B interrupted aortic arch (IAA) with aberrant right subclavian artery . Patent ductus arteriosus (PDA) provides blood flow to both subclavian arteries and the distal descending aorta (DA).*

*Sagittal oblique MIP CTA shows a hypoplastic aortic arch and PDA .*

*Sagittal oblique CTA cinematic rendering in the same patient shows a hypoplastic aortic arch and PDA . CT is the best noninvasive imaging modality to assess aortic arch and supraaortic vessel patterns as well as to measure vessel diameters.*

*Anterosuperior oblique CTA cinematic rendering shows type B IAA. The brachiocephalic trunk (BCT) and left carotid artery originate from the proximal aorta. The LSA originates from the ductal arch.*

*Sagittal oblique MIP CTA shows type B IAA . The BCT and left common carotid artery (LCC) originate from the proximal aorta. The LSA originates from the ductal arch.*

*CTA cinematic rendering demonstrates type B IAA. The LSA originates from the DA . The BCT and LCC originate from the proximal ascending aorta (AA). The PDA provides blood flow to both the LSA and DA.*

*Sagittal oblique CTA cinematic rendering shows a hypoplastic distal aortic arch involving the isthmus and proximal DA .*
 between the AA and main pulmonary artery (MPA)
between the AA and main pulmonary artery (MPA)  . A PDA supplies the DA . PA branches
. A PDA supplies the DA . PA branches  are visible.](images/app.statdx.com_image_thumbnail_58e07e18-2a6b-48d3-bd2e-2ba26962f0dc_annotated_true_size_900_quality_90_900714405780c8b667e7f030ae56c9429ecf3574.jpg)
*Neonate with type A IAA shows AA terminating as the BCT , LCC , and LSA (left). Notice the AP window defect between the AA and main pulmonary artery (MPA) . A PDA supplies the DA . PA branches are visible.*

*Coronal (left) and sagittal (right) images in a neonate with type B IAA show the AA terminating as the BCT and LCC . The LSA and DA are supplied by a PDA . PA branches arise from the MPA. (Courtesy S. Kligerman, MD.)*
### Additional Images

*CTA cinematic rendering demonstrates a hypoplastic aortic arch with severe coarctation . Note the decreased diameter of the aortic arch due to hypoplasia.*

*Sagittal oblique MIP CTA in the same patient demonstrates decreased diameter of the aortic arch due to a hypoplastic aortic arch and associated severe aortic coarctation .*

*Coronal (left) and sagittal (right) oblique images in a 1-day-old with type B IAA show a hypoplastic ascending aorta terminating as the right common carotid and left common carotid arteries. The PDA supplies the descending thoracic aorta (DTA) . A portion of the LSA is seen from the DTA.*

*Coronal image in the same patient shows that an aberrant right subclavian artery arises from the DTA distal to the LSA , making this a type B IAA, subtype 2.*

*3D image in a neonate with type B IAA shows the ascending aorta terminating as the right BCT and LCC . The PDA supplies the descending thoracic aorta and LSA . (Courtesy S. Kligerman, MD.)*
are visible.](images/app.statdx.com_image_thumbnail_58e07e18-2a6b-48d3-bd2e-2ba26962f0dc_annotated_true_size_900_quality_90_900714405780c8b667e7f030ae56c9429ecf3574.jpg)
*Neonate with type A IAA shows AA terminating as the BCT , LCC , and LSA (left). Notice the AP window defect between the AA and main pulmonary artery (MPA) . A PDA supplies the DA . PA branches are visible.*

*Coronal (left) and sagittal (right) images in a neonate with type B IAA show the AA terminating as the BCT and LCC . The LSA and DA are supplied by a PDA . PA branches arise from the MPA. (Courtesy S. Kligerman, MD.)*
### Additional Images

*CTA cinematic rendering demonstrates a hypoplastic aortic arch with severe coarctation . Note the decreased diameter of the aortic arch due to hypoplasia.*

*Sagittal oblique MIP CTA in the same patient demonstrates decreased diameter of the aortic arch due to a hypoplastic aortic arch and associated severe aortic coarctation .*

*Coronal (left) and sagittal (right) oblique images in a 1-day-old with type B IAA show a hypoplastic ascending aorta terminating as the right common carotid and left common carotid arteries. The PDA supplies the descending thoracic aorta (DTA) . A portion of the LSA is seen from the DTA.*

*Coronal image in the same patient shows that an aberrant right subclavian artery arises from the DTA distal to the LSA , making this a type B IAA, subtype 2.*

*3D image in a neonate with type B IAA shows the ascending aorta terminating as the right BCT and LCC . The PDA supplies the descending thoracic aorta and LSA . (Courtesy S. Kligerman, MD.)*