---
title: "Posterior Fossa Neoplasm, Adult"
docid: "9d6bcceb-36a2-4f49-a5b2-1dd076541be8"
authors:
- key: "26ebc2e8-e4f7-40ee-8f5c-d23fe383e15c"
value: "Yoshimi Anzai, MD, MPH"
- key: "5cff4116-3654-4b3a-bb75-5ebe0b8c9850"
value: "Anne G. Osborn, MD, FACR"
breadcrumbs:
-
name: "Head and Neck"
slug: "head-and-neck"
treeNodeId: "ed24ed8c-5d57-4629-879b-447b82d2973d"
-
name: "Differential Diagnosis"
slug: "differential-diagnosis"
treeNodeId: "40d68862-8975-4dde-ac2b-ebc43ab0fb5c"
-
name: "CPA-IAC and Posterior Fossa"
slug: "cpa-iac-and-posterior-fossa"
treeNodeId: "c590eedb-4a3b-4158-a04f-ad880564c992"
-
name: "Anatomically Based Differentials"
slug: "anatomically-based-differentials"
treeNodeId: "debfb06c-8656-4f5d-92c1-eaa468185d78"
-
name: "Posterior Fossa Neoplasm, Adult"
slug: "posterior-fossa-neoplasm-adult"
treeNodeId: null
category: "Head and Neck"
documentVersionId: "8071b0df-9c2d-4d93-8775-a2b6a68bf9c8"
imageCount: 22
lastUpdated: "08/06/18"
pageDescription: "Posterior Fossa Neoplasm, Adult"
pageKeywords: "Head and Neck, Differential Diagnosis, CPA-IAC and Posterior Fossa, Anatomically Based Differentials, Posterior Fossa Neoplasm, Adult"
pageTitle: "Posterior Fossa Neoplasm, Adult | STATdx"
enhancedTitle: "Posterior Fossa Neoplasm, Adult"
type: "DDX"
references: true
breadcrumbs:
- "Head and Neck"
- "Differential Diagnosis"
- "CPA-IAC and Posterior Fossa"
- "Anatomically Based Differentials"
- "Posterior Fossa Neoplasm, Adult"
---
# ESSENTIAL INFORMATION
- ## Key Differential Diagnosis Issues
- With exception of vestibular schwannoma, posterior fossa (PF) neoplasms rare in adults
- Most important question: Is lesion intra- or extraaxial
- **Extraaxial PF lesions**
- Most adult PF neoplasms are extraaxial
- By far, most common is **vestibular schwannoma**
- Meningioma > metastasis > other schwannomas > glomus jugulare paraganglioma
- **Intraaxial: Parenchymal or intraventricular**
- Adult parenchymal neoplasms all uncommon/rare
- Overall, most common by far is metastasis
- Hemangioblastoma most common primary
- Glioblastoma, astrocytomas, most common adult supratentorial tumors are rare in PF
- 4th ventricle
- Subependymoma > ependymoma > choroid plexus papilloma
- Number 1 site for ependymoma & subependymoma
- Ependymoma (usually in children) often extends into foramen of Luschka &/or Magendie
- Choroid plexus papilloma in body/lateral recess, cerebellopontine angle (CPA)
- ## Helpful Clues for Common Diagnoses
- **Vestibular Schwannoma**
- By far most common adult PF neoplasm
- All others less common or rare
- 90% of all CPA-IAC masses
- Imaging findings
- Looks like "ice cream on cone" (CPA-IAC)
- Enhances strongly
- ± intra- or extratumoral cysts
- Preserved fluid at IAC fundus is predictive of improved hearing preservation after resection
- ## Helpful Clues for Less Common Diagnoses
- **Meningioma****in****Cerebellopontine Angle**
- Imaging findings
- Mushroom-shaped mass caps IAC
- Flat base towards dural surface
- ± hyperostosis, dural tail sign
- 25% show IAC involvement
- **Metastases****in****Cerebellopontine Angle**
- CPA metastases can arise in 4 locations
- Dura-arachnoid
- Cranial nerves (VII, VIII most common)
- Flocculusmimi
- Choroid plexus (foramen of Luschka)
- Imaging findings
- Irregular, invasive margins
- Solid, enhancing tumor on dura, cranial nerve surfaces, in flocculus or choroid plexus
- **Metastasi****s****in Brainstem or Cerebellum**
- 2nd most common adult PF neoplasm
- Most common adult parenchymal PF tumor
- Rarely may be only brain metastasis
- Enhancing solid or cystic mass with adjacent brain edema
- **Hemangioblastoma**
- 95% are located in PF
- Hemispheres > > vermis > brainstem, 4th ventricle
- < 50% of patients have von Hippel-Lindau syndrome
- Look for multiple lesions: Spinal mass, visceral cysts
- Imaging findings
- 60% nonenhancing cyst with avidly enhancing mural nodule
- Large drainage vein, ± blood products
- **Other Schwannomas**
- **Trigeminal (CNV)****S****chwannoma**
- Upper CPA mass
- Look for dumbbell shape (CPA + Meckel cave components)
- **Facial****N****erve (CNVII) Schwannoma**
- CPA-IAC mass with labyrinthine tail
- Look for CNVII labyrinthine segment tumor
- If labyrinthine tail absent, mimics vestibular schwannoma
- **Jugular Foramen****Schwannoma**
- Enhancing mass arising from jugular foramen
- Smooth remodeling of bony margins
- Projects cephalad into CPA cistern
- **Hypoglossal (CNXII) Schwannoma**
- Enhancing mass
- Smooth remodeling or widening of hypoglossal canal
- Look for ipsilateral tongue atrophy
- **Subependymoma**
- Middle-aged/elderly adult; asymptomatic most often
- Imaging: T2 hyperintense lobulated intraventricular mass
- 4th ventricle (60%) > other locations
- ± cysts, calcifications, rare intramural hemorrhage
- **Choroid Plexus Papilloma**
- 40% occur in 4th ventricle or CPA cistern in adults
- Imaging findings
- Cauliflower- or frond-like excrescences
- Intense, relatively uniform enhancement
- ## Helpful Clues for Rare Diagnoses
- **Astrocytomas**
- **Glioblastoma**
- Infratentorial glioblastomas (GBM) rare
- Typically necrotic, ring enhancing
- **Anaplastic Astrocytoma**
- Rare in infratentorial area
- Infiltrative, variable enhancement
- **Low-****Grade Diffuse Astrocytoma**
- Young adults
- Focal or diffuse T2-hyperintense white matter mass, usually nonenhancing
- Enhancement suggests conversion to higher grade
- **Pilocytic Astrocytoma**
- Rare in adults
- Cystic mass with enhancing nodule typical
- **G****lomus Jugulare****Paraganglioma**
- Spreads superolaterally into middle ear much more frequently than superomedially into CPA
- Imaging findings
- Intense heterogeneous enhancement
- Look for salt and pepper flow voids
- Permeative; destructive, infiltrative
- **Dysplastic Cerebellar Gangliocytoma (Lhermitte-Duclos)**
- May be familial or sporadic
- Molecular studies suggest high frequency of alterations in PTEN-AKT-mTOR pathway
- Association with Cowden syndrome
- Autosomal dominant; germline mutation in *PTEN*tumor suppressor gene
- ↑ risk of breast, thyroid, genitourinary malignancy, & mucocutaneous lesions
- Imaging findings
- Widened, irregular cerebellar folia with ↑ T2
- Layered/laminated or tiger stripes appearance
- May cause significant mass effect
- Typically does not enhance (rarely may)
- **Medulloblastoma (Desmoplastic Variant)**
- Desmoplastic variant more common in 2nd-3rd decades
- Imaging findings
- Off-midline (lateral cerebellar hemisphere) location
- Enhances; cerebrospinal fluid spread uncommon
- **Hemangiopericytoma**
- Highly cellular & vascularized mesenchymal tumor mimics meningioma
- Imaging findings
- Lobular, avidly enhancing, extraaxial mass with dural attachment; ± skull erosion
- Mimics meningioma, but no calcifications or hyperostosis; often heterogeneous
- Commonly involve falx, tentorium, or dural sinuses; occipital most common
- Dural tail seen in ~ 50%
- **Ecchordosis Physaliphora**
- Small, gelatinous mass considered ectopic notochordal remnant
- Midline of craniospinal axis from dorsum sellae to sacrococcygeal region
- Erosion dorsal clivus to PF
- Found in 2% of autopsies, typically asymptomatic
- Imaging findings
- Hypointense on T1, hyperintense on T2
- No enhancement
- ± stalk-like connection to mass
## References
# Selected References
1. [Moinuddin FM et al: Bilateral lateral ventricular subependymoma with extensive multiplicity presenting with hemorrhage. Neuroradiol J. 31(1):27-31, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=28696174%5Bpmid%5D)
1. [Shrot S et al: Dysplasia and overgrowth: magnetic resonance imaging of pediatric brain abnormalities secondary to alterations in the mechanistic target of rapamycin pathway. Neuroradiology. 60(2):137-150, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=29279945%5Bpmid%5D)
1. [Jiang T et al: Lhermitte-Duclos disease (dysplastic gangliocytoma of the cerebellum) and Cowden syndrome: clinical experience from a single institution with long-term follow-up. World Neurosurg. 104:398-406, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=28479525%5Bpmid%5D)
1. [Ciccarino P et al: Multifocal presentation of medulloblastoma in adulthood. J Neurooncol. 107(2):233-7, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22071791%5Bpmid%5D)
1. [Solis OE et al: Rosette-forming glioneuronal tumor: a pineal region case with IDH1 and IDH2 mutation analyses and literature review of 43 cases. J Neurooncol. 102(3):477-84, 2011](http://www.ncbi.nlm.nih.gov/pubmed/?term=20872044%5Bpmid%5D)
1. [Goddard JC et al: Fundal fluid as a predictor of hearing preservation in the middle cranial fossa approach for vestibular schwannoma. Otol Neurotol. 31(7):1128-34, 2010](http://www.ncbi.nlm.nih.gov/pubmed/?term=20657334%5Bpmid%5D)
1. [Koyfman SA et al: Stereotactic radiosurgery for single brainstem metastases: the cleveland clinic experience. Int J Radiat Oncol Biol Phys. 78(2):409-14, 2010](http://www.ncbi.nlm.nih.gov/pubmed/?term=20133072%5Bpmid%5D)
1. [Andres RH et al: Lhermitte-Duclos disease with atypical vascularization--case report and review of the literature. Clin Neuropathol. 28(2):83-90, 2009](http://www.ncbi.nlm.nih.gov/pubmed/?term=19353838%5Bpmid%5D)
1. [Bonneville F et al: Imaging of cerebellopontine angle lesions: an update. Part 1: enhancing extra-axial lesions. Eur Radiol. 17(10):2472-82, 2007](http://www.ncbi.nlm.nih.gov/pubmed/?term=17562049%5Bpmid%5D)
1. [Bonneville F et al: Imaging of cerebellopontine angle lesions: an update. Part 2: intra-axial lesions, skull base lesions that may invade the CPA region, and non-enhancing extra-axial lesions. Eur Radiol. 17(11):2908-20, 2007](http://www.ncbi.nlm.nih.gov/pubmed/?term=17569053%5Bpmid%5D)
1. [Recinos PF et al: Brainstem tumors: where are we today? Pediatr Neurosurg. 43(3):192-201, 2007](http://www.ncbi.nlm.nih.gov/pubmed/?term=17409788%5Bpmid%5D)
1. [Koeller KK et al: From the archives of the AFIP: medulloblastoma: a comprehensive review with radiologic-pathologic correlation. Radiographics. 23(6):1613-37, 2003](http://www.ncbi.nlm.nih.gov/pubmed/?term=14615567%5Bpmid%5D)
1. [Zabek M: Primary posterior fossa tumours in adult patients. Folia Neuropathol. 41(4):231-6, 2003](http://www.ncbi.nlm.nih.gov/pubmed/?term=14977253%5Bpmid%5D)
## Images
### Selected Images
 involving the right cerebellopontine angle cistern and extending into the internal auditory canal
involving the right cerebellopontine angle cistern and extending into the internal auditory canal  .](images/app.statdx.com_image_thumbnail_df62b1b1-e2f2-4f73-8cb3-009ad02b8459_annotated_true_size_900_quality_90_72e555ee76ab95be5f3dc1dafc3b9f3573533a66.jpg)
**Vestibular Schwannoma**
*Axial T1 C+ MR shows a partly cystic and solid, heterogeneously enhancing, vestibular schwannoma involving the right cerebellopontine angle cistern and extending into the internal auditory canal .*
**Vestibular Schwannoma**
*Axial T1 C+ MR shows a partly cystic and solid, heterogeneously enhancing, vestibular schwannoma involving the right cerebellopontine angle cistern and extending into the internal auditory canal .*

**Vestibular Schwannoma**
*Axial T1 C+ MR shows a partly cystic and solid, heterogeneously enhancing, vestibular schwannoma involving the right cerebellopontine angle cistern and extending into the internal auditory canal .*

**Vestibular Schwannoma**
*Axial T1 C+ MR shows a partly cystic and solid, heterogeneously enhancing, vestibular schwannoma involving the right cerebellopontine angle cistern and extending into the internal auditory canal .*

**Vestibular Schwannoma**
*Axial T1 C+ MR shows a partly cystic and solid, heterogeneously enhancing, vestibular schwannoma involving the right cerebellopontine angle cistern and extending into the internal auditory canal .*

**Vestibular Schwannoma**
*Axial T1 C+ MR shows a partly cystic and solid, heterogeneously enhancing, vestibular schwannoma involving the right cerebellopontine angle cistern and extending into the internal auditory canal .*
 in the right cerebellopontine angle cistern. The mass has a broad base toward the dural surface. Note the dural tail sign
in the right cerebellopontine angle cistern. The mass has a broad base toward the dural surface. Note the dural tail sign  of reactive meningeal thickening in the internal auditory canal.](images/app.statdx.com_image_thumbnail_b79aca2e-1ac7-4379-a472-983bd7113c88_annotated_true_size_900_quality_90_0e416a56e6e47f3ef2a115826374038901501872.jpg)
**Meningioma in Cerebellopontine Angle**
*Axial T1 C+ MR shows a large, mushroom-shaped, enhancing mass in the right cerebellopontine angle cistern. The mass has a broad base toward the dural surface. Note the dural tail sign of reactive meningeal thickening in the internal auditory canal.*
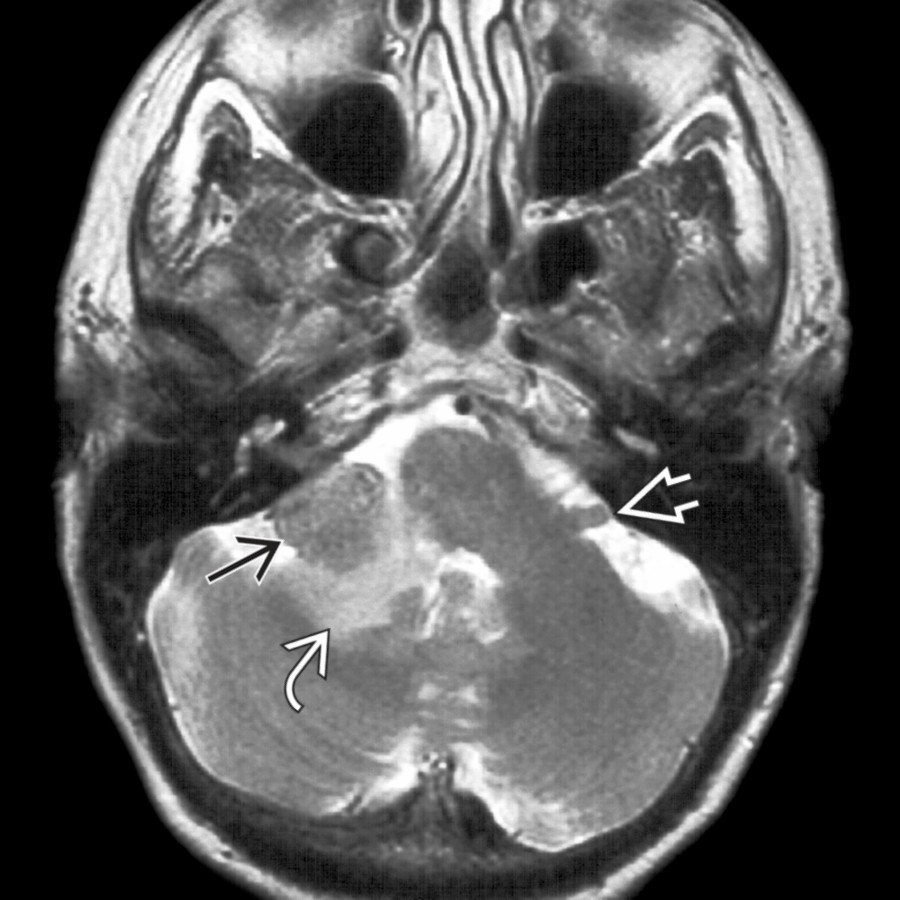
**Metastases in Cerebellopontine Angle**
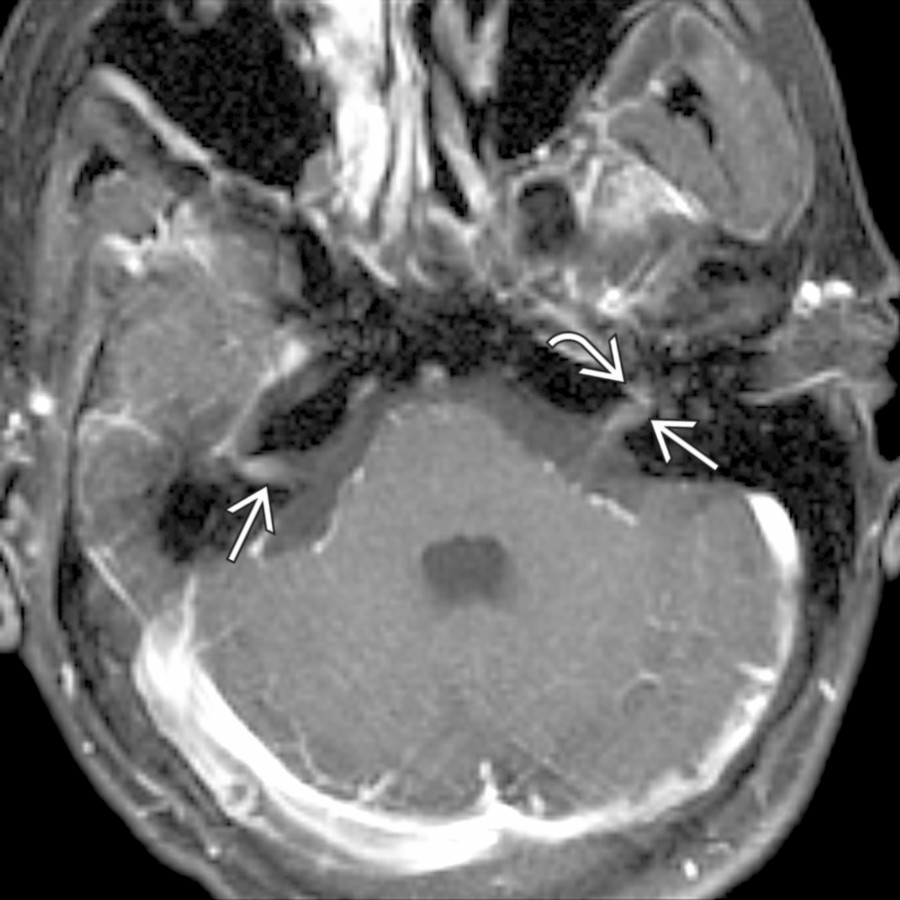
*Axial T2 MR in a female patient with breast carcinoma shows a lobulated extraaxial mass in the right flocculus with associated parenchymal edema . Note the normal flocculus on the left .*
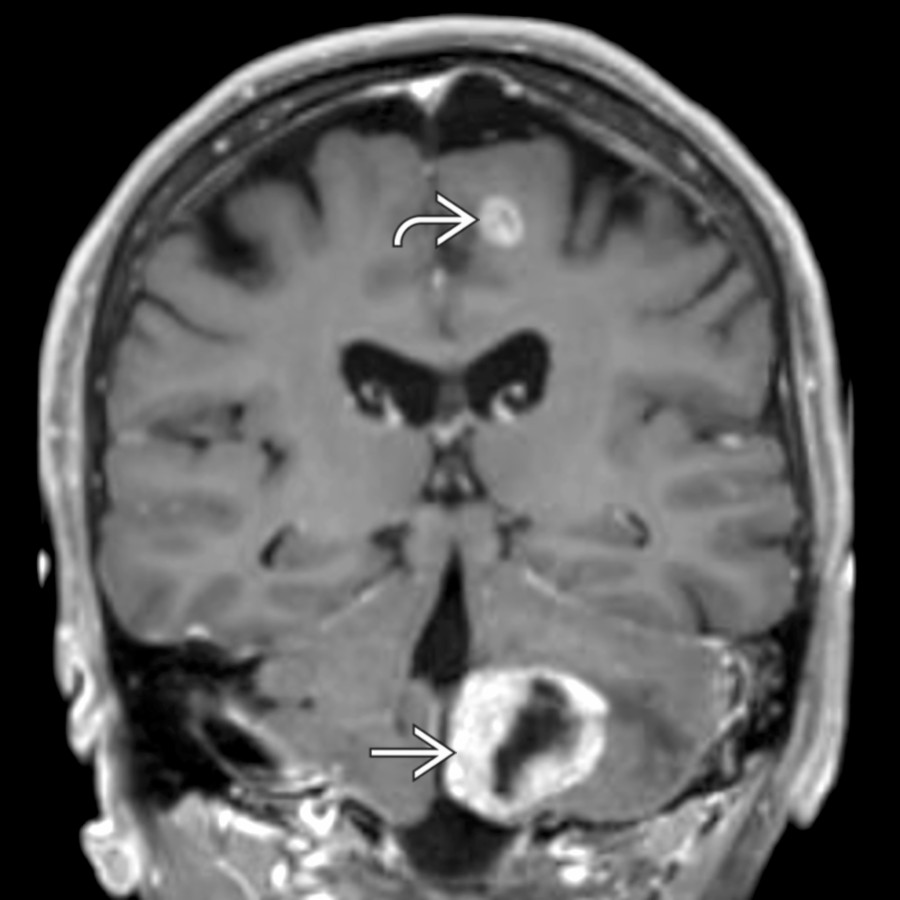
**Metastasis in Brainstem or Cerebellum**
*Coronal T1 C+ MR demonstrates a partly cystic, partly solid enhancing mass in the left cerebellar hemisphere with surrounding vasogenic edema. A 2nd enhancing mass in the left frontal lobe increases suspicion for metastatic disease in this patient with lung cancer (confirmed histologically).*
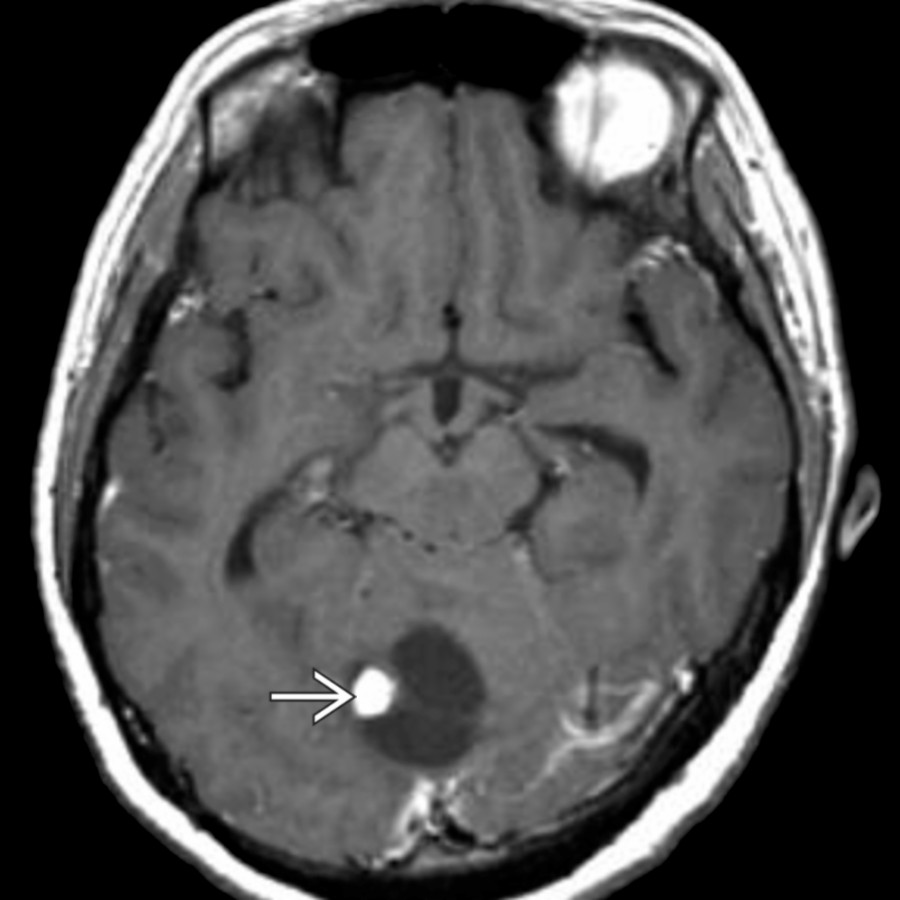
**Hemangioblastoma**
*Axial T1 C+ MR in a patient with von Hippel-Lindau syndrome shows a cystic cerebellar mass with a nodule of enhancement , typical of hemangioblastoma. Retinal angiomas and an additional posterior fossa hemangioblastoma were also present (not shown).*

**Jugular Foramen Schwannoma**
*Axial T1 C+ MR shows a large, solid, intensely enhancing, extraaxial mass extending into the enlarged, smoothly remodeled jugular foramen . Intratumoral cysts, not present here, are common in posterior fossa schwannomas.*

**Subependymoma**
*Axial T2 MR shows an unusually large lateral ventricle subependymoma causing obstructive hydrocephalus. Note the heterogeneous internal signal intensity. No enhancement was seen (not shown), typical of subependymomas. Subependymomas are more often small, incidentally discovered masses.*

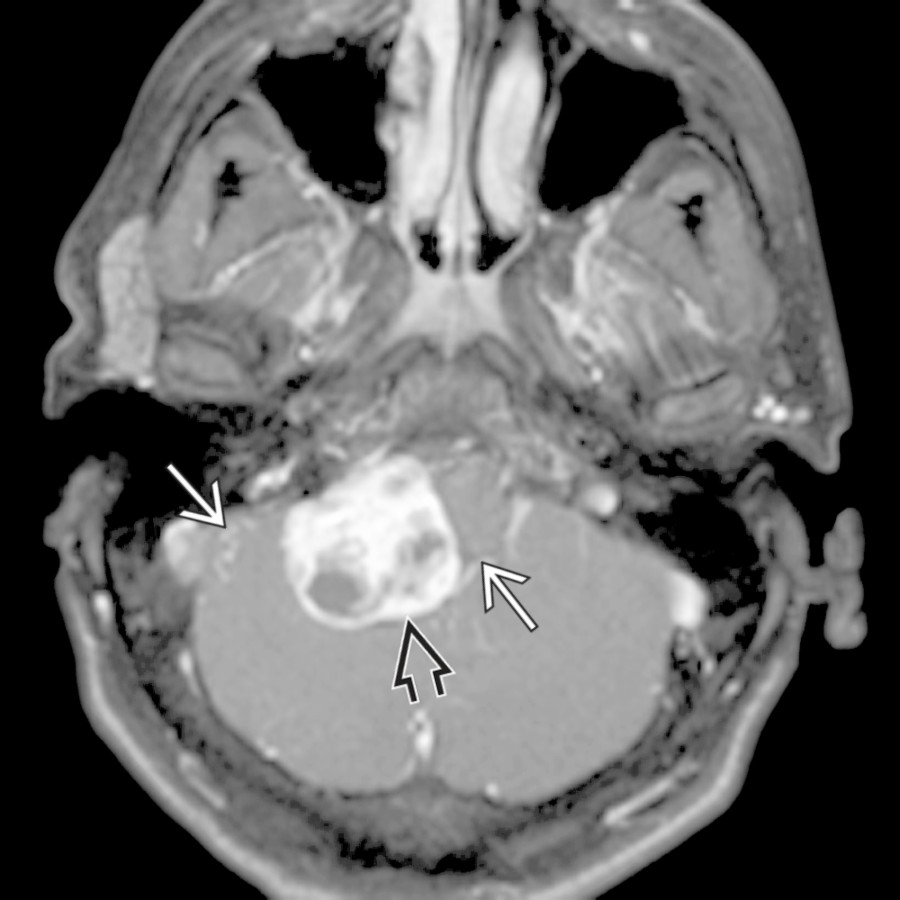
**Choroid Plexus Papilloma**
*Coronal T1 C+ MR in a 43-year-old woman with headaches shows a "speckled" or "bubbly," heterogeneously enhancing mass in the 4th ventricle with extension into the lateral recess .*

**Astrocytomas**
*Axial T1 C+ MR in an older teenager with nausea and vomiting shows an inhomogeneously enhancing vermian mass with cystic and solid components. Preoperative diagnosis was malignant astrocytoma. However, a WHO grade II tumor was found at biopsy.*

**Low-Grade Diffuse Astrocytoma**
*Sagittal T2 MR in a 25-year-old woman with lower cranial nerve palsies shows a dorsally exophytic pontomedullary mass . Biopsy proved WHO grade II astrocytoma.*

**Dysplastic Cerebellar Gangliocytoma (Lhermitte-Duclos)**
*Axial T2 MR shows enlargement and hyperintensity involving the left cerebellar hemisphere . Note the classic tiger stripes appearance with overall preserved cerebellar foliar architecture.*

**Medulloblastoma (Desmoplastic Variant)**
*Axial T2 MR in a 26-year-old man shows an inhomogeneously hyperintense mass in the lateral cerebellum . The mass enhanced heterogeneously (not shown). This is typical of desmoplastic medulloblastoma, although an atypical teratoid rhabdoid tumor could be considered in a child.*

**Meningioma in Cerebellopontine Angle**
*Axial T1 C+ MR shows a large, mushroom-shaped, enhancing mass in the right cerebellopontine angle cistern. The mass has a broad base toward the dural surface. Note the dural tail sign of reactive meningeal thickening in the internal auditory canal.*

**Metastases in Cerebellopontine Angle**
*Axial T2 MR in a female patient with breast carcinoma shows a lobulated extraaxial mass in the right flocculus with associated parenchymal edema . Note the normal flocculus on the left .*

**Metastasis in Brainstem or Cerebellum**
*Coronal T1 C+ MR demonstrates a partly cystic, partly solid enhancing mass in the left cerebellar hemisphere with surrounding vasogenic edema. A 2nd enhancing mass in the left frontal lobe increases suspicion for metastatic disease in this patient with lung cancer (confirmed histologically).*

**Hemangioblastoma**
*Axial T1 C+ MR in a patient with von Hippel-Lindau syndrome shows a cystic cerebellar mass with a nodule of enhancement , typical of hemangioblastoma. Retinal angiomas and an additional posterior fossa hemangioblastoma were also present (not shown).*

**Jugular Foramen Schwannoma**
*Axial T1 C+ MR shows a large, solid, intensely enhancing, extraaxial mass extending into the enlarged, smoothly remodeled jugular foramen . Intratumoral cysts, not present here, are common in posterior fossa schwannomas.*

**Subependymoma**
*Axial T2 MR shows an unusually large lateral ventricle subependymoma causing obstructive hydrocephalus. Note the heterogeneous internal signal intensity. No enhancement was seen (not shown), typical of subependymomas. Subependymomas are more often small, incidentally discovered masses.*

**Choroid Plexus Papilloma**
*Coronal T1 C+ MR in a 43-year-old woman with headaches shows a "speckled" or "bubbly," heterogeneously enhancing mass in the 4th ventricle with extension into the lateral recess .*

**Astrocytomas**
*Axial T1 C+ MR in an older teenager with nausea and vomiting shows an inhomogeneously enhancing vermian mass with cystic and solid components. Preoperative diagnosis was malignant astrocytoma. However, a WHO grade II tumor was found at biopsy.*

**Low-Grade Diffuse Astrocytoma**
*Sagittal T2 MR in a 25-year-old woman with lower cranial nerve palsies shows a dorsally exophytic pontomedullary mass . Biopsy proved WHO grade II astrocytoma.*

**Dysplastic Cerebellar Gangliocytoma (Lhermitte-Duclos)**
*Axial T2 MR shows enlargement and hyperintensity involving the left cerebellar hemisphere . Note the classic tiger stripes appearance with overall preserved cerebellar foliar architecture.*

**Medulloblastoma (Desmoplastic Variant)**
*Axial T2 MR in a 26-year-old man shows an inhomogeneously hyperintense mass in the lateral cerebellum . The mass enhanced heterogeneously (not shown). This is typical of desmoplastic medulloblastoma, although an atypical teratoid rhabdoid tumor could be considered in a child.*
 and extracranial
and extracranial  components.](d5c83b0f-e7b6-4a26-a580-379ccbbce549)
**Hemangiopericytoma**
*Axial T1 C+ MR shows a large, inhomogeneously enhancing, destructive, transcalvarial mass with both intracranial and extracranial components.*

**Ecchordosis Physaliphora**
*Sagittal T1 MR shows a midline mass in front of and indenting the pons . Note the slightly increased signal of the mass relative to CSF. There is loss of a normal hypointense cortical margin in the clivus from which the mass originates. The mass was extremely hyperintense on T2 MR, consistent with its notochordal remnant origin.*
### Additional Images
**Metastases in Cerebellopontine Angle**
*Axial T1 C+ MR in a patient with adenocarcinoma shows enhancing metastatic lesions in both IAC cisterns . Note the transmodiolar extension on left .*

**Metastasis in Brainstem or Cerebellum**
*Axial T1 C+ FS MR shows a large, enhancing, cerebellar mass . A 2nd mass in the left temporal lobe makes a diagnosis of metastases in a patient with known renal cell carcinoma easy.*
**Hemangioblastoma**
*Axial T1 C+ FS MR shows a mixed, solid, cystic enhancing mass in the cerebellum . Note the enlarged vessels , suggesting hypervascularity. A solid/mixed solid lesion with intratumoral cysts is less common than classic hemangioblastoma (a nodule and nonenhancing cyst).*

**Subependymoma**
*Sagittal T2 MR shows a small, mildly hyperintense mass in the inferior 4th ventricle, found incidentally in this 43-year-old man with headache and trigeminal neuralgia. No hydrocephalus was identified. Diagnosis was presumed subependymoma.*

**Glomus Jugulare Paraganglioma**
*Axial T1 C+ FS MR shows a large, strongly enhancing, glomus jugulare paraganglioma centered in the jugular foramen. The destructive, erosive nature of the tumor is readily apparent with extension into the EAC .*

**Dysplastic Cerebellar Gangliocytoma (Lhermitte-Duclos)**
*Coronal T2 MR shows enlarged, dysplastic-appearing cerebellar folia with a striated, mixed hyper-/isointense mass in the right cerebellum .*

*Axial T1 C+ MR in a 50-year-old man with supratentorial primary CNS lymphoma shows a subependymal/choroid plexus as well as dural-based spread of the tumor.*

**Ecchordosis Physaliphora**
*Axial T2 FS MR shows a lobulated, hyperintense, extraaxial mass indenting the pons. Note the subtle clival involvement with focal destruction of a bony cortex typical of ecchordosis physaliphora.*
components.](d5c83b0f-e7b6-4a26-a580-379ccbbce549)
**Hemangiopericytoma**
*Axial T1 C+ MR shows a large, inhomogeneously enhancing, destructive, transcalvarial mass with both intracranial and extracranial components.*

**Ecchordosis Physaliphora**
*Sagittal T1 MR shows a midline mass in front of and indenting the pons . Note the slightly increased signal of the mass relative to CSF. There is loss of a normal hypointense cortical margin in the clivus from which the mass originates. The mass was extremely hyperintense on T2 MR, consistent with its notochordal remnant origin.*
### Additional Images

**Metastases in Cerebellopontine Angle**
*Axial T1 C+ MR in a patient with adenocarcinoma shows enhancing metastatic lesions in both IAC cisterns . Note the transmodiolar extension on left .*

**Metastasis in Brainstem or Cerebellum**
*Axial T1 C+ FS MR shows a large, enhancing, cerebellar mass . A 2nd mass in the left temporal lobe makes a diagnosis of metastases in a patient with known renal cell carcinoma easy.*

**Hemangioblastoma**
*Axial T1 C+ FS MR shows a mixed, solid, cystic enhancing mass in the cerebellum . Note the enlarged vessels , suggesting hypervascularity. A solid/mixed solid lesion with intratumoral cysts is less common than classic hemangioblastoma (a nodule and nonenhancing cyst).*

**Subependymoma**
*Sagittal T2 MR shows a small, mildly hyperintense mass in the inferior 4th ventricle, found incidentally in this 43-year-old man with headache and trigeminal neuralgia. No hydrocephalus was identified. Diagnosis was presumed subependymoma.*

**Glomus Jugulare Paraganglioma**
*Axial T1 C+ FS MR shows a large, strongly enhancing, glomus jugulare paraganglioma centered in the jugular foramen. The destructive, erosive nature of the tumor is readily apparent with extension into the EAC .*

**Dysplastic Cerebellar Gangliocytoma (Lhermitte-Duclos)**
*Coronal T2 MR shows enlarged, dysplastic-appearing cerebellar folia with a striated, mixed hyper-/isointense mass in the right cerebellum .*

*Axial T1 C+ MR in a 50-year-old man with supratentorial primary CNS lymphoma shows a subependymal/choroid plexus as well as dural-based spread of the tumor.*

**Ecchordosis Physaliphora**
*Axial T2 FS MR shows a lobulated, hyperintense, extraaxial mass indenting the pons. Note the subtle clival involvement with focal destruction of a bony cortex typical of ecchordosis physaliphora.*