---
title: "Pheochromocytoma"
docid: "1bfc887d-4686-445b-a0d2-f3b380a0da3a"
authors:
- key: "7e25292c-4d6a-4f35-98b2-1877e5989352"
value: "Ashish P. Wasnik, MD, FSAR"
breadcrumbs:
-
name: "Ultrasound"
slug: "ultrasound"
treeNodeId: "e7cdfeb1-bb55-4cca-9854-46cadee515d2"
-
name: "Diagnosis"
slug: "diagnosis"
treeNodeId: "594506fe-1241-4d01-9b37-a9d64f0c98c4"
-
name: "Adrenal Gland"
slug: "adrenal-gland"
treeNodeId: "bdbaa036-5505-43ee-94e1-5a2ece43da0f"
-
name: "Pheochromocytoma"
slug: "pheochromocytoma"
treeNodeId: null
category: "Ultrasound"
cmeTopicId: "294ea24b-7fbc-4cf4-89d4-e53caacbe2e6"
documentVersionId: "84b213c9-8864-4424-b1e5-b6a46d8489bc"
imageCount: 16
lastUpdated: "07/01/21"
pageDescription: "Pheochromocytoma"
pageKeywords: "Ultrasound, Diagnosis, Adrenal Gland, Pheochromocytoma"
pageTitle: "Pheochromocytoma | STATdx"
enhancedTitle: "Pheochromocytoma"
type: "DX"
references: true
breadcrumbs:
- "Ultrasound"
- "Diagnosis"
- "Adrenal Gland"
- "Pheochromocytoma"
---
# KEY FACTS
- ## Terminology
- Rare catecholamine-secreting tumor arising from chromaffin cells of adrenal medulla
- Termed **paraganglioma** if extraadrenal
- ## Imaging
- Best diagnostic clue
- Adrenal mass in setting of clinical symptoms or biochemical abnormality
- Paroxysmal headache, palpitations, sweating
- ↑ levels of 24-hour urine-fractionated metanephrines
- "**Imaging chameleon**": Variable US/CT/MR appearance; mimics other lesions
- Commonly solid and hypervascular ± cystic change, necrosis, and calcification
- Can be purely cystic
- **1st line**: CT or MR
- **US**: Comparable to CT in detecting adrenal tumors; limited for extraadrenal disease
- **I-123 MIBG**: For extraadrenal, metastatic, or recurrent disease
- ## Top Differential Diagnoses
- Adrenal adenoma
- Adrenal metastases or lymphoma
- Adrenocortical carcinoma
- Adrenal neuroblastoma
- Adrenal granulomatous infection
- ## Diagnostic Checklist
- Remembered as "**r****ule of 10s**"
- 10% extraadrenal (paraganglioma)
- 10% bilateral (suggest hereditary disease)
- 10% pediatric (suggest hereditary disease)
- 10% contain calcification
- 10% malignant (↑ extraadrenal cases)
- 25% familial (previously thought to be 10%)
# TERMINOLOGY
- ## Definitions
- Paraganglioma: Neuroendocrine tumor arising from paraganglia anywhere in sympathetic chain
- Pheochromocytoma: Adrenal medullary paraganglioma arising from catecholamine-secreting chromaffin cells of adrenal medulla
# IMAGING
- ## General Features
- ### Best diagnostic clue
- Adrenal mass in setting of clinical symptoms or biochemical abnormality
- ### Location
- Paragangliomas can occur along sympathetic chain from neck to urinary bladder
- Majority are subdiaphragmatic (98%)
- Adrenal (90%)
- Extraadrenal (10%)
- Organ of Zuckerkandl, 2.5% [from superior mesenteric artery (SMA) to aortic bifurcation, mostly around inferior mesenteric artery]
- Urinary bladder sympathetic chain, 1%
- Typically unilateral
- Bilateral: Commonly with hereditary conditions
- ### Size
- Variable: Typically 3-5 cm (can be up to 15 cm)
- ### Morphology
- Well-circumscribed, encapsulated tumor
- Variable size and appearance on morphology and imaging renders name "chameleon tumors"
- Commonly solid and hypervascular ± cystic change, necrosis, and calcification
- Can be purely cystic
- Pheochromocytomas and paragangliomas demonstrate similar imaging features but vary in location
- ## Ultrasonographic Findings
- ### Grayscale ultrasound
- Variable appearance: Solid (75%) > solid/cystic or cystic
- Iso-/hypoechoic (75%) or hyperechoic (25%) to renal cortex
- Small tumors: Solid, well-circumscribed; uniform echoes → can be poorly delineated due to obscuration from overlying bowel gas
- Large tumors: Solid, heterogeneous, or homogeneous echotexture
- Heterogeneity due to necrosis (hypoechoic) and hemorrhage (hyperechoic)
- Can be predominantly cystic due to chronic hemorrhage and necrotic debris (fluid-fluid level)
- Always evaluate bladder wall, renal hilum, and organ of Zuckerkandl at origin of inferior mesenteric artery (CT more sensitive)
- ### Color Doppler
- Hypervascular ± heterogeneous
- Compression/invasion of inferior vena cava (IVC)/renal vein
- Seen with both benign and malignant tumors
- ## CT Findings
- **NECT**: Well-defined mass with low soft tissue attenuation
- Generally attenuation > 10 HU; however, rarely intracellular fat may result in lower attenuation → posing challenge to differentiate from adenoma
- ± ↑ density (hemorrhage), ↓ density (cystic degeneration; necrosis), calcification (rare; 10%)
- **CECT**: Marked enhancement; may be heterogeneous due to hemorrhage/necrosis
- Variable washout characteristics: Can show rapid washout that mimics adenoma
- No convincing evidence that IV injection of iodinated contrast precipitates hypertensive crisis
- ## MR Findings
- **T1WI**: **Isointense** to muscle and hypointense to liver
- Variable signal intensity if necrosis/hemorrhage present
- Rarely, contain microscopic fat on chemical shift imaging, mimicking adenoma
- **T2WI**: T2 hyperintense due to ↑ water content (cystic/liquefactive necrosis)
- Classic light bulb appearance of marked T2-bright signal intensity (SI), variably (present in up to 2/3)
- 35% have low T2 SI (isointense to spleen)
- Most common: Heterogeneously enhancing lesion with multiple high-SI pockets
- **T1WI C+**: Characteristic **salt and pepper** pattern
- **Salt** (enhancing parenchyma); **pepper** (↑ vascular flow voids due to hypervascular tumor)
- ## Nuclear Medicine Findings
- **1st line**: I-123 metaiodobenzylguanidine (**MIBG**)
- Norepinephrine analog
- After 24-72 hours: ↑ uptake of I-123 MIBG in tumor
- Useful for extraadrenal, metastatic, recurrent disease
- Sensitivity (77-90%); specificity (95-100%)
- 2nd line: 111In-pentetreotide FDG PET
- F-18 fluorodopamine, F-18 dihydroxyphenylalanine (DOPA) analogs
- ## Imaging Recommendations
- ### Best imaging tool
- **NE + CECT**: Overall 93-100% sensitive; however, up to 40% of extraadrenal lesions may be missed on CT
- **I-123 MIBG**: Superior detection of extraadrenal, metastatic, &/or recurrent disease
- US limited for smaller adrenal tumors; poor sensitivity for extraadrenal lesions
- ### Protocol advice
- Include aortic bifurcation in CT/MR FOV to evaluate for paragangliomas (along sympathetic chain)
# DIFFERENTIAL DIAGNOSIS
- [Adrenal Adenoma](/document/adrenal-adenoma/25bd0538-d37f-4bd1-9eb3-094d625723a5)
- Most common benign adrenal lesion
- Pheochromocytomas tend to be larger than adenomas
- Cystic and rare microscopic fat-containing pheochromocytomas may also be hypodense on NECT
- Adenoma: Characteristic CT washout and MR signal dropout (majority)
- ## Adrenal Metastases
- Most common malignant adrenal neoplasm (up to 25%)
- Typically bilateral; delayed contrast washout
- [Adrenal Lymphoma](/document/adrenal-lymphoma/44639c90-bd04-4e2a-a470-2c28a0e2ff78)
- Large infiltrative, bilateral masses; maintain adrenal contour
- 25% secondary to non-Hodgkin lymphoma; primary is rare
- ## Adrenocortical Carcinoma
- Rare; aggressive; large, unilateral, heterogeneous solid mass with necrosis; hemorrhage ± calcification
- T2 hyperintense and T1 hypointense to liver (as with "classic" pheochromocytomas)
- Aggressive, often with IVC extension
- ## Adrenal Neuroblastoma
- Large pediatric adrenal mass; calcification (80-90%)
- ## Adrenal Granulomatous Infection
- TB, histoplasmosis, other fungal diseases; usually bilateral
- Acute (hypoechoic masses) or chronic (small and calcified)
# PATHOLOGY
- ## General Features
- ### Associated abnormalities
- Majority are sporadic
- 25% have autosomal dominant gene mutation
- **Multiple endocrine neoplasia type 2 (MEN2)**
- *MEN2*mutation; 50% have pheochromocytoma
- Medullary thyroid carcinoma, hyperparathyroidism, neuromas, and marfanoid habitus
- **von Hippel-Lindau (VHL) disease**
- *VHL*tumor suppressor gene; 10-25% risk
- Multiple benign and malignant tumors
- **Neurofibromatosis type 1**
- Rare cause of pheochromocytomas; 1% risk
- Cutaneous/plexiform neurofibromas, optic nerve gliomas, peripheral nerve sheath tumors, gastrointestinal stromal tumors
- **Pheochromocytoma-paraganglioma syndromes**
- Mutations of succinate dehydrogenase gene family; 50% risk
- ↑ incidence of extraadrenal tumors and head/neck paragangliomas
- Most are benign; 10% are malignant
- Diagnosis of malignancy is based solely on presence of direct local tumor invasion or metastatic disease
- Extraadrenal paragangliomas are more likely to be malignant
- ## Gross Pathologic & Surgical Features
- Small tumor: Well-circumscribed, yellow-tan lesion confined to adrenals
- Large tumor: Hemorrhagic, cystic/necrotic masses
- ## Microscopic Features
- Predominantly chromaffin cells; occasionally spindle cells are dominant feature
- Term pheochromocytoma refers to dusky color of cells stained with chromium salts
- No single histologic feature of pheochromocytoma consistently predicts malignancy
- Definitive pathologic diagnosis of malignancy is based on presence of metastatic disease
# CLINICAL ISSUES
- ## Presentation
- ### Most common signs/symptoms
- Majority are asymptomatic; symptoms may be episodic or paroxysmal
- Classic triad (arises from adrenergic excess)
- Paroxysmal headache, palpitations, sweating
- 90% specific but uncommon (only present in 10.0-36.5% of patients)
- ### Other signs/symptoms
- Hypertensive crisis: Palpitations, tremors, arrhythmias, pain, myocardial infarction
- Laboratory data
- Tumors typically secrete norepinephrine > epinephrine
- **↑**levels of 24-hour urine-fractionated metanephrines
- 90-97% sensitivity; 69-98% specificity
- ## Demographics
- ### Age
- Sporadic cases, 3rd and 4th decades
- Hereditary cases, 3rd decade
- 10% are found in children
- ### Sex
- Slight female predilection (M:F = 1:1.4)
- ### Epidemiology
- Exact incidence: Unknown
- Prevalence in hypertensive adults 0.1-0.6%
- Majority of pheochromocytomas are likely asymptomatic (incidentalomas)
- ## Natural History & Prognosis
- Hypertensive crises and cardiovascular complications ↑ morbidity/mortality
- Prognosis: Noninvasive and nonmetastatic: Typically favorable
- ## Treatment
- Symptomatic therapy: α-adrenergic blockade and calcium channel antagonists
- Laparoscopic resection/debulking for both benign and malignant tumors
- Adjuvant therapy (malignant tumors): I-131 MIBG therapy ± chemotherapy (cyclophosphamide, vincristine, dacarbazine)
# DIAGNOSTIC CHECKLIST
- ## Consider
- Imaging can mimic other diagnoses; labs essential for diagnosis
- ## Image Interpretation Pearls
- Extraadrenal tumors arise anywhere along sympathetic ganglia (neck to bladder), attention to these locations
c0256142-d2c8-452c-ad4f-032d36d44ba0
## References
# Selected References
1. [Nandra G et al: Technical and interpretive pitfalls in adrenal imaging. Radiographics. 40(4):1041-60, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=32609593%5Bpmid%5D)
1. [Chang CA et al: (68)Ga-DOTATATE and (18)F-FDG PET/CT in paraganglioma and pheochromocytoma: utility, patterns and heterogeneity. Cancer Imaging. 16(1):22, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27535829%5Bpmid%5D)
1. [Lattin GE Jr et al: From the radiologic pathology archives: adrenal tumors and tumor-like conditions in the adult: radiologic-pathologic correlation. Radiographics. 34(3):805-29, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24819798%5Bpmid%5D)
1. [Leung K et al: Pheochromocytoma: the range of appearances on ultrasound, CT, MRI, and functional imaging. AJR Am J Roentgenol. 200(2):370-8, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=23345359%5Bpmid%5D)
1. [Raja A et al: Multimodality imaging findings of pheochromocytoma with associated clinical and biochemical features in 53 patients with histologically confirmed tumors. AJR Am J Roentgenol. 201(4):825-33, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=24059371%5Bpmid%5D)
1. [Parenti G et al: Updated and new perspectives on diagnosis, prognosis, and therapy of malignant pheochromocytoma/paraganglioma. J Oncol. 2012:872713, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22851969%5Bpmid%5D)
1. [Blake MA et al: Pheochromocytoma: an imaging chameleon. Radiographics. 24 Suppl 1:S87-99, 2004](http://www.ncbi.nlm.nih.gov/pubmed/?term=15486252%5Bpmid%5D)
## Images
### Selected Images
 , moderate in size with a well-circumscribed margin and solid appearance. Note hypervascularity
, moderate in size with a well-circumscribed margin and solid appearance. Note hypervascularity  of the mass, which commonly results in necrosis and cystic change.](images/app.statdx.com_image_thumbnail_1a98e200-6f6a-4fb6-888d-6da42b0c490b_annotated_true_size_900_quality_90_4c277881ccda491f9a0e10e657c401bd902d1b73.jpg)
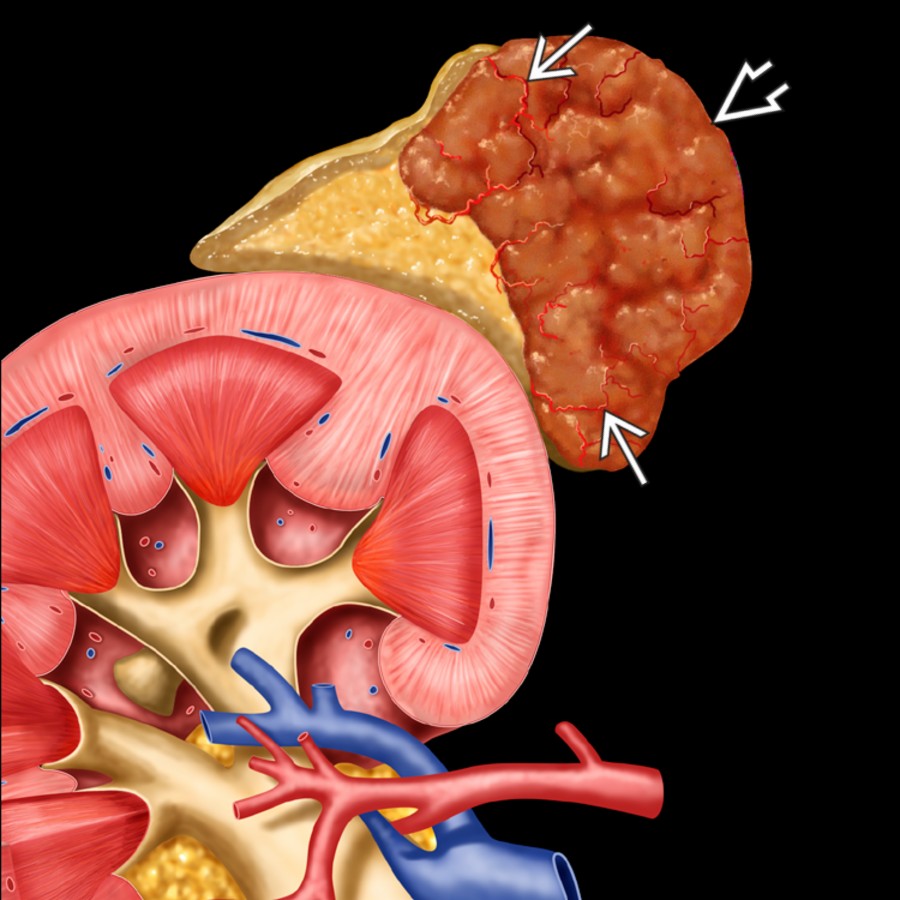
*Graphic shows a typical pheochromocytoma , moderate in size with a well-circumscribed margin and solid appearance. Note hypervascularity of the mass, which commonly results in necrosis and cystic change.*

*Graphic shows a typical pheochromocytoma , moderate in size with a well-circumscribed margin and solid appearance. Note hypervascularity of the mass, which commonly results in necrosis and cystic change.*
*Graphic shows a typical pheochromocytoma , moderate in size with a well-circumscribed margin and solid appearance. Note hypervascularity of the mass, which commonly results in necrosis and cystic change.*

*Graphic shows a typical pheochromocytoma , moderate in size with a well-circumscribed margin and solid appearance. Note hypervascularity of the mass, which commonly results in necrosis and cystic change.*
 , proven to be a pheochromocytoma.](images/app.statdx.com_image_thumbnail_49dae42d-f58a-4b44-895e-afa709899446_annotated_true_size_900_quality_90_5631abd56094d59dcb19b3758f8159fde1d675f1.jpg)
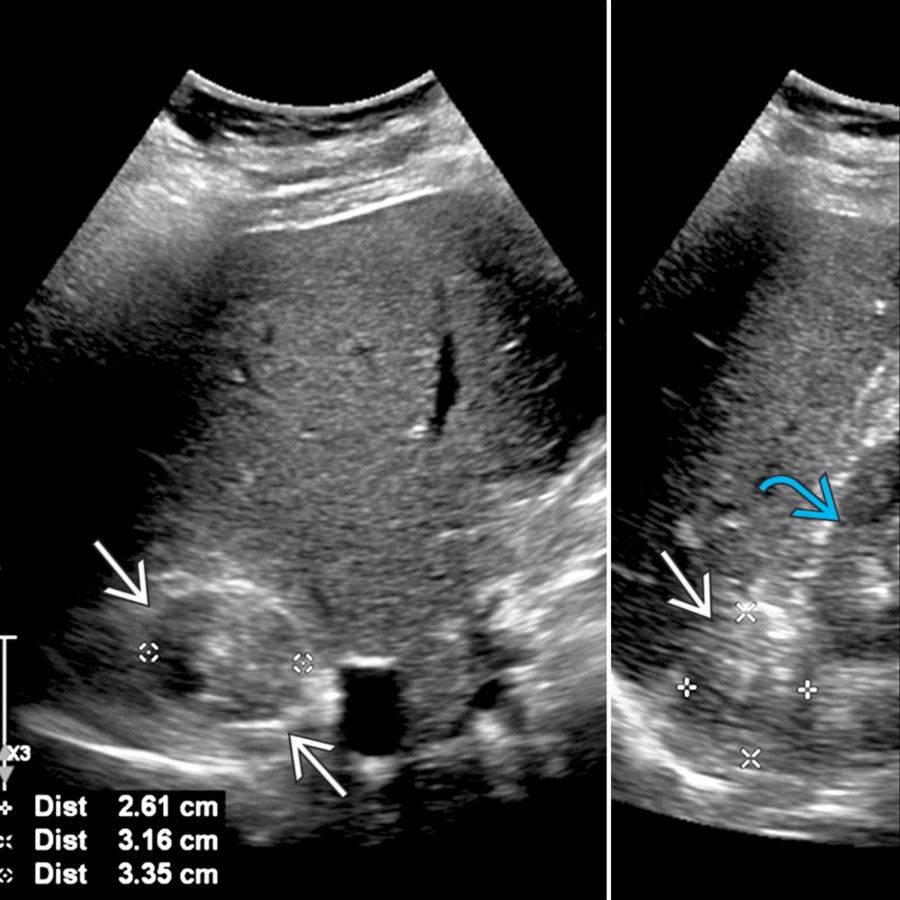
*Transverse (left) and longitudinal (right) transabdominal ultrasound show a well-demarcated, heterogenous, solid right adrenal mass hyperechoic to the renal cortex , proven to be a pheochromocytoma.*
*Transverse (left) and longitudinal (right) transabdominal ultrasound show a well-demarcated, heterogenous, solid right adrenal mass hyperechoic to the renal cortex , proven to be a pheochromocytoma.*
 in the right suprarenal region medially, proven to be a paraganglioma.](images/app.statdx.com_image_thumbnail_0319f064-3c59-42e3-9b35-56d895048d9b_annotated_true_size_900_quality_90_9a98eb818bac8c87fdf4bd942b07b110d34ece4f.jpg)
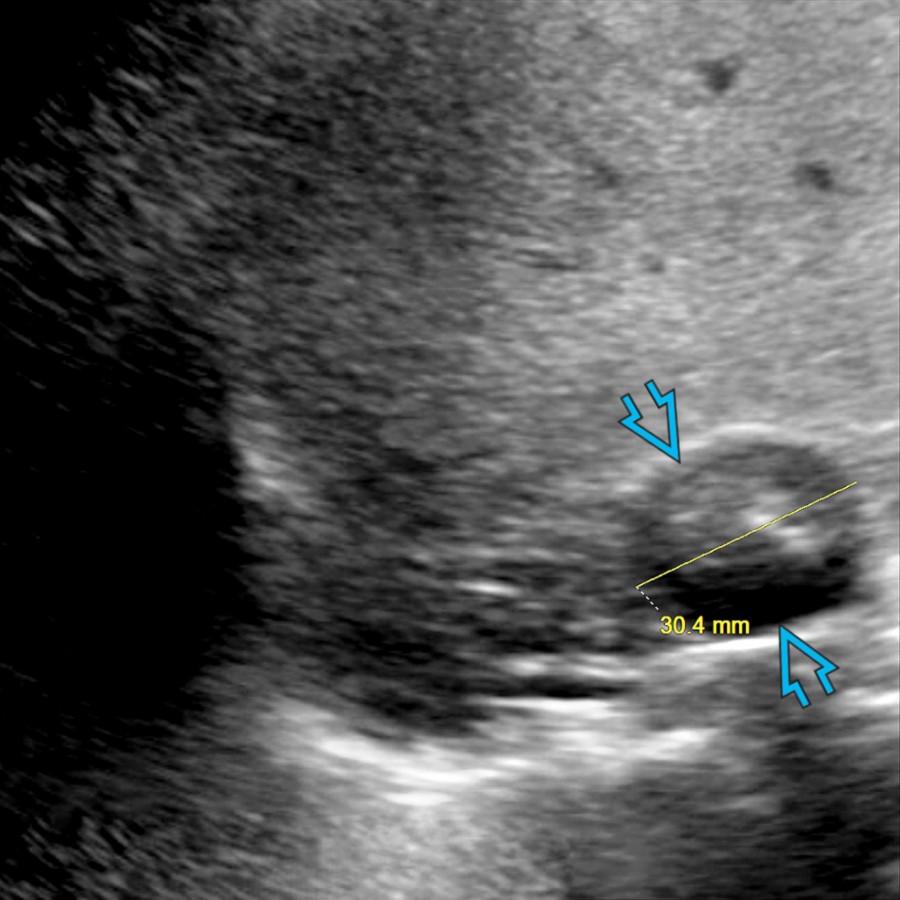
*Longitudinal transabdominal ultrasound demonstrates well-circumscribed, round, heterogeneous, hypoechoic mass in the right suprarenal region medially, proven to be a paraganglioma.*
*Longitudinal transabdominal ultrasound demonstrates well-circumscribed, round, heterogeneous, hypoechoic mass in the right suprarenal region medially, proven to be a paraganglioma.*
 , proven to be a paraganglioma.](images/app.statdx.com_image_thumbnail_320a766e-0e57-4194-88b2-d3fbb58bcea8_annotated_true_size_900_quality_90_299fbc8b184de3906e0d903ade2b46dcffda67db.jpg)
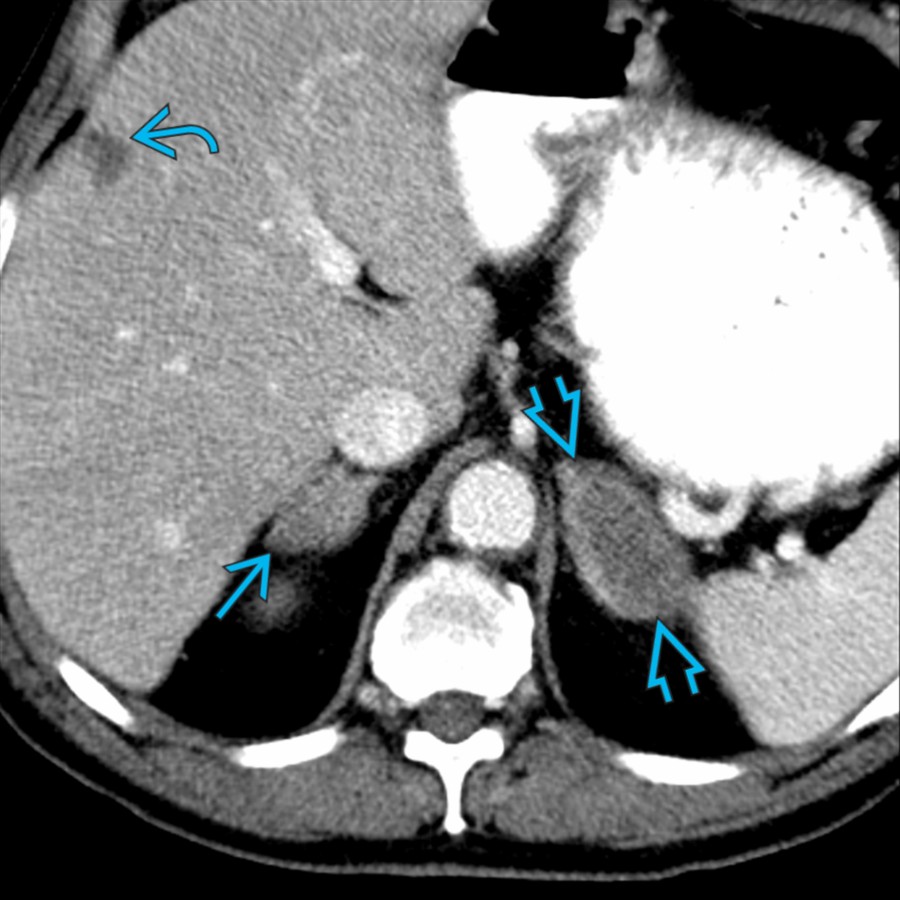
*Axial CECT in the previous patient shows a well-circumscribed, round, heterogeneous, hypodense mass , anteromedial to the upper pole right kidney , proven to be a paraganglioma.*

*Axial CECT in the previous patient shows a well-circumscribed, round, heterogeneous, hypodense mass , anteromedial to the upper pole right kidney , proven to be a paraganglioma.*
 .](images/app.statdx.com_image_thumbnail_126ce433-ace3-4fe1-b768-68d82c6ae5fb_annotated_true_size_900_quality_90_415965939753a72d160a59ebddedff54047b9f27.jpg)
*Longitudinal transabdominal ultrasound shows a large left adrenal mass , slightly heterogeneous and hypoechoic to the renal cortex .*
*Axial CECT in the same patient confirms the left adrenal mass , along with right adrenal mass and a liver lesion , confirmed lung cancer metastases.*

*Axial T2WI MR shows 2 well-circumscribed, paraaortic paragangliomas .*

*Corresponding axial T1WI C+ FS MR demonstrates the same paragangliomas . Notice the salt and pepper appearance of the right-most paragangliomas, consisting of enhancing parenchyma and internal flow void (hypervascularity).*
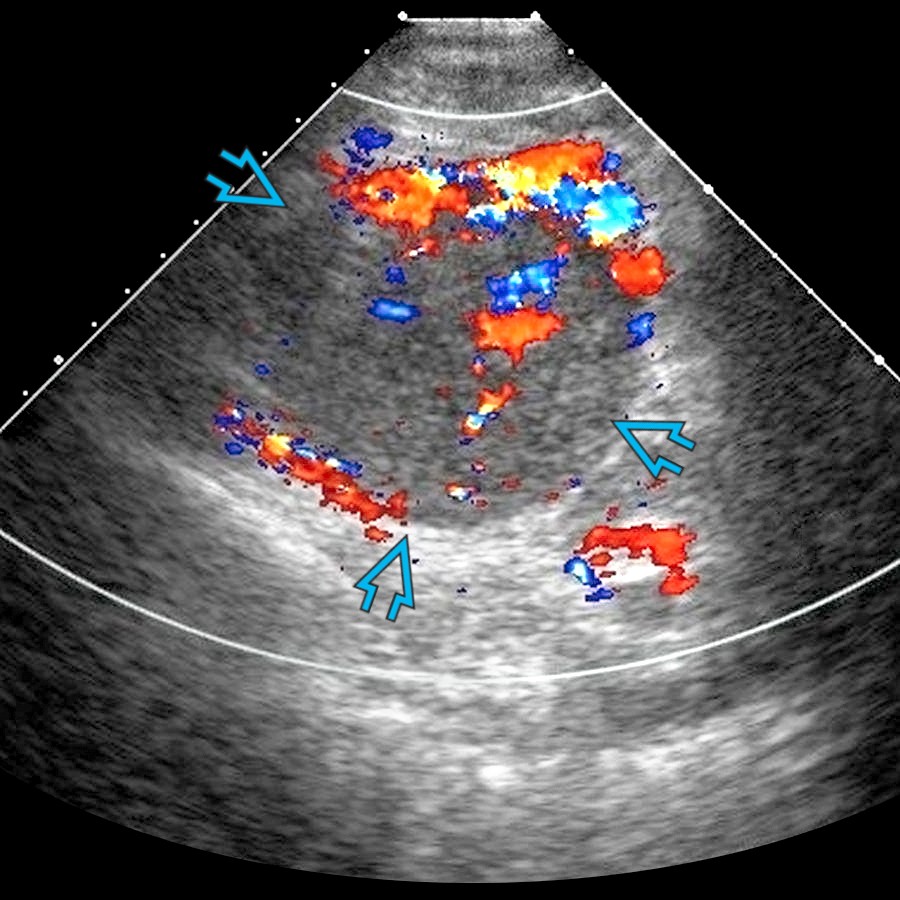
*Transverse transabdominal color Doppler ultrasound shows heterogenous, hypervascular mass anteromedial to the left kidney, confirmed paraganglioma.*

*Axial arterial-phase CECT in the same patient confirms a large heterogeneously enhancing mass in the left retroperitoneum , confirmed paraganglioma.*
### Additional Images

*Transverse transabdominal color Doppler ultrasound of a right adrenal pheochromocytoma shows a well-defined, heterogenous mass .*

*Coronal CECT shows a large, well-defined mass with avidly enhancing solid portions and large, hypodense areas of necrosis , confirmed paraganglioma.*

*Axial fused PET/CT demonstrates ↑ radiotracer uptake within the solid portions of the paraganglioma, whereas the necrotic areas appear photopenic . The mass is distinct from the left kidney , but notice abutment/narrowing of the main left renal vein .*

*Transverse color Doppler ultrasound shows a right adrenal pheochromocytoma displacing and compressing the inferior vena cava .*

*Axial CECT shows a large, well-circumscribed, moderately enhancing right adrenal pheochromocytoma with hypodense area of necrosis .*

*DTPA-MIBG scan of the same patient shows uptake within the pheochromocytoma . Note DTPA uptake in kidneys . MIBG is useful to detect extraadrenal tumors.*
.](images/app.statdx.com_image_thumbnail_126ce433-ace3-4fe1-b768-68d82c6ae5fb_annotated_true_size_900_quality_90_415965939753a72d160a59ebddedff54047b9f27.jpg)
*Longitudinal transabdominal ultrasound shows a large left adrenal mass , slightly heterogeneous and hypoechoic to the renal cortex .*

*Axial CECT in the same patient confirms the left adrenal mass , along with right adrenal mass and a liver lesion , confirmed lung cancer metastases.*

*Axial T2WI MR shows 2 well-circumscribed, paraaortic paragangliomas .*

*Corresponding axial T1WI C+ FS MR demonstrates the same paragangliomas . Notice the salt and pepper appearance of the right-most paragangliomas, consisting of enhancing parenchyma and internal flow void (hypervascularity).*

*Transverse transabdominal color Doppler ultrasound shows heterogenous, hypervascular mass anteromedial to the left kidney, confirmed paraganglioma.*

*Axial arterial-phase CECT in the same patient confirms a large heterogeneously enhancing mass in the left retroperitoneum , confirmed paraganglioma.*
### Additional Images

*Transverse transabdominal color Doppler ultrasound of a right adrenal pheochromocytoma shows a well-defined, heterogenous mass .*

*Coronal CECT shows a large, well-defined mass with avidly enhancing solid portions and large, hypodense areas of necrosis , confirmed paraganglioma.*

*Axial fused PET/CT demonstrates ↑ radiotracer uptake within the solid portions of the paraganglioma, whereas the necrotic areas appear photopenic . The mass is distinct from the left kidney , but notice abutment/narrowing of the main left renal vein .*

*Transverse color Doppler ultrasound shows a right adrenal pheochromocytoma displacing and compressing the inferior vena cava .*

*Axial CECT shows a large, well-circumscribed, moderately enhancing right adrenal pheochromocytoma with hypodense area of necrosis .*

*DTPA-MIBG scan of the same patient shows uptake within the pheochromocytoma . Note DTPA uptake in kidneys . MIBG is useful to detect extraadrenal tumors.*