---
title: "Neuromyelitis Optica Spectrum Disorders"
docid: "54d4a8bc-9267-4df6-98c1-f22aae051d01"
authors:
- key: "a25c450b-3d34-4f64-bba3-cc0834813df6"
value: "Miral D. Jhaveri, MD, MBA"
breadcrumbs:
-
name: "Brain"
slug: "brain"
treeNodeId: "6d8829f1-14d7-45af-8675-255189aa526a"
-
name: "Diagnosis"
slug: "diagnosis"
treeNodeId: "51c00394-446e-4a38-94af-d3b1d14d34e8"
-
name: "Pathology-Based Diagnoses"
slug: "pathology-based-diagnoses"
treeNodeId: "d9d3a8ed-f21b-4831-8c77-591a3500ef77"
-
name: "Infectious, Inflammatory, and Demyelinating Disease"
slug: "infectious-inflammatory-and-demyel-"
treeNodeId: "7210f860-fe5f-4a2d-81cc-4fe06c769607"
-
name: "Inflammatory and Demyelinating Disease"
slug: "inflammatory-and-demyelinating-dis-"
treeNodeId: "62ab4dc3-dbf6-45a9-8532-f0e962aa62dc"
-
name: "Neuromyelitis Optica Spectrum Disorders"
slug: "neuromyelitis-optica-spectrum-diso-"
treeNodeId: null
category: "Brain"
documentVersionId: "e640534a-1c8b-4d12-970e-c0994fbfc239"
imageCount: 22
lastUpdated: "07/28/20"
pageDescription: "Neuromyelitis Optica Spectrum Disorders"
pageKeywords: "Brain, Diagnosis, Pathology-Based Diagnoses, Infectious, Inflammatory, and Demyelinating Disease, Inflammatory and Demyelinating Disease, Neuromyelitis Optica Spectrum Disorders"
pageTitle: "Neuromyelitis Optica Spectrum Disorders | STATdx"
enhancedTitle: "Neuromyelitis Optica Spectrum Disorders"
type: "DX"
references: true
tables: 1
breadcrumbs:
- "Brain"
- "Diagnosis"
- "Pathology-Based Diagnoses"
- "Infectious, Inflammatory, and Demyelinating Disease"
- "Inflammatory and Demyelinating Disease"
- "Neuromyelitis Optica Spectrum Disorders"
---
# KEY FACTS
- ## Terminology
- Neuromyelitis optica spectrum disorders (NMOSDs)
- MOG antibody-associated disease (MOG-AAD)
- Autoimmune inflammatory demyelinating disease of CNS with preferential involvement of optic nerves and spinal cord, AQP4 antibody (+/-)
- ## Imaging
- Hyperintense, mildly enlarged optic nerves + enhancement
- **AQP4 antibody (+)**:****More posterior involvement, including chiasm
- **MOG-AAD**:****More anterior optic nerve involvement
- Expansile, hyperintense cord signal, ≥ 3 segments
- Brain lesions in NMOSD are distinct from multiple sclerosis (MS)
- Acute cord lesions show patchy enhancement
- Patchy enhancement with blurred margins (cloud-like enhancement) in cerebral lesions
- "Pencil-thin" ependymal enhancement
- ## Top Differential Diagnoses
- MS, acute disseminated encephalomyelitis (ADEM)
- Optic neuritis, transverse myelitis
- Spinal cord neoplasm, neurosarcoid
- ## Pathology
- NMO antibody: IgG autoantibody that binds to AQP4
- **AQP4-IgG** is 90% specific and 70-75% sensitive for NMOSD
- **AQP4-IgG (-) NMOSD** less common (10-25%)
- Minority of AQP4-IgG (-) patients with phenotype of NMOSD are MOG-IgG (+)
- 2015 International Panel for NMO Diagnosis (IPND) developed revised diagnostic criteria for NMOSD stratified by serologic testing (NMOSD with or without AQP4-IgG)
- ## Clinical Issues
- Impaired vision, myelopathy, brainstem syndrome
- Relapsing course in 85-90% of patients
- Acute exacerbation: Steroids, plasmapheresis
# TERMINOLOGY
- ## Abbreviations
- Neuromyelitis optica spectrum disorders (NMOSDs)
- Aquaporin-4 (AQP4)
- Myelin oligodendrocyte glycoprotein (MOG)
- MOG antibody-associated disease (MOG-AAD)
- ## Synonyms
- Devic syndrome
- ## Definitions
- Autoimmune inflammatory demyelinating disease of CNS with preferential involvement of optic nerves and spinal cord, AQP4 antibody (+/-)
# IMAGING
- ## General Features
- ### Best diagnostic clue
- Optic neuritis and myelitis
- Spectrum of lesions atypical for multiple sclerosis (MS)
- ### Location
- **AQP4 antibody (+)**
- Spinal cord: More common cervicomedullary junction
- Optic nerves: More posterior involvement of optic nerve, including chiasm, bilateral disease
- Brain lesions: Deep white matter, periependymal regions, corpus callosum, corticospinal tracts, brainstem, and cerebellum
- **MOG-AAD**
- Spinal cord: More likely thoracolumbar and conus
- Optic nerves: Long, bilateral, anterior optic nerve
- Brain lesions: Basal ganglia, thalamus, infratentorial (brainstem, cerebellar peduncles, around 4th ventricle)
- ### Size
- Spinal lesions typically expansile, multisegment
- Brain lesions punctate or small (< 3 mm) to large, confluent in cerebral white matter
- ## MR Findings
- ### T2WI
- Hyperintense, mildly enlarged optic nerves
- **AQP4 antibody (+)**:****More posterior involvement, including chiasm
- **MOG-AAD**: More anterior optic nerve involvement
- Expansile, hyperintense cord signal, ≥ 3 segments → longitudinally extensive transverse myelitis (LETM)
- May have heterogeneous areas of brighter T2 signal
- Central/central and peripheral, > 50% cord area
- ### STIR
- Hyperintense optic nerve
- LETM: Central gray matter/central and peripheral, > 50% cord area
- ### FLAIR
- Brain lesions are quite characteristic and distinct from lesions in MS
- Hyperintense brain lesions in AQP4 antibody (+) NMOSD correspond to sites of high AQP4 expression
- Adjacent to ventricular system at any level
- **Periependymal surrounding 3rd ventricle and cerebral aqueduct**
- Thalamus, hypothalamus, ventral midbrain
- **Dorsal brainstem adjacent to 4th ventricle**
- Including area postrema and nucleus tracts solitarius
- **Periventricular surrounding lateral ventricles**
- Follow ependymal lining in disseminated pattern
- Often edematous and heterogeneous, creating marbled pattern unlike MS
- Complete thickness of splenium in unique arch bridge pattern
- Chronic lesions reduce in size and intensity; may even disappear
- Cystic changes and atrophy of corpus callosum
- **Lesions involving corticospinal tracts**
- Unilateral or bilateral, posterior limb internal capsule, cerebral peduncle
- Contiguous, often longitudinally extensive
- **Extensive hemispheric lesions**
- Tumefactive (> 3 cm), long spindle-like, or radial
- Occasionally mimicking posterior reversible encephalopathy syndrome (PRES)
- **Nonspecific lesions: Not unique, but most common**
- Nonspecific punctate or small (< 3 mm) dots or patches of hyperintensities in subcortical or deep white matter
- **MOG-AAD** lesions tend to involve deep gray matter and infratentorial parenchyma
- ### DWI
- ↑ diffusivity, ↓ fractional anisotropy than MS patients or controls
- Patient with NMOSD and normal brain MR
- DTI shows ↑ mean diffusivity in corticospinal tract and optic radiation, but not in cingulum or corpus callosum
- ### T1WI C+
- Long-segment optic nerve enhancement unilateral or bilateral, often extending posterior to optic chiasm
- Acute lesions in cord show patchy enhancement
- Most brain lesions do not show enhancement
- Patchy enhancement with blurred margins (cloud-like enhancement) in cerebral lesions
- Relatively specific for NMOSD
- "Pencil-thin" ependymal enhancement
- Rarely, well-marginated nodular enhancement, leptomeningeal enhancement
- ### MRS
- In NMOSD, metabolites are normal in normal-appearing white matter (NAWM) and normal-appearing gray matter (NAGM) compared to patients with MS
- In MS, NAA ↓ and choline ↑ in NAWM
- ## Imaging Recommendations
- ### Best imaging tool
- Contrast-enhanced MR of brain, spine, and orbits
- ### Protocol advice
- Orbits: Axial and coronal STIR/T2 FS and T1 C+ FS
- Spine: Sagittal STIR/T2, T1WI C+
- Brain: Axial and sagittal FLAIR, T1WI C+
# DIFFERENTIAL DIAGNOSIS
- [Multiple Sclerosis](/document/multiple-sclerosis/7892b2a2-f52a-4d7f-9858-a326f2b7ab04)
- Radially oriented, perivenular lesions (Dawson fingers)
- Optic neuritis, typically unilateral, shorter segment
- Myelitis, usually smaller longitudinal extension, peripheral
- [Acute Disseminated Encephalomyelitis](/document/adem/a3fafeb7-5861-4364-beb8-c0e30220564e)
- Bilateral, asymmetric involvement of supratentorial and infratentorial, white matter and gray matter lesions
- Common in children and young adults
- LETM similar to NMOSD
- [Optic Neuritis](/document/optic-neuritis/ac9c8fc9-33cd-4716-a509-2542ec5579ca)
- 1 component of NMOSD
- Consider NMOSD in case of 1st optic neuritis, but otherwise normal brain MR
- [Transverse Myelitis](/document/idiopathic-acute-transverse-myelit-/6e774628-d7ad-48f1-9847-e09a4fad168b)
- 1 component of NMOSD
- Idiopathic inflammatory or postinfectious myelitis
- Differentiation from other immune-mediated myelitis like Sjögren disease or SLE difficult
- [Spinal Cord Neoplasm](/document/spinal-cord-astrocytoma/43d5efa2-7a6d-4972-bfc6-c300cc31f9af)
- Astrocytoma or ependymoma can show similar multisegment cord T2 hyperintensity and enhancement
- [Neurosarcoid](/document/neurosarcoid/fef69139-0019-4be3-9bdc-e26bc3644251)
- Parenchymal granulomas near hypothalamus, visual pathway
- Optic nerve involvement bilateral, extensive, resemble NMOSD
- Nodular leptomeningeal, dural, and cranial nerve enhancement
- Systemic manifestations, (+) chest x-ray
# PATHOLOGY
- ## General Features
- NMO antibody: IgG autoantibody that binds to AQP4
- AQP4 channel is most abundant water channel in CNS
- Located in foot processes of astrocytes
- Highly expressed in optic nerve, spinal cord, periventricular areas, hypothalamus, subpial regions, brainstem, area postrema
- **AQP4-IgG** can be identified in other autoimmune disorders, myasthenia gravis, SLE, Sjögren syndrome, RA
- Rare clinical coexistence of anti-*n*-methyl-*d*-aspartate (NMDA) receptor encephalitis and NMOSD
- **AQP4-IgG** is 90% specific and 70-75% sensitive for NMOSD
- **AQP4-IgG (-) NMOSD** less common (10-25%)
- Minority of AQP4-IgG (-) patients with phenotype of NMOSD are MOG-IgG (+)
- MOG antibody targets oligodendrocytes
- MOG-IgG also found in association with other demyelinating disorders, such as MS, acute disseminated encephalomyelitis (ADEM), optic neuritis, LETM
- Controversial if MOG-AAD distinct entity or part of NMOSD
- ## Microscopic Features
- Selective AQP4 immunoreactivity loss, vasculocentric complement, immunoglobulin deposition characteristic
# CLINICAL ISSUES
- ## Presentation
- ### Most common signs/symptoms
- Optic neuritis: Impaired or double vision
- Myelitis: Myelopathy
- Brainstem symptoms: Nystagmus, dysarthria, dysphagia, ataxia, ophthalmoplegia
- Area postrema syndrome: Hiccups, nausea, vomiting
- Symptomatic narcolepsy or acute diencephalic syndrome
- ### Clinical profile
- CSF: Pleocytosis, ↑ protein, (-) oligoclonal bands
- ## Demographics
- 1st symptoms commonly between 32-45 years of age
- 15-20% of patients over age 60 at onset
- NMOSD worldwide disease
- AQP4(+) NMOSD, F:M ratio is 8-9:1
- MOG-AAD usually younger age at onset, F:M ratio is ~ 1:1
- ## Natural History & Prognosis
- Relapsing course in 85-90% of patients
- Worse prognosis with more severe disability than MS
- Anti-AQP4 antibody (+): High risk of further relapses
- MOG-AAD: More likely to be monophasic, fewer relapses
- ## Treatment
- Acute exacerbation: Steroids
- Plasma exchange in relapses not responding to steroids
- Prevention of relapses: Immunosuppression, eculizumab
- Symptom management and rehabilitation
# DIAGNOSTIC CHECKLIST
- ## Consider
- NMOSD in patient with optic neuritis and myelitis
- Characteristic brain lesions involving periependymal regions, corpus callosum, corticospinal tracts, brainstem
9e0e24a9-6707-4e55-9895-fe13a49f7c8e
## References
# Selected References
1. [Rosenthal JF et al: CNS inflammatory demyelinating disorders: MS, NMOSD and MOG antibody associated disease. J Investig Med. 68(2):321-30, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=31582425%5Bpmid%5D)
1. [Salama S et al: MRI differences between MOG antibody disease and AQP4 NMOSD. Mult Scler. 1352458519893093, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=31937191%5Bpmid%5D)
1. [Fujihara K: Neuromyelitis optica spectrum disorders: still evolving and broadening. Curr Opin Neurol. 32(3):385-94, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30893099%5Bpmid%5D)
1. [Huda S et al: Neuromyelitis optica spectrum disorders. Clin Med (Lond). 19(2):169-76, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30872305%5Bpmid%5D)
1. [Wynford-Thomas R et al: Neurological update: MOG antibody disease. J Neurol. 266(5):1280-6, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30569382%5Bpmid%5D)
1. [Dutra BG et al: Neuromyelitis optica spectrum disorders: spectrum of MR imaging findings and their differential diagnosis. Radiographics. 38(1):169-93, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=29320331%5Bpmid%5D)
1. [Narayan R et al: MOG antibody disease: a review of MOG antibody seropositive neuromyelitis optica spectrum disorder. Mult Scler Relat Disord. 25:66-72, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=30048919%5Bpmid%5D)
1. [Kim HJ et al: MRI characteristics of neuromyelitis optica spectrum disorder: an international update. Neurology. 84(11):1165-73, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=25695963%5Bpmid%5D)
1. [Wingerchuk DM et al: International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. 85(2):177-89, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=26092914%5Bpmid%5D)
1. [Barnett Y et al: Conventional and advanced imaging in neuromyelitis optica. AJNR Am J Neuroradiol. 35(8):1458-66, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=23764723%5Bpmid%5D)
1. [Kawachi I et al: [Characteristic features of radiological findings in multiple sclerosis and neuromyelitis optica.] Nihon Rinsho. 72(11):1976-82, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=25518380%5Bpmid%5D)
1. [Uzawa A et al: Neuromyelitis optica: concept, immunology and treatment. J Clin Neurosci. 21(1):12-21, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=23916471%5Bpmid%5D)
1. [Jacob A et al: Current concept of neuromyelitis optica (NMO) and NMO spectrum disorders. J Neurol Neurosurg Psychiatry. 84(8):922-30, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=23142960%5Bpmid%5D)
1. [Sato DK et al: Clinical spectrum and treatment of neuromyelitis optica spectrum disorders: evolution and current status. Brain Pathol. 23(6):647-60, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=24118482%5Bpmid%5D)
1. [Kim W et al: Brain abnormalities in neuromyelitis optica spectrum disorder. Mult Scler Int. 2012:735486, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=23259063%5Bpmid%5D)
1. [Lana-Peixoto MA et al: The expanded spectrum of neuromyelitis optica: evidences for a new definition. Arq Neuropsiquiatr. 70(10):807-13, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=23060108%5Bpmid%5D)
1. [Benavente E et al: Neuromyelitis optica-AQP4: an update. Curr Rheumatol Rep. 13(6):496-505, 2011](http://www.ncbi.nlm.nih.gov/pubmed/?term=21922173%5Bpmid%5D)
1. [Cree B: Neuromyelitis optica: diagnosis, pathogenesis, and treatment. Curr Neurol Neurosci Rep. 8(5):427-33, 2008](http://www.ncbi.nlm.nih.gov/pubmed/?term=18713580%5Bpmid%5D)
1. [Jacob A et al: Treatment of neuromyelitis optica with rituximab: retrospective analysis of 25 patients. Arch Neurol. 65(11):1443-8, 2008](http://www.ncbi.nlm.nih.gov/pubmed/?term=18779415%5Bpmid%5D)
1. [Li Y et al: Brain magnetic resonance imaging abnormalities in neuromyelitis optica. Acta Neurol Scand. 118(4):218-25, 2008](http://www.ncbi.nlm.nih.gov/pubmed/?term=18384459%5Bpmid%5D)
1. [Jarius S et al: NMO-IgG in the diagnosis of neuromyelitis optica. Neurology. 68(13):1076-7, 2007](http://www.ncbi.nlm.nih.gov/pubmed/?term=17287449%5Bpmid%5D)
1. [Matiello M et al: Neuromyelitis optica. Curr Opin Neurol. 20(3):255-60, 2007](http://www.ncbi.nlm.nih.gov/pubmed/?term=17495617%5Bpmid%5D)
1. [Benedetti B et al: Grading cervical cord damage in neuromyelitis optica and MS by diffusion tensor MRI. Neurology. 67(1):161-3, 2006](http://www.ncbi.nlm.nih.gov/pubmed/?term=16832101%5Bpmid%5D)
1. [Pittock SJ et al: Brain abnormalities in neuromyelitis optica. Arch Neurol. 63(3):390-6, 2006](http://www.ncbi.nlm.nih.gov/pubmed/?term=16533966%5Bpmid%5D)
1. [Wingerchuk DM et al: Revised diagnostic criteria for neuromyelitis optica. Neurology. 66(10):1485-9, 2006](http://www.ncbi.nlm.nih.gov/pubmed/?term=16717206%5Bpmid%5D)
## Tables
# 2015 IPND Criteria for NMOSD
| AQP4-IgG (+) Status | AQP4-IgG (-) or Unknown Status |
| --- | --- |
| AQP4-IgG positivity + 1 core clinical characteristic | At least 2 core clinical characteristics; 1 must be optic neuritis, LETM, or area postrema syndrome |
| - Optic neuritis - Acute myelitis - Area postrema syndrome Unexplained hiccups, or nausea and vomiting | If optic neuritis, MR with - Normal brain or nonspecific white matter lesions or - T2-hyperintense or T1 C+ enhancing optic nerve involving chiasm or > 50% of optic nerve |
| - Acute brainstem syndrome | If acute myelitis, MR with - Intramedullary lesion over 3 contiguous segments, or - Focal atrophy of at least 3 contiguous segments |
| - Symptomatic narcolepsy or diencephalic syndrome With NMOSD-typical diencephalic MR lesions | If area postrema syndrome, MR with - Dorsal medullary/area postrema lesion(s) |
| - Symptomatic cerebral syndrome With NMOSD-typical brain lesions | If acute brainstem syndrome, MR with - Periependymal brainstem lesions |
## Images
### Selected Images
 of the intraorbital segment of the right optic nerve.](images/app.statdx.com_image_thumbnail_e8ba18d2-7677-4bf1-8a89-ea3f7610a1dd_annotated_true_size_900_quality_90_503cf50a_20251018T122510Z.jpg)
*Axial T1 C+ MR in a 22-year-old woman with right vision loss demonstrates swelling with enhancement of the intraorbital segment of the right optic nerve.*

*Axial T1 C+ MR in a 22-year-old woman with right vision loss demonstrates swelling with enhancement of the intraorbital segment of the right optic nerve.*

*Axial T1 C+ MR in a 22-year-old woman with right vision loss demonstrates swelling with enhancement of the intraorbital segment of the right optic nerve.*

*Axial T1 C+ MR in a 22-year-old woman with right vision loss demonstrates swelling with enhancement of the intraorbital segment of the right optic nerve.*

*Axial T1 C+ MR in a 22-year-old woman with right vision loss demonstrates swelling with enhancement of the intraorbital segment of the right optic nerve.*

*Axial T1 C+ MR in a 22-year-old woman with right vision loss demonstrates swelling with enhancement of the intraorbital segment of the right optic nerve.*
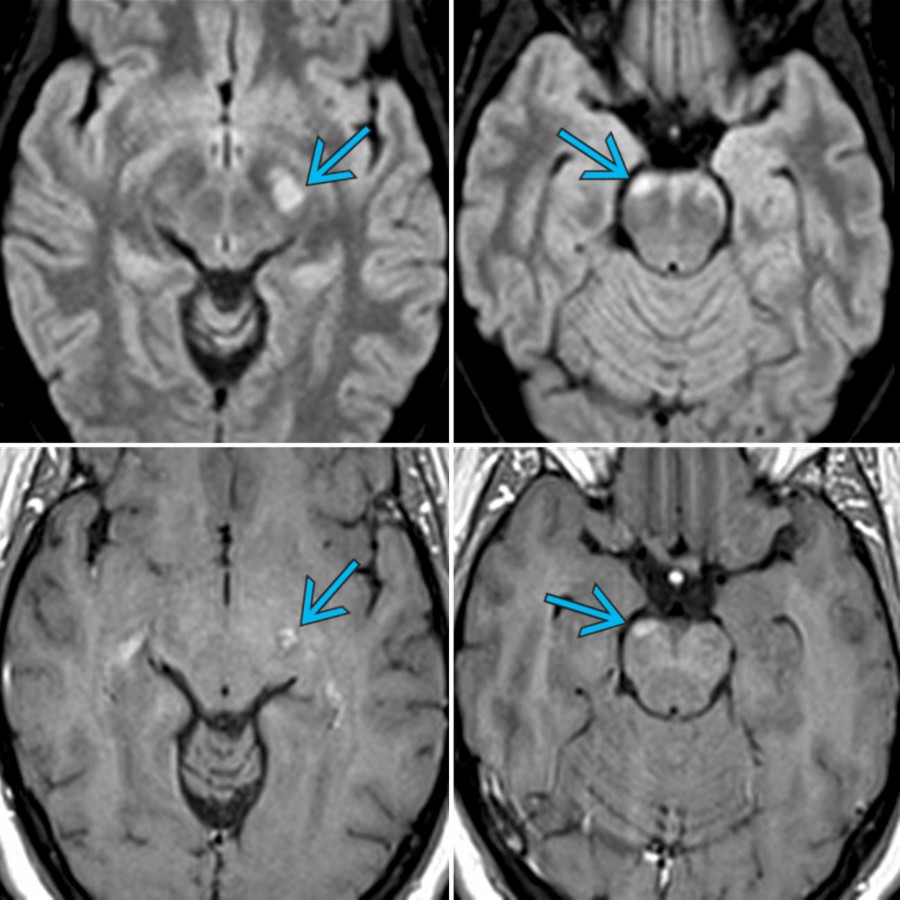
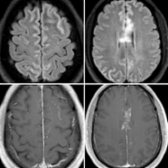
 along the cerebral peduncles. AQP4 antibody was positive in this patient with NMOSD. Brain lesions in NMOSD typically involve the deep white matter, periependymal regions, corpus callosum, corticospinal tracts, brainstem, and cerebellum.](images/app.statdx.com_image_thumbnail_d26008df-62a0-4116-a5a3-ebf9f767936e_annotated_true_size_900_quality_90_95e09ab2_20251018T122510Z.jpg)
*Axial FLAIR MR (top) and T1 C+ MR (bottom) images in the same patient show hyperintense enhancing lesions along the cerebral peduncles. AQP4 antibody was positive in this patient with NMOSD. Brain lesions in NMOSD typically involve the deep white matter, periependymal regions, corpus callosum, corticospinal tracts, brainstem, and cerebellum.*
*Axial FLAIR MR (top) and T1 C+ MR (bottom) images in the same patient show hyperintense enhancing lesions along the cerebral peduncles. AQP4 antibody was positive in this patient with NMOSD. Brain lesions in NMOSD typically involve the deep white matter, periependymal regions, corpus callosum, corticospinal tracts, brainstem, and cerebellum.*
*Axial FLAIR MR (top) and T1 C+ MR (bottom) images in the same patient show hyperintense enhancing lesions along the cerebral peduncles. AQP4 antibody was positive in this patient with NMOSD. Brain lesions in NMOSD typically involve the deep white matter, periependymal regions, corpus callosum, corticospinal tracts, brainstem, and cerebellum.*

*Axial FLAIR MR (top) and T1 C+ MR (bottom) images in the same patient show hyperintense enhancing lesions along the cerebral peduncles. AQP4 antibody was positive in this patient with NMOSD. Brain lesions in NMOSD typically involve the deep white matter, periependymal regions, corpus callosum, corticospinal tracts, brainstem, and cerebellum.*
 .](images/app.statdx.com_image_thumbnail_18a3a92e-8b6e-4557-9a3e-308224813fb7_annotated_true_size_900_quality_90_79e1db98_20251018T122510Z.jpg)
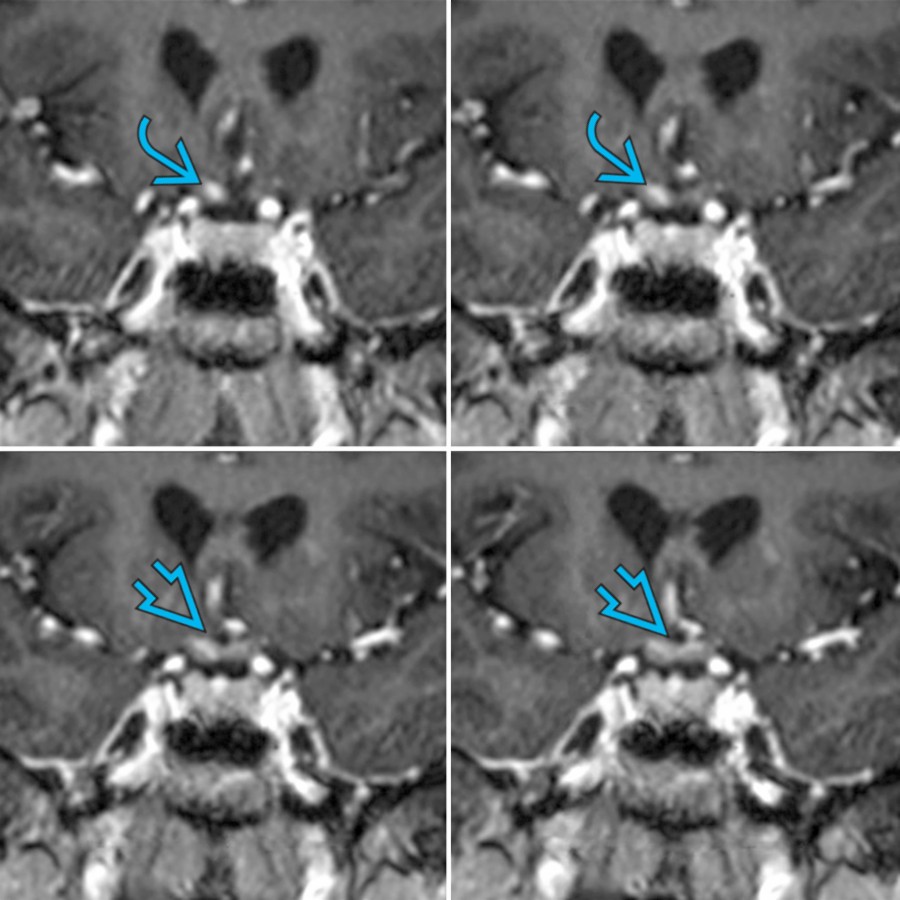
*Coronal T1 C+ MR images in a patient with AQP4 antibody (+) NMOSD show enhancement along the prechiasmatic right optic nerve and the optic chiasm .*

*Coronal T1 C+ MR images in a patient with AQP4 antibody (+) NMOSD show enhancement along the prechiasmatic right optic nerve and the optic chiasm .*
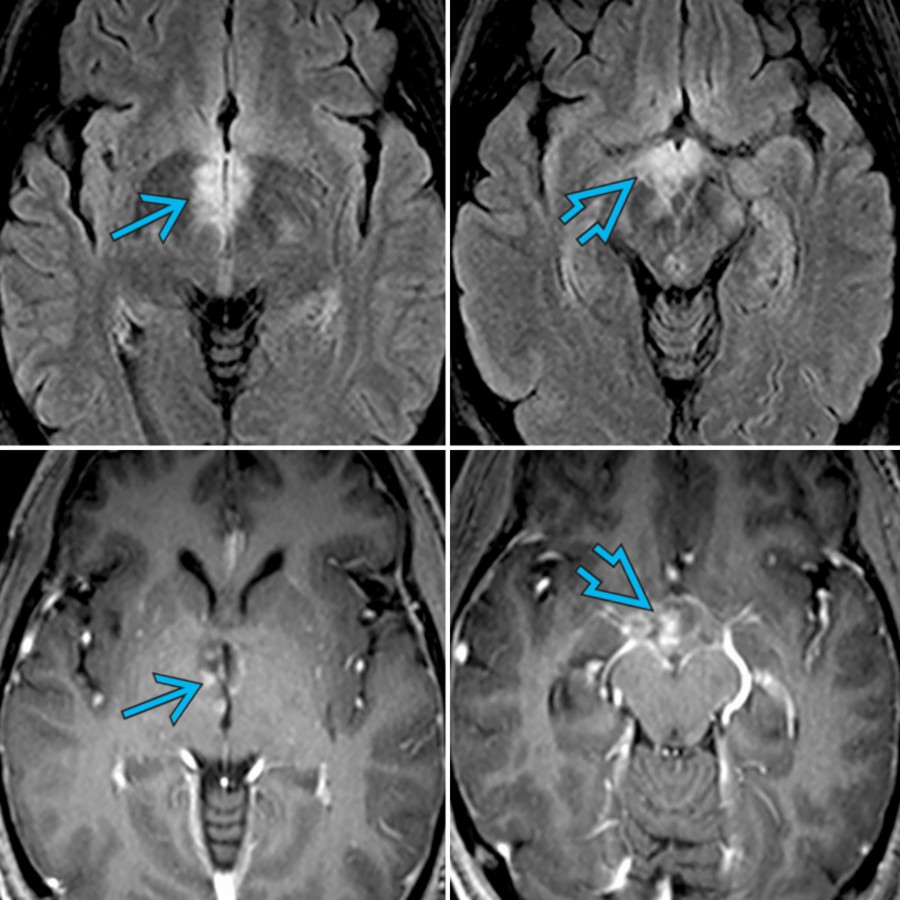
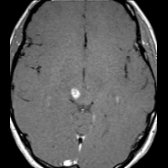
*Axial FLAIR MR (top) and T1 C+ MR (bottom) in the same patient show hyperintense lesions with patchy enhancement in the periependymal region surrounding the 3rd ventricle , and the hypothalamus . Brain lesions in NMOSD are typically localized in the periependymal regions where AQP4 is highly expressed.*
*Axial FLAIR MR (top) and T1 C+ MR (bottom) in the same patient show hyperintense lesions with patchy enhancement in the periependymal region surrounding the 3rd ventricle , and the hypothalamus . Brain lesions in NMOSD are typically localized in the periependymal regions where AQP4 is highly expressed.*
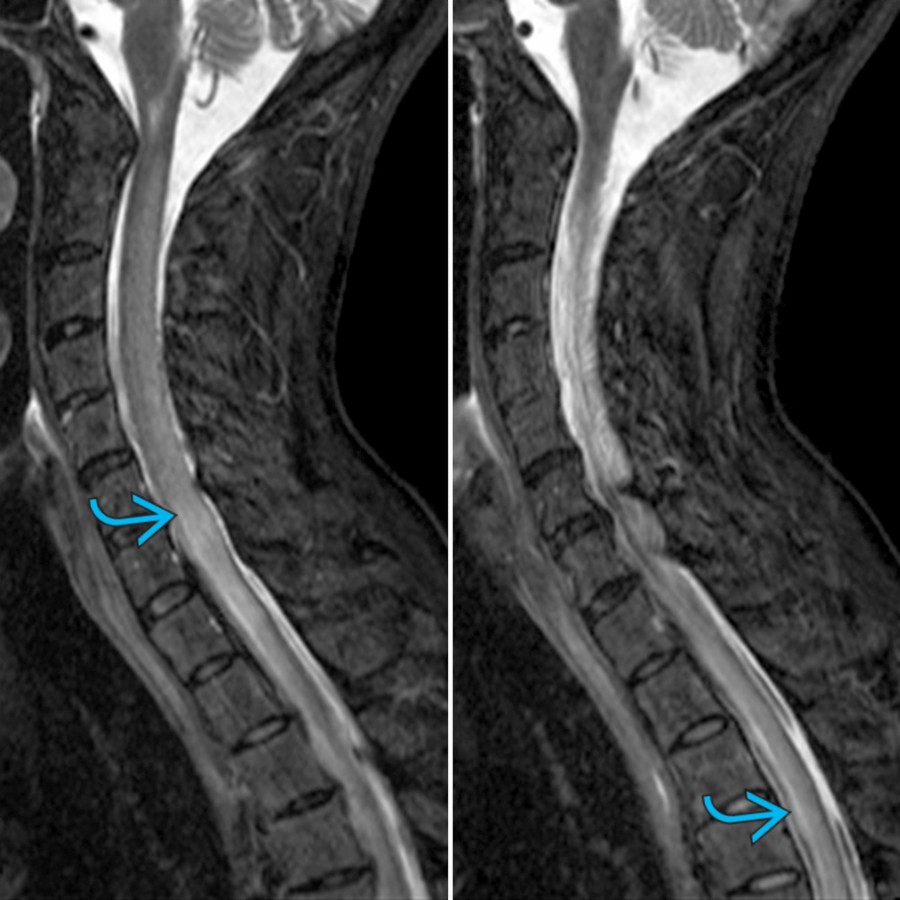
*Sagittal STIR MR in a patient presenting with myelopathy demonstrates a long segment of cord enlargement with hyperintensity .*
*Sagittal STIR MR in a patient presenting with myelopathy demonstrates a long segment of cord enlargement with hyperintensity .*

*Sagittal T1 C+ FS MR in the same patient demonstrates patchy enhancement in the cervical and upper thoracic cord. Cord lesions in NMOSD typically extend over 3 or more contiguous vertebral segments. There is involvement of the central gray matter or central and peripheral regions of the cord with > 50% cord area in the axial plane.*
*Sagittal T1 C+ FS MR in the same patient demonstrates patchy enhancement in the cervical and upper thoracic cord. Cord lesions in NMOSD typically extend over 3 or more contiguous vertebral segments. There is involvement of the central gray matter or central and peripheral regions of the cord with > 50% cord area in the axial plane.*
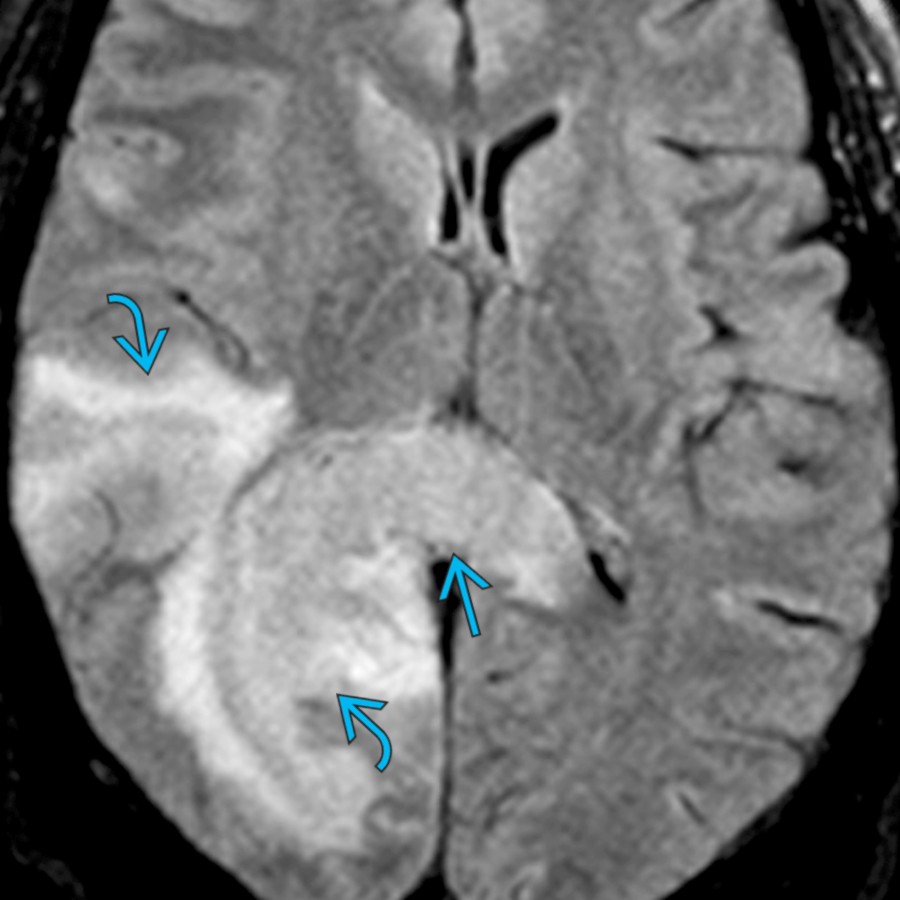
*Axial FLAIR MR in a patient with AQP4-IgG (+) NMOSD demonstrates large confluent lesions in the right temporal and occipital regions with involvement of the splenium of the corpus callosum.*
*Axial FLAIR MR in a patient with AQP4-IgG (+) NMOSD demonstrates large confluent lesions in the right temporal and occipital regions with involvement of the splenium of the corpus callosum.*
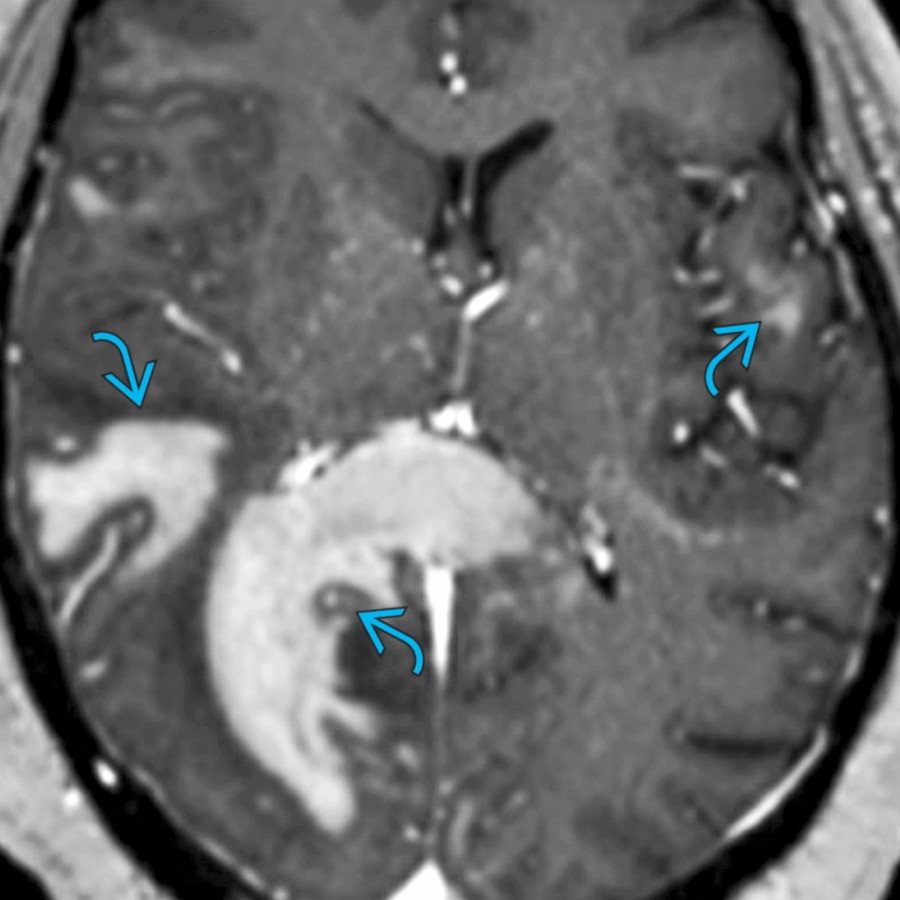
*Axial T1 C+ MR in the same patient shows large patchy areas of enhancement , often called "cloud-like" enhancement. This is one of the most common patterns of enhancement in NMOSD. Other patterns of enhancement include "pencil-thin" periependymal, nodular, and leptomeningeal.*
*Axial T1 C+ MR in the same patient shows large patchy areas of enhancement , often called "cloud-like" enhancement. This is one of the most common patterns of enhancement in NMOSD. Other patterns of enhancement include "pencil-thin" periependymal, nodular, and leptomeningeal.*

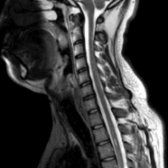
*Sagittal T2 MR (right) and T1 C+ MR (left) in a patient with NMOSD presenting with nausea and myelopathy demonstrate patchy enhancing lesion involving the dorsal medulla (area postrema region) and the upper cervical cord .*

*Sagittal T2 MR (right) and T1 C+ MR (left) in a patient with NMOSD presenting with nausea and myelopathy demonstrate patchy enhancing lesion involving the dorsal medulla (area postrema region) and the upper cervical cord .*
*Coronal T1 C+ MR images in a patient with AQP4 antibody (+) NMOSD show enhancement along the prechiasmatic right optic nerve and the optic chiasm .*

*Coronal T1 C+ MR images in a patient with AQP4 antibody (+) NMOSD show enhancement along the prechiasmatic right optic nerve and the optic chiasm .*

*Axial FLAIR MR (top) and T1 C+ MR (bottom) in the same patient show hyperintense lesions with patchy enhancement in the periependymal region surrounding the 3rd ventricle , and the hypothalamus . Brain lesions in NMOSD are typically localized in the periependymal regions where AQP4 is highly expressed.*

*Axial FLAIR MR (top) and T1 C+ MR (bottom) in the same patient show hyperintense lesions with patchy enhancement in the periependymal region surrounding the 3rd ventricle , and the hypothalamus . Brain lesions in NMOSD are typically localized in the periependymal regions where AQP4 is highly expressed.*

*Sagittal STIR MR in a patient presenting with myelopathy demonstrates a long segment of cord enlargement with hyperintensity .*

*Sagittal STIR MR in a patient presenting with myelopathy demonstrates a long segment of cord enlargement with hyperintensity .*

*Sagittal T1 C+ FS MR in the same patient demonstrates patchy enhancement in the cervical and upper thoracic cord. Cord lesions in NMOSD typically extend over 3 or more contiguous vertebral segments. There is involvement of the central gray matter or central and peripheral regions of the cord with > 50% cord area in the axial plane.*

*Sagittal T1 C+ FS MR in the same patient demonstrates patchy enhancement in the cervical and upper thoracic cord. Cord lesions in NMOSD typically extend over 3 or more contiguous vertebral segments. There is involvement of the central gray matter or central and peripheral regions of the cord with > 50% cord area in the axial plane.*

*Axial FLAIR MR in a patient with AQP4-IgG (+) NMOSD demonstrates large confluent lesions in the right temporal and occipital regions with involvement of the splenium of the corpus callosum.*

*Axial FLAIR MR in a patient with AQP4-IgG (+) NMOSD demonstrates large confluent lesions in the right temporal and occipital regions with involvement of the splenium of the corpus callosum.*

*Axial T1 C+ MR in the same patient shows large patchy areas of enhancement , often called "cloud-like" enhancement. This is one of the most common patterns of enhancement in NMOSD. Other patterns of enhancement include "pencil-thin" periependymal, nodular, and leptomeningeal.*

*Axial T1 C+ MR in the same patient shows large patchy areas of enhancement , often called "cloud-like" enhancement. This is one of the most common patterns of enhancement in NMOSD. Other patterns of enhancement include "pencil-thin" periependymal, nodular, and leptomeningeal.*

*Sagittal T2 MR (right) and T1 C+ MR (left) in a patient with NMOSD presenting with nausea and myelopathy demonstrate patchy enhancing lesion involving the dorsal medulla (area postrema region) and the upper cervical cord .*

*Sagittal T2 MR (right) and T1 C+ MR (left) in a patient with NMOSD presenting with nausea and myelopathy demonstrate patchy enhancing lesion involving the dorsal medulla (area postrema region) and the upper cervical cord .*
 enhancement. MOG was (+) and AQP4-IgG was (-).](images/app.statdx.com_image_thumbnail_5abd7f5f-c219-4988-be56-6ab012cbd08c_annotated_true_size_900_quality_90_4488b678_20251018T095345Z.jpg)
*Axial FLAIR (top) and T1 C+ MR (bottom) show patchy hyperintensity involving the cortex , cingulate gyrus, and corpus callosum with leptomeningeal and nodular enhancement. MOG was (+) and AQP4-IgG was (-).*
*Axial FLAIR (top) and T1 C+ MR (bottom) show patchy hyperintensity involving the cortex , cingulate gyrus, and corpus callosum with leptomeningeal and nodular enhancement. MOG was (+) and AQP4-IgG was (-).*
### Additional Images

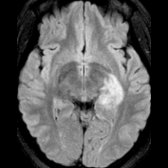
*Axial FLAIR MR in a patient with NMO demonstrates an ill-defined hyperintense lesion involving the right cerebral peduncle and midbrain .*
*Axial T1 C+ MR in the same patient shows a well-defined nodular area of enhancement in the region of FLAIR signal abnormality. Most reported NMO brain lesions do not show enhancement. The enhancement patterns reported include patchy enhancement with blurred margins ("cloud-like" enhancement), "pencil-thin" ependymal enhancement, and solid enhancement.*

*Axial FLAIR (top) and T1 C+ MR (bottom) show patchy hyperintensity involving the cortex , cingulate gyrus, and corpus callosum with leptomeningeal and nodular enhancement. MOG was (+) and AQP4-IgG was (-).*

*Axial FLAIR (top) and T1 C+ MR (bottom) show patchy hyperintensity involving the cortex , cingulate gyrus, and corpus callosum with leptomeningeal and nodular enhancement. MOG was (+) and AQP4-IgG was (-).*
### Additional Images

*Axial FLAIR MR in a patient with NMO demonstrates an ill-defined hyperintense lesion involving the right cerebral peduncle and midbrain .*

*Axial T1 C+ MR in the same patient shows a well-defined nodular area of enhancement in the region of FLAIR signal abnormality. Most reported NMO brain lesions do not show enhancement. The enhancement patterns reported include patchy enhancement with blurred margins ("cloud-like" enhancement), "pencil-thin" ependymal enhancement, and solid enhancement.*
 , consistent with acute optic neuritis.](images/app.statdx.com_image_thumbnail_0c76b02a-afd8-4735-91b3-86054aaebc0b_size_168_quality_85_48167667_20251018T095343Z.jpg)
*Axial T1WI C+ FS MR shows a markedly enhancing prechiasmatic right optic nerve and chiasm , consistent with acute optic neuritis.*

*Sagittal T2 DP FSE MR in the same patient shows a long segment of cord enlargement with hyperintensity. Ill-defined enhancement was also present in the cervical cord in this patient with myelopathy and vision loss. Patients with NMO have a worse prognosis with more severe disability than multiple sclerosis, despite lack of brain involvement.*
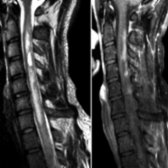
*Sagittal T2 (left) and T1WI C+ FS (right) images show multilevel T2 hyperintensity with irregular posterior enhancement in the cervical cord in a patient with a previous history of optic neuritis.*
*Sagittal T2WI MR in the same patient 1 year after treatment shows near-complete resolution of the T2 signal abnormality. Enhancement was no longer seen in the cervical cord. The cord lesions seen in NMO typically extend over 3 or more segments.*
*Axial FLAIR MR in a patient who presented with altered sensorium demonstrates a large hyperintense lesion in the left medial temporal lobe .*
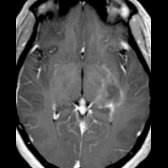
*Axial T1 C+ MR in the same patient shows patchy enhancement with blurred margins ("cloud-like" enhancement). NMO- IgG antibody in serum was positive in this patient. This pattern of enhancement has been reported as relatively specific for NMO.*
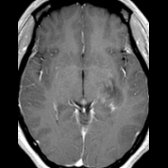
*Axial T1 C+ MR in the same patient 4 days after IV steroid therapy shows almost complete resolution of the enhancement .*
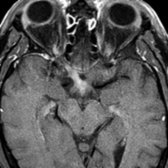
*Axial T1WI C+ FS MR shows a markedly enhancing prechiasmatic right optic nerve and chiasm , consistent with acute optic neuritis.*

*Sagittal T2 DP FSE MR in the same patient shows a long segment of cord enlargement with hyperintensity. Ill-defined enhancement was also present in the cervical cord in this patient with myelopathy and vision loss. Patients with NMO have a worse prognosis with more severe disability than multiple sclerosis, despite lack of brain involvement.*

*Sagittal T2 (left) and T1WI C+ FS (right) images show multilevel T2 hyperintensity with irregular posterior enhancement in the cervical cord in a patient with a previous history of optic neuritis.*

*Sagittal T2WI MR in the same patient 1 year after treatment shows near-complete resolution of the T2 signal abnormality. Enhancement was no longer seen in the cervical cord. The cord lesions seen in NMO typically extend over 3 or more segments.*

*Axial FLAIR MR in a patient who presented with altered sensorium demonstrates a large hyperintense lesion in the left medial temporal lobe .*

*Axial T1 C+ MR in the same patient shows patchy enhancement with blurred margins ("cloud-like" enhancement). NMO- IgG antibody in serum was positive in this patient. This pattern of enhancement has been reported as relatively specific for NMO.*

*Axial T1 C+ MR in the same patient 4 days after IV steroid therapy shows almost complete resolution of the enhancement .*
 in a unique "arch bridge" pattern.](images/app.statdx.com_image_thumbnail_edd8c34f-8077-4ed1-82a4-b1ecbfd4416e_size_168_quality_85_a2a9bd81_20251018T095342Z.jpg)
*Axial FLAIR MR in a patient with NMO shows multiple characteristic brain lesions. A large tumefactive lesion with ill-defined borders is seen in the left frontal lobe . An ill-defined hyperintense lesion is seen involving the posterior limb of right internal capsule , and there is involvement of the splenium of corpus callosum in a unique "arch bridge" pattern.*

*Axial FLAIR MR in a patient with NMOSD shows characteristic periependymal lesions surrounding the 3rd ventricle, involving the thalamus and hypothalamus .*
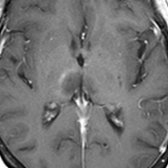
*Axial T1 C+ MR in the same patient shows subtle rim enhancement in the lesion in the right thalamus . Brain lesions in NMO/NMOSD are typically localized in the periependymal regions where AQP4 is highly expressed.*
in a unique "arch bridge" pattern.](images/app.statdx.com_image_thumbnail_edd8c34f-8077-4ed1-82a4-b1ecbfd4416e_size_168_quality_85_a2a9bd81_20251018T095342Z.jpg)
*Axial FLAIR MR in a patient with NMO shows multiple characteristic brain lesions. A large tumefactive lesion with ill-defined borders is seen in the left frontal lobe . An ill-defined hyperintense lesion is seen involving the posterior limb of right internal capsule , and there is involvement of the splenium of corpus callosum in a unique "arch bridge" pattern.*

*Axial FLAIR MR in a patient with NMOSD shows characteristic periependymal lesions surrounding the 3rd ventricle, involving the thalamus and hypothalamus .*

*Axial T1 C+ MR in the same patient shows subtle rim enhancement in the lesion in the right thalamus . Brain lesions in NMO/NMOSD are typically localized in the periependymal regions where AQP4 is highly expressed.*