---
title: "Posterior Fossa Neoplasm, Pediatric"
docid: "22c55144-5db6-4235-9292-de3dd1315dd2"
authors:
- key: "f184750a-90b4-47a7-907b-23b05d70357a"
value: "Chang Yueh Ho, MD"
- key: "e8af6d26-3aad-47c9-9083-5128aab09af2"
value: "Susan I. Blaser, MD, FRCPC"
breadcrumbs:
-
name: "Head and Neck"
slug: "head-and-neck"
treeNodeId: "ed24ed8c-5d57-4629-879b-447b82d2973d"
-
name: "Differential Diagnosis"
slug: "differential-diagnosis"
treeNodeId: "40d68862-8975-4dde-ac2b-ebc43ab0fb5c"
-
name: "CPA-IAC and Posterior Fossa"
slug: "cpa-iac-and-posterior-fossa"
treeNodeId: "c590eedb-4a3b-4158-a04f-ad880564c992"
-
name: "Anatomically Based Differentials"
slug: "anatomically-based-differentials"
treeNodeId: "debfb06c-8656-4f5d-92c1-eaa468185d78"
-
name: "Posterior Fossa Neoplasm, Pediatric"
slug: "posterior-fossa-neoplasm-pediatric"
treeNodeId: null
category: "Head and Neck"
documentVersionId: "f9182a7b-2287-4827-8cc9-fd986d37f943"
imageCount: 57
lastUpdated: "08/20/18"
pageDescription: "Posterior Fossa Neoplasm, Pediatric"
pageKeywords: "Head and Neck, Differential Diagnosis, CPA-IAC and Posterior Fossa, Anatomically Based Differentials, Posterior Fossa Neoplasm, Pediatric"
pageTitle: "Posterior Fossa Neoplasm, Pediatric | STATdx"
enhancedTitle: "Posterior Fossa Neoplasm, Pediatric"
type: "DDX"
references: true
breadcrumbs:
- "Head and Neck"
- "Differential Diagnosis"
- "CPA-IAC and Posterior Fossa"
- "Anatomically Based Differentials"
- "Posterior Fossa Neoplasm, Pediatric"
---
# ESSENTIAL INFORMATION
- ## Key Differential Diagnosis Issues
- Unlike in adults, primary neoplasm is more common than metastases in children
- Most common pediatric posterior fossa neoplasms
- Astrocytomas: Pilocytic astrocytoma (PA), infiltrating glioma (astrocytoma, WHO grade II)
- Medulloblastoma
- Ependymoma
- Imaging
- Location helpful in differential diagnosis
- Tectum, cerebellum: PA
- Pons: Diffusely infiltrating astrocytomas
- Midline (vermis, 4th ventricle): Medulloblastoma, PA
- 4th ventricle + lateral recess/CPA mass: Ependymoma
- Diffusion-weighted imaging
- Can discriminate between high-grade & low-grade pediatric posterior fossa tumors
- Medulloblastoma & atypical teratoid-rhabdoid tumor (ATRT) show DWI restriction
- Examine entire neuraxis in child with posterior fossa tumor prior to surgery
- T1 C+ essential (look for CSF spread)
- ## Helpful Clues for Common Diagnoses
- **Pilocytic Astrocytoma**
- Child with cystic cerebellar hemispheric mass + enhancing mural nodule
- Solid component low-density NECT, high-signal T2
- **Medulloblastoma**
- Most common malignant pediatric brain tumor
- Most common 4th ventricular neoplasm of childhood
- Arises from vermis & fills 4th ventricle
- Hydrocephalus common
- Hemispheric involvement is less common
- Hypercellular: ↑ density on NECT, ↓ T2
- DWI: Decreased diffusion
- Previous classification based on histopathology: Desmoplastic/nodular; medulloblastoma with extensive nodularity; classic, large cell, & anaplastic variants
- Current classification with molecular subgroups predicts outcomes better
- Wingless (WNT): CPA predilection; uncommon in infants; good prognosis
- Associated with Turcot syndrome
- Sonic hedgehog (SHH): Cerebellar hemispheric location; good prognosis in infants; intermediate in older children & adults
- Associated with Gorlin syndrome
- Medulloblastoma with extensive nodularity & desmoplastic variants
- Group 3: 4th ventricle; ill-defined tumor margin; seen in infants & children; poor prognosis
- Group 4: 4th ventricle; minimal to no enhancement; intermediate prognosis seen in infants to adults
- **Ependymoma**
- Extrudes through 4th ventricle outlet foramina into cisterns
- Coarse calcifications
- Diffusion restriction uncommon, may predict anaplastic behavior
- **Brainstem Glioma, Pediatric**
- Exophytic brainstem tumors are typically low grade, PA, or diffuse astrocytoma
- Good outcome, may require chemotherapy or ventricular shunting for sequela of mass effect
- Tectal plate glioma
- NECT: Increased density progresses to Ca⁺⁺
- CECT/MR: Faint or no enhancement
- Dorsal exophytic glioma
- Tumor protrudes into 4th ventricle
- If large, may be difficult to differentiate from PA
- Look for FLAIR signal change in dorsal brainstem or peduncles
- **Diffuse Intrinsic Pontine Glioma**
- Poor prognosis; near 100% mortality
- Expansile T2-hyperintense mass affecting at least 50% of central pons
- Enlarged pons engulfs basilar artery
- Enhances late in course, rarely at diagnosis
- Associated with histone mutations (H3-K27M)
- H3-K27M diffuse midline gliomas occur in pons, thalamus, & spinal cord
- H3-K27M midline gliomas have variable radiologic presentation, from nonenhancing, expansile T2 hyperintensity to central necrosis with peripheral enhancement
- ## Helpful Clues for Less Common Diagnoses
- **Ganglioglioma**
- Brainstem most common posterior fossa site
- Look for expansion of nucleus cuneatus/gracilis
- **Schwannoma**
- Contrast-enhancing masses along cranial nerves: Vestibular schwannoma (ICA/CPA) looks like ice cream on cone
- T2 hyperintensity helps differentiate from meningioma
- Multiple in neurofibromatosis type 2 (NF2)
- **Meningioma, CPA-IAC**
- Broad dural base, covers IAC
- Variable signal, but T2 hypointensity common
- Hyperostosis, tumoral calcifications
- May have intra- or juxtatumoral cyst(s)
- Uncommon in children
- Consider NF2
- **Hemangioblastoma**
- Late teen or adult
- Intraaxial (cerebellum > medulla, cord)
- Cyst + nodule > solid
- Solid component shows flow voids, enhances avidly
- Multiple lesions diagnostic of von Hippel-Lindau (VHL)
- Avidly enhancing mural nodule abuts pia
- Look for visceral markers of VHL in any child/young adult with hemangioblastoma
- **Choroid Plexus Papilloma**
- Frond-like 4th ventricle or CPA tumor
- Avidly enhancing
- Hydrocephalus common
- ## Helpful Clues for Rare Diagnoses
- **Anaplastic Astrocytoma**
- Infiltrating mass involves predominantly white matter
- Enhancement none to sparse or patchy enhancement
- Ring enhancement suggests progression to glioblastoma
- **Atypical Teratoid-Rhabdoid Tumor**
- Imaging similar to medulloblastoma
- ATRT patients generally younger
- Cysts, hemorrhages more common
- CPA involvement more common
- Frequent metastases at diagnosis
- Both ATRT, medulloblastoma show diffusion restriction
- **Choroid Plexus Carcinoma**
- Similar to choroid plexus papilloma plus
- Cysts, necrosis, bleeds
- CSF/ependymal/parenchymal spread
- **Medulloblastoma Variants**
- Desmoplastic medulloblastoma
- 5-25% of all medulloblastomas
- 55-60% of medulloblastomas in children < 3 years old
- Associated with SHH subgroup
- Desmoplastic subtype of medulloblastoma in children < 2 is major diagnostic criterion for basal cell nevus syndrome (Gorlin syndrome)
- Nodular collections of neurocytic cells bounded by desmoplastic zones
- Lateral (cerebellar) location
- Medulloblastoma with extensive nodularity
- Formerly called cerebellar neuroblastoma
- Usually occurs in infants
- Gyriform or grape-like appearance
- May mature → better prognosis
- Associated with SHH subgroup
- **Medulloepithelioma**
- Rare embryonal brain &/or ocular tumor
- Heterogeneous signal, enhancement
- **Embryonal Tumor With Multilayered Rosettes**
- Aggressive primitive neuroectodermal tumor, subtype of CNS embryonal tumor
- Ependymoblastic rosettes
- Previously termed embryonal tumor with abundant neuropil & true rosettes
- Occurs < 4 years of age
- Large mass with heterogeneous contrast enhancement
- Can occur both supra- & infratentorially
- **Dysplastic Cerebellar Gangliocytoma**
- Diffuse or focal hemispheric mass
- Thick cerebellar folia with striated appearance
- Evaluate for Cowden syndrome
## References
# Selected References
1. [Johnson DR et al: 2016 updates to the WHO brain tumor classification system: what the radiologist needs to know. Radiographics. 37(7):2164-2180, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=29028423%5Bpmid%5D)
1. [Vijapura C et al: Genetic syndromes associated with central nervous system tumors. Radiographics. 37(1):258-280, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=27911673%5Bpmid%5D)
1. [Castel D et al: Histone H3F3A and HIST1H3B K27M mutations define two subgroups of diffuse intrinsic pontine gliomas with different prognosis and phenotypes. Acta Neuropathol. 130(6):815-27, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=26399631%5Bpmid%5D)
1. [Taylor MD et al: Molecular subgroups of medulloblastoma: the current consensus. Acta Neuropathol. 123(4):465-72, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22134537%5Bpmid%5D)
## Images
### Selected Images
 . Note the effacement of the 4th ventricle
. Note the effacement of the 4th ventricle  rather than expansion, which would be typical for medulloblastoma and ependymomas.](images/app.statdx.com_image_thumbnail_c50cb67e-93c0-4b5d-89c2-2c6bced6e023_annotated_true_size_900_quality_90_85e40bf8703443bd140eeb79008269b6a5ab6ecf.jpg)
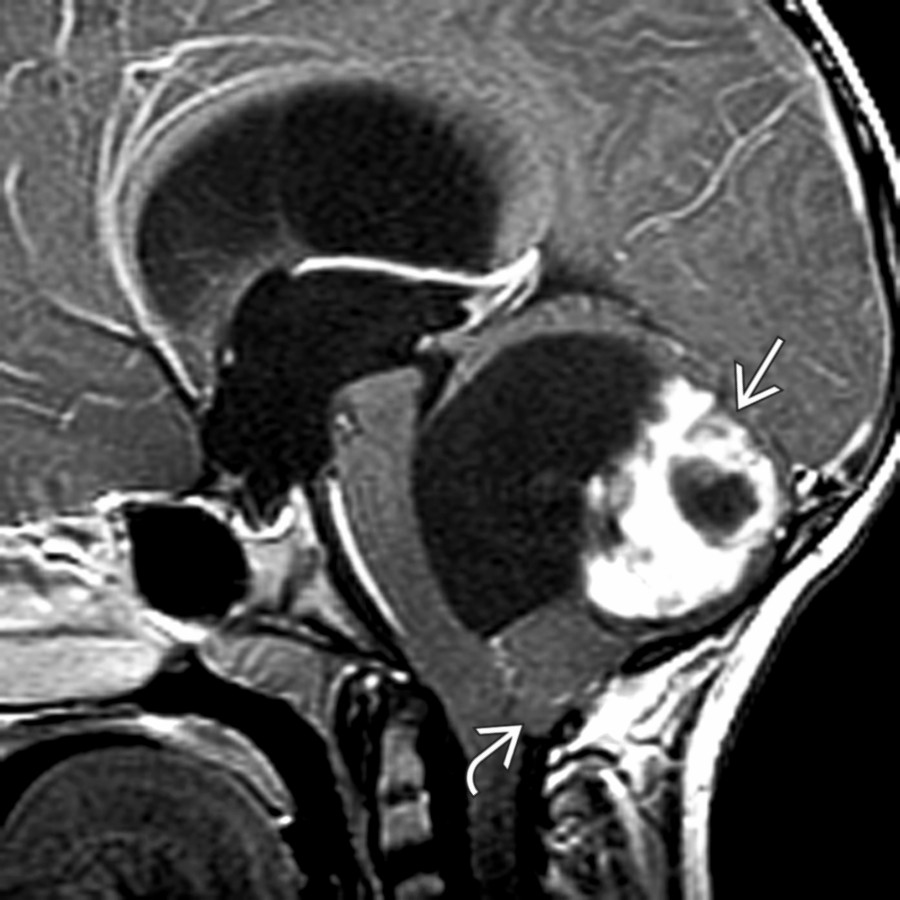
**Pilocytic Astrocytoma**
*Sagittal T1 C+ FS MR shows a pilocytic astrocytoma involving the cerebellum with heterogeneous enhancement and a large cyst . Note the effacement of the 4th ventricle rather than expansion, which would be typical for medulloblastoma and ependymomas.*
**Pilocytic Astrocytoma**
*Sagittal T1 C+ FS MR shows a pilocytic astrocytoma involving the cerebellum with heterogeneous enhancement and a large cyst . Note the effacement of the 4th ventricle rather than expansion, which would be typical for medulloblastoma and ependymomas.*

**Pilocytic Astrocytoma**
*Axial T2 FS MR shows a T2-hyperintense solid mass filling the 4th ventricle. Postcontrast enhancement was seen (not shown), consistent with pilocytic astrocytoma. Low-grade tumors typically have a T2-hyperintense signal of the tumor parenchyma.*

**Medulloblastoma**
*Axial T1 C+ FS MR shows a heterogeneously enhancing mass filling the 4th ventricle. This was a group 1 medulloblastoma with Wingless (WNT) activation. These are rare medulloblastomas, but they have a very good prognosis. They are typically seen near the cerebellopontine angle in older children.*
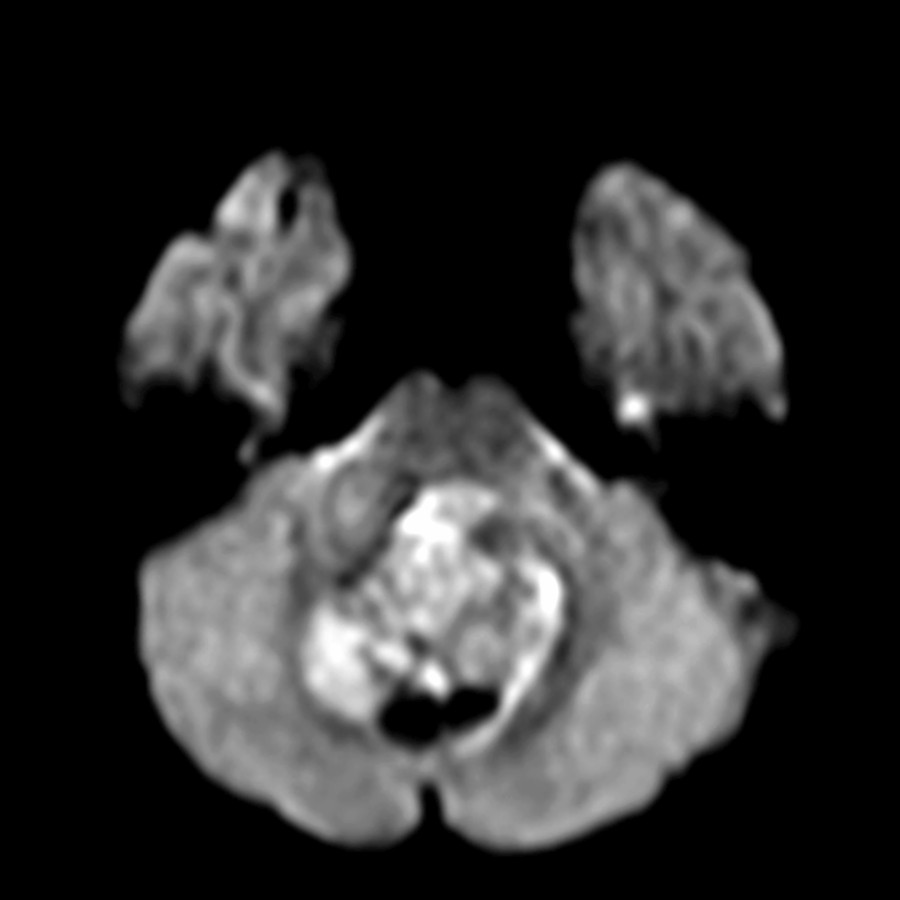
**Medulloblastoma**
*Axial DWI MR shows areas of decreased diffusion in this WNT pathway medulloblastoma. Decreased diffusion is typical for all medulloblastomas and high- grade neoplasms.*

**Medulloblastoma**
*Axial T2 MR in an infant shows an isointense nodular mass within the 4th ventricle with associated cerebellar edema . This neoplasm demonstrated intense enhancement and decreased diffusion (not shown). This neoplasm was SHH-activated, group 2 medulloblastoma classified histologically as a medulloblastoma with extensive nodularity.*
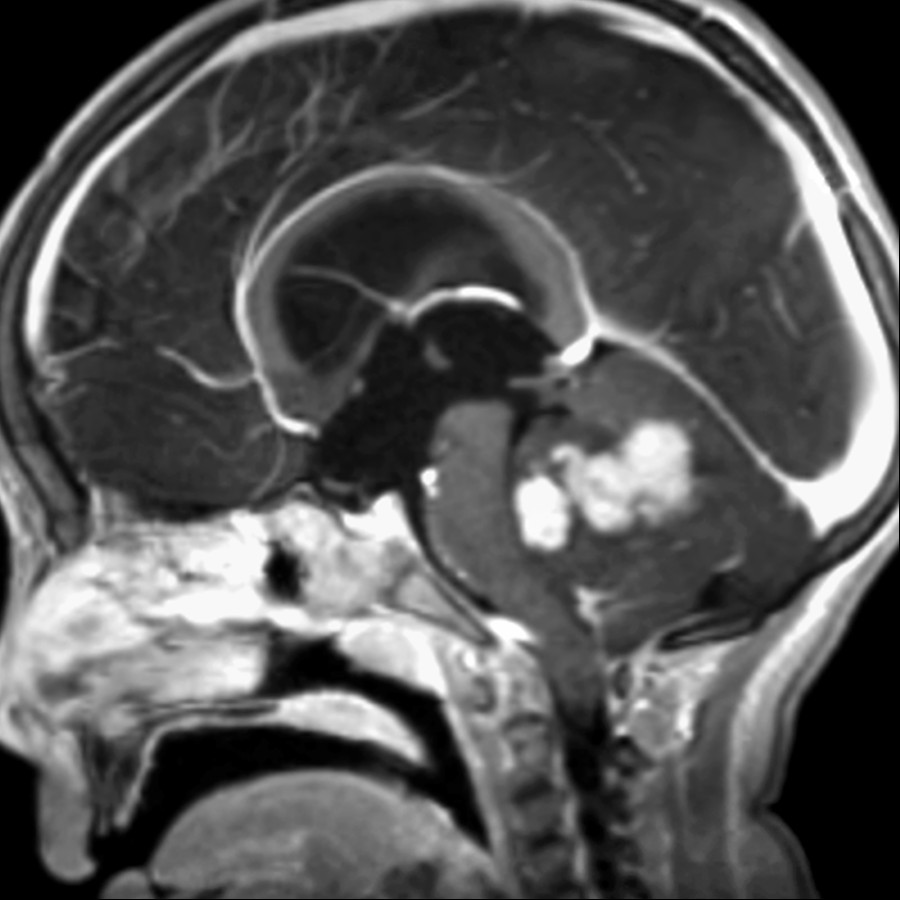
**Medulloblastoma**
*Sagittal T1 C+ MR shows nodular enhancement in this group 3 medulloblastoma, which has a poor outcome compared to other subgroups.*

**Medulloblastoma**
*Sagittal T1 C+ FS MR shows a minimally enhancing mass within the 4th ventricle . This is consistent with a group 4 medulloblastoma, which arises in the classic location but has minimal enhancement.*

**Medulloblastoma**
*Axial DWI MR shows that the intraventricular tumor has nearly uniform decreased diffusion compatible with a high-grade neoplasm. Despite minimal contrast enhancement, group 4 medulloblastomas show decreased diffusion. This most common subgroup has an intermediate prognosis.*

**Ependymoma**
*Axial T2 FS MR shows a T2 iso- to hyperintense mass filling the 4th ventricle but extending through the foramina inferiorly, particularly the right foramen of Luschka . This is a typical appearance for a posterior fossa ependymoma.*

**Brainstem Glioma, Pediatric**
*Sagittal T1 MR shows a mass involving the tectal plate, which is consistent with a tectal plate glioma . Pedunculated brainstem gliomas typically are low grade with good prognosis.*

**Diffuse Intrinsic Pontine Glioma**
*Axial FLAIR MR shows a hyperintense mass diffusely expanding the pons and encasing the basilar artery . Unlike pedunculated brain stem tumors, diffuse lesions have a poor prognosis.*

**Diffuse Intrinsic Pontine Glioma**
*Axial T1 C+ FS MR shows minimal asymmetric enhancement of the diffuse pontine mass and effacement of the 4th ventricle . With near 100% mortality, these tumors have been associated with H3-K27M mutations, which also contribute to diffuse midline gliomas in the thalamus and spinal cord.*

**Ganglioglioma**
*Axial T2 FS MR shows a heterogeneous, irregular mass in the left brachium pontis with cystic change and areas of hemorrhage . This was a ganglioglioma at resection.*

**Ganglioglioma**
*Axial T1 C+ FS MR shows that the left middle cerebellar peduncle mass has irregular amorphous contrast enhancement. Note the involvement at the origin of the VII and VIII cranial nerves . This child presented with left sensorineural hearing loss and facial weakness.*

**Schwannoma**
*Axial T1 C+ MR shows an intensely enhancing extraaxial mass displacing the cerebellum & medulla arising below the cerebellopontine angle with extension through the left jugular foramen . There is central cystic nonenhancement , typical for large schwannomas.*

**Meningioma, CPA-IAC**
*Axial T1 C+ MR shows a homogeneous enhancing mass with a broad dural attachment along posterior dura, consistent with meningioma. Schwannomas & meningiomas are rare in children, and neurofibromatosis type 2 should be considered.*

**Hemangioblastoma**
*Sagittal T1 C+ MR shows a cystic mass involving the medulla and upper cervical cord. There are small nodules of enhancement along the rim of the cyst , consistent with hemangioblastoma in a child with von Hippel-Lindau disease.*

**Choroid Plexus Papilloma**
*Axial NECT shows a heavily calcified mass arising from the inferior 4th ventricle and extending into the cisterna magna with dilated temporal horns from obstructive hydrocephalus.*

**Choroid Plexus Papilloma**
*Axial T1 C+ MR shows a lobular enhancing mass at the left cerebellopontine angle without extension into the internal auditory canal. This is a rare location for a choroid plexus papilloma.*

**Anaplastic Astrocytoma**
*Axial T2 FS MR shows a poorly circumscribed infiltrative mass in the left pons, cerebellar peduncle, and deep white matter of the right cerebellum. No significant enhancement with areas of decreased diffusion was seen (not shown). This was a biopsy-proven anaplastic astrocytoma.*

**Atypical Teratoid-Rhabdoid Tumor**
*Axial T2 MR shows a heterogeneous mass with prominent cysts in the 4th ventricle. The solid component of tumor is iso- to hypointense on T2 & is consistent with high-grade neoplasm such as atypical teratoid-rhabdoid tumor (ATRT).*

**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T1 C+ MR shows heterogeneous enhancement of the 4th ventricle with a prominent cyst . Although not exclusive, ATRT tends to have more cystic change than medulloblastoma and other high-grade neoplasms. This tumor also had decreased diffusion (not shown).*

**Medulloblastoma Variants**
*Axial T2 MR shows an isointense mass within the 4th ventricle as well as a nodule in the right cerebellar hemisphere . Involvement of the cerebellar hemisphere in a medulloblastoma is suggestive of group 2 SHH-activation, which is histologically described as desmoplastic or extensive nodularity.*

**Medulloepithelioma**
*Axial DWI MR shows decreased diffusion in this medulloepithelioma involving the pons and right brachium pontis. These tumors are highly malignant and may have metastases to extracranial locations.*

**Embryonal Tumor With Multilayered Rosettes**
*Axial DWI MR shows a tumor with decreased diffusion within the prepontine cistern encasing the basilar artery . ETMR is an aggressive primitive neuroectodermal tumor with ependymoblastic rosettes occurring in young children.*

**Dysplastic Cerebellar Gangliocytoma**
*Axial T2 MR shows a large, infiltrative left cerebellar hemispheric mass with characteristic tigroid pattern from retained cerebellar folia architecture . This is classic for dysplastic cerebellar gangliocytoma (Lhermitte-Duclos), which is a benign hamartoma.*
### Additional Images
**Pilocytic Astrocytoma**
*Sagittal T1 C+ FS MR shows a pilocytic astrocytoma involving the cerebellum with heterogeneous enhancement and a large cyst . Note the effacement of the 4th ventricle rather than expansion, which would be typical for medulloblastoma and ependymomas.*

**Pilocytic Astrocytoma**
*Sagittal T1 C+ FS MR shows a pilocytic astrocytoma involving the cerebellum with heterogeneous enhancement and a large cyst . Note the effacement of the 4th ventricle rather than expansion, which would be typical for medulloblastoma and ependymomas.*

**Pilocytic Astrocytoma**
*Axial T2 FS MR shows a T2-hyperintense solid mass filling the 4th ventricle. Postcontrast enhancement was seen (not shown), consistent with pilocytic astrocytoma. Low-grade tumors typically have a T2-hyperintense signal of the tumor parenchyma.*

**Medulloblastoma**
*Axial T1 C+ FS MR shows a heterogeneously enhancing mass filling the 4th ventricle. This was a group 1 medulloblastoma with Wingless (WNT) activation. These are rare medulloblastomas, but they have a very good prognosis. They are typically seen near the cerebellopontine angle in older children.*

**Medulloblastoma**
*Axial DWI MR shows areas of decreased diffusion in this WNT pathway medulloblastoma. Decreased diffusion is typical for all medulloblastomas and high- grade neoplasms.*

**Medulloblastoma**
*Axial T2 MR in an infant shows an isointense nodular mass within the 4th ventricle with associated cerebellar edema . This neoplasm demonstrated intense enhancement and decreased diffusion (not shown). This neoplasm was SHH-activated, group 2 medulloblastoma classified histologically as a medulloblastoma with extensive nodularity.*

**Medulloblastoma**
*Sagittal T1 C+ MR shows nodular enhancement in this group 3 medulloblastoma, which has a poor outcome compared to other subgroups.*

**Medulloblastoma**
*Sagittal T1 C+ FS MR shows a minimally enhancing mass within the 4th ventricle . This is consistent with a group 4 medulloblastoma, which arises in the classic location but has minimal enhancement.*

**Medulloblastoma**
*Axial DWI MR shows that the intraventricular tumor has nearly uniform decreased diffusion compatible with a high-grade neoplasm. Despite minimal contrast enhancement, group 4 medulloblastomas show decreased diffusion. This most common subgroup has an intermediate prognosis.*

**Ependymoma**
*Axial T2 FS MR shows a T2 iso- to hyperintense mass filling the 4th ventricle but extending through the foramina inferiorly, particularly the right foramen of Luschka . This is a typical appearance for a posterior fossa ependymoma.*

**Brainstem Glioma, Pediatric**
*Sagittal T1 MR shows a mass involving the tectal plate, which is consistent with a tectal plate glioma . Pedunculated brainstem gliomas typically are low grade with good prognosis.*

**Diffuse Intrinsic Pontine Glioma**
*Axial FLAIR MR shows a hyperintense mass diffusely expanding the pons and encasing the basilar artery . Unlike pedunculated brain stem tumors, diffuse lesions have a poor prognosis.*

**Diffuse Intrinsic Pontine Glioma**
*Axial T1 C+ FS MR shows minimal asymmetric enhancement of the diffuse pontine mass and effacement of the 4th ventricle . With near 100% mortality, these tumors have been associated with H3-K27M mutations, which also contribute to diffuse midline gliomas in the thalamus and spinal cord.*

**Ganglioglioma**
*Axial T2 FS MR shows a heterogeneous, irregular mass in the left brachium pontis with cystic change and areas of hemorrhage . This was a ganglioglioma at resection.*

**Ganglioglioma**
*Axial T1 C+ FS MR shows that the left middle cerebellar peduncle mass has irregular amorphous contrast enhancement. Note the involvement at the origin of the VII and VIII cranial nerves . This child presented with left sensorineural hearing loss and facial weakness.*

**Schwannoma**
*Axial T1 C+ MR shows an intensely enhancing extraaxial mass displacing the cerebellum & medulla arising below the cerebellopontine angle with extension through the left jugular foramen . There is central cystic nonenhancement , typical for large schwannomas.*

**Meningioma, CPA-IAC**
*Axial T1 C+ MR shows a homogeneous enhancing mass with a broad dural attachment along posterior dura, consistent with meningioma. Schwannomas & meningiomas are rare in children, and neurofibromatosis type 2 should be considered.*

**Hemangioblastoma**
*Sagittal T1 C+ MR shows a cystic mass involving the medulla and upper cervical cord. There are small nodules of enhancement along the rim of the cyst , consistent with hemangioblastoma in a child with von Hippel-Lindau disease.*

**Choroid Plexus Papilloma**
*Axial NECT shows a heavily calcified mass arising from the inferior 4th ventricle and extending into the cisterna magna with dilated temporal horns from obstructive hydrocephalus.*

**Choroid Plexus Papilloma**
*Axial T1 C+ MR shows a lobular enhancing mass at the left cerebellopontine angle without extension into the internal auditory canal. This is a rare location for a choroid plexus papilloma.*

**Anaplastic Astrocytoma**
*Axial T2 FS MR shows a poorly circumscribed infiltrative mass in the left pons, cerebellar peduncle, and deep white matter of the right cerebellum. No significant enhancement with areas of decreased diffusion was seen (not shown). This was a biopsy-proven anaplastic astrocytoma.*

**Atypical Teratoid-Rhabdoid Tumor**
*Axial T2 MR shows a heterogeneous mass with prominent cysts in the 4th ventricle. The solid component of tumor is iso- to hypointense on T2 & is consistent with high-grade neoplasm such as atypical teratoid-rhabdoid tumor (ATRT).*

**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T1 C+ MR shows heterogeneous enhancement of the 4th ventricle with a prominent cyst . Although not exclusive, ATRT tends to have more cystic change than medulloblastoma and other high-grade neoplasms. This tumor also had decreased diffusion (not shown).*

**Medulloblastoma Variants**
*Axial T2 MR shows an isointense mass within the 4th ventricle as well as a nodule in the right cerebellar hemisphere . Involvement of the cerebellar hemisphere in a medulloblastoma is suggestive of group 2 SHH-activation, which is histologically described as desmoplastic or extensive nodularity.*

**Medulloepithelioma**
*Axial DWI MR shows decreased diffusion in this medulloepithelioma involving the pons and right brachium pontis. These tumors are highly malignant and may have metastases to extracranial locations.*

**Embryonal Tumor With Multilayered Rosettes**
*Axial DWI MR shows a tumor with decreased diffusion within the prepontine cistern encasing the basilar artery . ETMR is an aggressive primitive neuroectodermal tumor with ependymoblastic rosettes occurring in young children.*

**Dysplastic Cerebellar Gangliocytoma**
*Axial T2 MR shows a large, infiltrative left cerebellar hemispheric mass with characteristic tigroid pattern from retained cerebellar folia architecture . This is classic for dysplastic cerebellar gangliocytoma (Lhermitte-Duclos), which is a benign hamartoma.*
### Additional Images
 .](9e9bf0be-b52d-4c57-a76c-f9055da091e5)
**Medulloblastoma Variants**
*Axial T2 MR in a 10 month old shows a large mass with a lobular, expanded gyriform configuration .*

**Medulloblastoma Variants**
*Coronal T1 C+ MR in a 10 month old shows distinct grape-like lobular enhancement , characteristic of medulloblastoma but with extensive nodularity, a medulloblastoma variant with neuronal differentiation and a somewhat better prognosis.*

**Medulloblastoma Variants**
*Axial T2 MR shows a predominately solid lateral cerebellar mass with scattered hyperintense foci .*

**Medulloblastoma Variants**
*Coronal T1 C+ MR in the same patient shows that the mass enhances quite heterogeneously. A desmoplastic variant of the medulloblastoma was found at surgery.*

**Medulloblastoma Variants**
*Axial T2 MR in a 2 1/2 year old with 1 month of vomiting and headache shows a large heterogeneous midline mass dorsal to, and displacing the 4th ventricle anteriorly. The mass is minimally hyperintense compared to gray matter.*

**Medulloblastoma Variants**
*Axial T1 C+ FS MR in the same patient shows inhomogeneous enhancement. Histopathology was a desmoplastic variant of medulloblastoma, WHO grade IV.*
**Pilocytic Astrocytoma**
*Sagittal T1 C+ MR shows a typical tumor cyst with an enhancing mural nodule . There is hydrocephalus and protrusion of the cerebellar tonsils through the foramen magnum (acquired Chiari type 1).*

**Pilocytic Astrocytoma**
*Axial T2 MR shows an increased signal of the solid component of the mass. Interstitial edema is present in the temporal lobes.*

**Medulloblastoma**
*Sagittal T2 MR shows a hyperintense mass filling and expanding the 4th ventricle. The tumor does not extend through the 4th ventricular outlet foramina. There is hydrocephalus with acquired tonsillar herniation .*

**Medulloblastoma**
*Coronal T1 C+ MR shows heterogeneous enhancement of the 4th ventricular primitive neuroectodermal tumor/medulloblastoma*

**Ependymoma**
*Sagittal T1 MR shows a large tumor filling the 4th ventricle and extruding through the obex into the upper spinal canal.*

**Medulloblastoma Variants**
*Axial T2 MR in a 10 month old shows a large mass with a lobular, expanded gyriform configuration .*

**Medulloblastoma Variants**
*Coronal T1 C+ MR in a 10 month old shows distinct grape-like lobular enhancement , characteristic of medulloblastoma but with extensive nodularity, a medulloblastoma variant with neuronal differentiation and a somewhat better prognosis.*

**Medulloblastoma Variants**
*Axial T2 MR shows a predominately solid lateral cerebellar mass with scattered hyperintense foci .*

**Medulloblastoma Variants**
*Coronal T1 C+ MR in the same patient shows that the mass enhances quite heterogeneously. A desmoplastic variant of the medulloblastoma was found at surgery.*

**Medulloblastoma Variants**
*Axial T2 MR in a 2 1/2 year old with 1 month of vomiting and headache shows a large heterogeneous midline mass dorsal to, and displacing the 4th ventricle anteriorly. The mass is minimally hyperintense compared to gray matter.*

**Medulloblastoma Variants**
*Axial T1 C+ FS MR in the same patient shows inhomogeneous enhancement. Histopathology was a desmoplastic variant of medulloblastoma, WHO grade IV.*

**Pilocytic Astrocytoma**
*Sagittal T1 C+ MR shows a typical tumor cyst with an enhancing mural nodule . There is hydrocephalus and protrusion of the cerebellar tonsils through the foramen magnum (acquired Chiari type 1).*

**Pilocytic Astrocytoma**
*Axial T2 MR shows an increased signal of the solid component of the mass. Interstitial edema is present in the temporal lobes.*

**Medulloblastoma**
*Sagittal T2 MR shows a hyperintense mass filling and expanding the 4th ventricle. The tumor does not extend through the 4th ventricular outlet foramina. There is hydrocephalus with acquired tonsillar herniation .*

**Medulloblastoma**
*Coronal T1 C+ MR shows heterogeneous enhancement of the 4th ventricular primitive neuroectodermal tumor/medulloblastoma*

**Ependymoma**
*Sagittal T1 MR shows a large tumor filling the 4th ventricle and extruding through the obex into the upper spinal canal.*
 within the tumor.](22435260-8309-4d13-8e4c-53762c58bc3a)
**Ependymoma**
*Axial T2 MR shows a heterogeneous tumor expanding and extruding through the right foramen of Luschka . There are a few coarse calcific foci within the tumor.*

**Ependymoma**
*Axial T2 MR shows a heterogeneous tumor expanding and extruding through the right foramen of Luschka . There are a few coarse calcific foci within the tumor.*
 is bulbous and slightly increased in signal intensity. The aqueduct of Sylvius is obstructed
is bulbous and slightly increased in signal intensity. The aqueduct of Sylvius is obstructed  .](a1b37154-b363-4f92-b3d9-2ea2193ddd51)
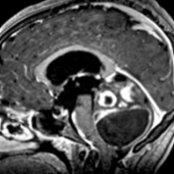
**Brainstem Glioma, Pediatric**
*Sagittal T2 MR in an infant with a tectal plate glioma shows marked hydrocephalus involving the 3rd and lateral ventricles. The corpus callosum is stretched thin . The tectal plate is bulbous and slightly increased in signal intensity. The aqueduct of Sylvius is obstructed .*

**Brainstem Glioma, Pediatric**
*Sagittal T2 MR in this child with a diffusely infiltrating pontine glioma shows homogeneous signal intensity of the expanded pons .*

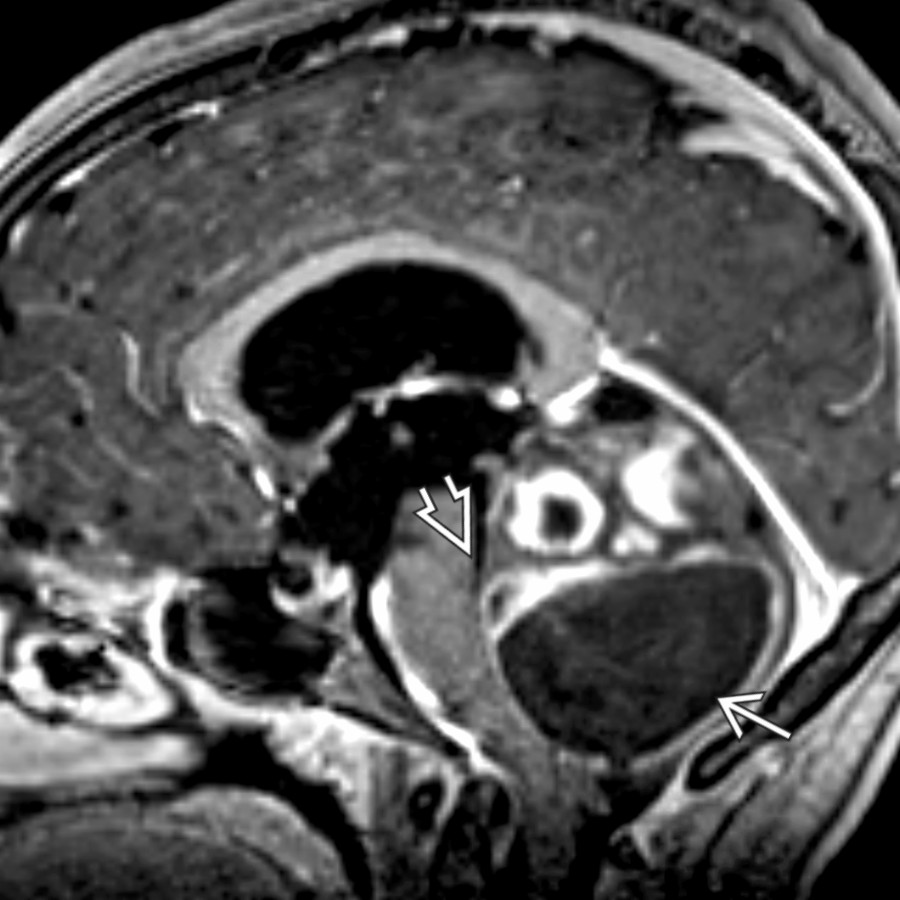
**Brainstem Glioma, Pediatric**
*Sagittal T1 C+ MR shows marked expansion of the medulla by a complex mass with intralesional cystic areas and avid, but heterogeneous, enhancement in this child with dorsal exophytic brainstem glioma. The inferior 4th ventricle is deformed by the protruding mass.*

**Ganglioglioma**
*Sagittal T2 MR shows marked expansion of the medulla and upper cervical spinal cord . The inferior 4th ventricle is deformed by the dorsally protruding mass.*

**Schwannoma**
*Axial T2 MR shows a bulky heterogeneous right cerebellopontine angle mass , which crosses the midline. There is also extensive remodeling of the right internal auditory canal by this schwannoma.*

**Schwannoma**
*Axial T1 C+ MR in another child shows small bilateral vestibular schwannomas. The right lesion assumes the appearance of an ice cream on a cone. Both demonstrate intralabyrinthine extension .*

**Meningioma, CPA-IAC**
*Axial T2 MR shows a low-signal, lobular cerebellopontine angle mass with hyperostosis of the adjacent petrous apex. There is mild rotation of the medulla due to mass effect.*

**Meningioma, CPA-IAC**
*Coronal NECT shows diffuse hyperostosis adjacent to the meningioma .*

**Hemangioblastoma**
*Sagittal T2 MR shows a solid component with multiple flow voids , a cyst , and edema of the medulla and upper cervical cord .*

**Hemangioblastoma**
*Sagittal T1 C+ MR of the same patient shows the cyst to better advantage. Here, the cyst's contents have slightly increased the signal.*

**Anaplastic Astrocytoma**
*Axial T2 MR shows multiple foci of abnormal signal intensity in the peripheral right cerebellar hemisphere and in the cerebellar white matter adjacent to the lateral recess of the 4th ventricle.*

**Anaplastic Astrocytoma**
*Axial T1 C+ MR shows enhancement following gadolinium administration. The lesion adjacent to the 4th ventricle lateral recess has ill-defined margins.*

**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T2 MR shows extensive posterior fossa , pineal region , and intraventricular low-signal intensity masses. Multifocal deposits of tumor at diagnosis are strongly suggestive of an atypical teratoid-rhabdoid tumor.*

**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T1 C+ MR shows quite variable enhancement of the posterior fossa , pineal region , and intraventricular tumor deposits. There is marked hydrocephalus.*

**Choroid Plexus Carcinoma**
*Axial T1 C+ MR shows a slightly heterogeneous but avidly enhancing mass within the right foramen of Luschka . There is an associated cyst .*

**Choroid Plexus Carcinoma**
*Axial T2 MR in a different child undergoing treatment for choroid plexus carcinoma shows a large skull base metastatic deposit .*

**Medulloepithelioma**
*Axial NECT in a 1-day-old infant shows a dense, lobular mass filling the posterior fossa. Foci of increased density superimposed in the mass are due to hemorrhage. Note the blood-CSF level in the dilated infundibular recess .*

**Medulloepithelioma**
*Coronal T1 C+ MR in the same infant following biopsy shows extension into the spinal canal . Gas in the ventricular system follows neurosurgical intervention. There is extensive ependymal seeding .*

**Dysplastic Cerebellar Gangliocytoma**
*Axial T1 C+ MR shows a large nonenhancing mass involving the left cerebellar hemisphere. Preservation of the cerebellar folia pattern, or striated cerebellum , is characteristic for dysplastic cerebellar gangliocytoma (Lhermitte-Duclos). This disease has a strong association with Cowden syndrome.*
.](a1b37154-b363-4f92-b3d9-2ea2193ddd51)
**Brainstem Glioma, Pediatric**
*Sagittal T2 MR in an infant with a tectal plate glioma shows marked hydrocephalus involving the 3rd and lateral ventricles. The corpus callosum is stretched thin . The tectal plate is bulbous and slightly increased in signal intensity. The aqueduct of Sylvius is obstructed .*

**Brainstem Glioma, Pediatric**
*Sagittal T2 MR in this child with a diffusely infiltrating pontine glioma shows homogeneous signal intensity of the expanded pons .*

**Brainstem Glioma, Pediatric**
*Sagittal T1 C+ MR shows marked expansion of the medulla by a complex mass with intralesional cystic areas and avid, but heterogeneous, enhancement in this child with dorsal exophytic brainstem glioma. The inferior 4th ventricle is deformed by the protruding mass.*

**Ganglioglioma**
*Sagittal T2 MR shows marked expansion of the medulla and upper cervical spinal cord . The inferior 4th ventricle is deformed by the dorsally protruding mass.*

**Schwannoma**
*Axial T2 MR shows a bulky heterogeneous right cerebellopontine angle mass , which crosses the midline. There is also extensive remodeling of the right internal auditory canal by this schwannoma.*

**Schwannoma**
*Axial T1 C+ MR in another child shows small bilateral vestibular schwannomas. The right lesion assumes the appearance of an ice cream on a cone. Both demonstrate intralabyrinthine extension .*

**Meningioma, CPA-IAC**
*Axial T2 MR shows a low-signal, lobular cerebellopontine angle mass with hyperostosis of the adjacent petrous apex. There is mild rotation of the medulla due to mass effect.*

**Meningioma, CPA-IAC**
*Coronal NECT shows diffuse hyperostosis adjacent to the meningioma .*

**Hemangioblastoma**
*Sagittal T2 MR shows a solid component with multiple flow voids , a cyst , and edema of the medulla and upper cervical cord .*

**Hemangioblastoma**
*Sagittal T1 C+ MR of the same patient shows the cyst to better advantage. Here, the cyst's contents have slightly increased the signal.*

**Anaplastic Astrocytoma**
*Axial T2 MR shows multiple foci of abnormal signal intensity in the peripheral right cerebellar hemisphere and in the cerebellar white matter adjacent to the lateral recess of the 4th ventricle.*

**Anaplastic Astrocytoma**
*Axial T1 C+ MR shows enhancement following gadolinium administration. The lesion adjacent to the 4th ventricle lateral recess has ill-defined margins.*

**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T2 MR shows extensive posterior fossa , pineal region , and intraventricular low-signal intensity masses. Multifocal deposits of tumor at diagnosis are strongly suggestive of an atypical teratoid-rhabdoid tumor.*

**Atypical Teratoid-Rhabdoid Tumor**
*Sagittal T1 C+ MR shows quite variable enhancement of the posterior fossa , pineal region , and intraventricular tumor deposits. There is marked hydrocephalus.*

**Choroid Plexus Carcinoma**
*Axial T1 C+ MR shows a slightly heterogeneous but avidly enhancing mass within the right foramen of Luschka . There is an associated cyst .*

**Choroid Plexus Carcinoma**
*Axial T2 MR in a different child undergoing treatment for choroid plexus carcinoma shows a large skull base metastatic deposit .*

**Medulloepithelioma**
*Axial NECT in a 1-day-old infant shows a dense, lobular mass filling the posterior fossa. Foci of increased density superimposed in the mass are due to hemorrhage. Note the blood-CSF level in the dilated infundibular recess .*

**Medulloepithelioma**
*Coronal T1 C+ MR in the same infant following biopsy shows extension into the spinal canal . Gas in the ventricular system follows neurosurgical intervention. There is extensive ependymal seeding .*

**Dysplastic Cerebellar Gangliocytoma**
*Axial T1 C+ MR shows a large nonenhancing mass involving the left cerebellar hemisphere. Preservation of the cerebellar folia pattern, or striated cerebellum , is characteristic for dysplastic cerebellar gangliocytoma (Lhermitte-Duclos). This disease has a strong association with Cowden syndrome.*