---
title: "Progressive Supranuclear Palsy"
docid: "840ed321-c0ab-4069-a07e-ad416232f916"
authors:
- key: "1fa14dfd-71ea-4960-908e-e720313bc63a"
value: "Santhosh Gaddikeri, MD"
- key: "a25c450b-3d34-4f64-bba3-cc0834813df6"
value: "Miral D. Jhaveri, MD, MBA"
breadcrumbs:
-
name: "Brain"
slug: "brain"
treeNodeId: "6d8829f1-14d7-45af-8675-255189aa526a"
-
name: "Diagnosis"
slug: "diagnosis"
treeNodeId: "51c00394-446e-4a38-94af-d3b1d14d34e8"
-
name: "Pathology-Based Diagnoses"
slug: "pathology-based-diagnoses"
treeNodeId: "d9d3a8ed-f21b-4831-8c77-591a3500ef77"
-
name: "Acquired Toxic/Metabolic/Degenerative Disorders"
slug: "acquired-toxicmetabolicdegenerativ-"
treeNodeId: "ba3cfeaf-64d9-4117-91e8-d2ce58783fc5"
-
name: "Dementias and Degenerative Disorders"
slug: "dementias-and-degenerative-disorde-"
treeNodeId: "6381104d-7a4c-4be5-bb19-3cd90837d547"
-
name: "Progressive Supranuclear Palsy"
slug: "progressive-supranuclear-palsy"
treeNodeId: null
category: "Brain"
cmeTopicId: "8cea7de9-b88c-4f6f-b68f-28b6d8211a0d"
documentVersionId: "a7220f81-7488-458f-8ea9-a772c9889b66"
imageCount: 19
lastUpdated: "08/07/20"
pageDescription: "Progressive Supranuclear Palsy"
pageKeywords: "Brain, Diagnosis, Pathology-Based Diagnoses, Acquired Toxic/Metabolic/Degenerative Disorders, Dementias and Degenerative Disorders, Progressive Supranuclear Palsy"
pageTitle: "Progressive Supranuclear Palsy | STATdx"
enhancedTitle: "Progressive Supranuclear Palsy"
type: "DX"
references: true
breadcrumbs:
- "Brain"
- "Diagnosis"
- "Pathology-Based Diagnoses"
- "Acquired Toxic/Metabolic/Degenerative Disorders"
- "Dementias and Degenerative Disorders"
- "Progressive Supranuclear Palsy"
---
# KEY FACTS
- ## Terminology
- Neurodegenerative disease characterized by vertical supranuclear gaze palsy, postural instability, mild dementia
- ## Imaging
- Midbrain atrophy (penguin or hummingbird sign)
- Sagittal T1WI shows concave/flat upper border of midbrain (normally convex)
- Axial T1WIs show abnormal concavity of lateral margins of midbrain tegmentum (morning glory or Mickey Mouse sign)
- Thinning of superior colliculus
- Midsagittal 3D-MPRAGE or FSPGR images
- Voxel-based morphometry used to calculate ratio of midbrain area:pons area
- Midbrain area < 70 mm² (50% of normal)
- Midbrain:pons ratio < 0.15 strongly suggests PSP
- MR parkinsonism index: Allows discrimination of PSP from MSA-P, PD, and control
- New MRPI 2.0 more powerful than MRPI for differentiating PSP from PD
- ## Top Differential Diagnoses
- Multiple system atrophy, parkinsonian type
- Corticobasal degeneration
- Dementia with Lewy bodies
- Parkinson disease
- ## Pathology
- Neurofibrillary tangles and neuropil threads in globus pallidus, subthalamic nucleus, substantia nigra; cerebral cortex relatively preserved except for perirolandic cortex
- Neuronal loss, tufted astrocytes (hallmark of PSP), and coiled bodies of oligodendrocyte
- ## Clinical Issues
- PSP-RS (Richardson syndrome)
- Lurching gait, axial dystonia, vertical supranuclear palsy
- PSP-P (parkinsonian type)
- Bradykinesia, rigidity, normal eye movements
- 2nd most common neurodegenerative cause of parkinsonism overall
# TERMINOLOGY
- ## Abbreviations
- Progressive supranuclear palsy (PSP)
- ## Synonyms
- Steele-Richardson-Olszewski syndrome
- ## Definitions
- Atypical parkinsonian syndrome and neurodegenerative disease characterized by vertical supranuclear gaze palsy, postural instability with unexplained falls, akinesia, and cognitive dysfunction
# IMAGING
- ## General Features
- ### Best diagnostic clue
- Midbrain tegmentum atrophy (penguin or hummingbird sign)
- Most accurate: Calculation of midbrain area:pons area ratio
- Distinguishes PSP from other conditions
- PSP vs. parkinsonian form of multisystem atrophy (MSA-P)
- ### Location
- Midbrain
- Tegmentum
- Tectum (superior colliculus)
- ### Morphology
- Prominent midbrain volume loss
- Pons normal
- ## Imaging Recommendations
- ### Best imaging tool
- MR
- PET
- ### Protocol advice
- Midsagittal T1WI
- 3D MPRAGE or FSPGR images
- Use voxel-based morphometry to calculate ratio of midbrain area:pons area
- ## CT Findings
- ### NECT
- Atrophy of midbrain with prominent mesencephalic cisterns and enlarged 3rd ventricle
- ## MR Findings
- ### T1WI
- Sagittal T1WI helpful in detecting midbrain tectal atrophy (penguin or hummingbird sign)
- Concave or flat profile of cephalad surface of midbrain (as opposed to normal convex superior profile)
- Thinning of superior colliculus
- Axial T1WIs show abnormal concavity of lateral margins of midbrain tegmentum (morning glory or Mickey Mouse sign)
- Superior cerebellar peduncle atrophy (correlates with disease duration)
- Midbrain area ~ 1/2 that of normal individuals
- Ratio of midbrain area:pons area in PSP (0.124) was significantly smaller than in Parkinson disease (PD) (0.208), MSA-P (0.266), and normal control (0.237)
- Sagittal midbrain area < 70 mm², ratio of midbrain tegmentum:pons area < 0.15 → diagnostic of PSP
- Sensitivity: 100%; specificity: 91-100%
- MR parkinsonism index (MRPI) = (pons area/midbrain area x middle cerebellar peduncle width/superior cerebellar peduncle width)
- Allows discrimination of patients with PSP from MSA-P, PD, and control with 100% sensitivity, 100% specificity, and 100% PPV
- MRPI 2.0
- MRPI 2.0 = MRPI x (3rd ventricle width/frontal horns width)
- Higher sensitivity (100%) and similar specificity (94.3%) of MRPI 2.0 in differentiating patients with PSP-P from those with PD when compared to previous MRPI (sensitivity and specificity of 73.5% and 98.1%, respectively)
- More powerful than MRPI in differentiating PSP patients in early stage of disease with slowness of vertical saccades from patients with PD
- Help clinicians to consolidate diagnosis based on clinical features
- AP midbrain diameter < 17 mm
- ### T2WI
- ↓ AP diameter of midbrain on axial T2WI < 17 mm, 75% positive predictive value in differentiating PSP from MSA
- Hyperintense signal in midbrain tegmentum = periaqueductal
- Prominent mesencephalic cisterns and enlarged 3rd ventricle
- Occasionally abnormal hypointense signal in striatum
- ### DWI
- ↑ ADC in putamen might discriminate PSP from PD
- ↑ ADC in decussation of superior cerebellar peduncles
- DTI
- ↑ mean diffusivity in decussation of superior cerebellar peduncle
- DTI indices (fractional anisotropy, mean diffusivity) demonstrate widespread white matter abnormalities
- ↑ mean diffusivity in midbrain of PSP patients compared with PD and MSA
- ## Nuclear Medicine Findings
- ### PET
- 18 F-FDG ↓ in putamen, thalamus, medial frontal cortex, and midbrain
- 11C-raclopride PET ↓ striatal dopamine receptor binding
- Fluorodopa-PET: Reduction of F-dopa uptake in caudate, putamen (more severe than in PD)
- SPECT
- I-123-IBZM SPECT: Reduced dopamine receptor binding in striatum
# DIFFERENTIAL DIAGNOSIS
- [Multiple System Atrophy, Parkinsonian Type](/document/multiple-system-atrophy/4fb9af00-e0bd-4164-8f61-4011ddc8bf9e)
- T2 hypointensity in putamen without prominent midbrain atrophy
- Cerebellar and pontine atrophy
- Prominent cerebellar symptoms, autonomic dysfunction, parkinsonism
- [Corticobasal Degeneration](/document/corticobasal-degeneration/23f97d4e-8724-4229-b9f8-08f63906ebd8)
- Severe frontoparietal atrophy in asymmetric pattern
- Unilateral parkinsonism
- "Alien limb" phenomenon, cortical sensory deficit
- [Dementia With Lewy Bodies](/document/dementia-with-lewy-bodies/e8e46d1d-46d2-4e5a-880f-f025a84c5871)
- Cortical atrophy without prominent midbrain atrophy
- Hallucinations, cortical dementia with aphasia, parkinsonism
- [Parkinson Disease](/document/parkinson-disease/0bc3188a-935b-416d-b1a0-25b2d52c6399)
- No prominent midbrain atrophy
- Tremor-dominant clinical symptoms, good response to levodopa
# PATHOLOGY
- ## General Features
- ### Etiology
- PSP is tauopathy
- Abnormal accumulation of phosphorylated tau protein in brain
- Pallidum, subthalamic nucleus, red nucleus, substantia nigra, pontine tegmentum, striatum, oculomotor nucleus, medulla, dentate nucleus
- ### Genetics
- Associated with tau, *MTAP* on chromosome 17
- Tau haplotype H1 associated with both PSP and corticobasal degeneration
- Suggests that gene on chromosome 17 for tau abnormality causes both diseases
- ## Gross Pathologic & Surgical Features
- Atrophy of subthalamic nucleus and brainstem (midbrain tectum and superior cerebellar peduncle)
- Loss of pigmentation in substantia nigra → nigrostriatal dopaminergic degeneration
- ## Microscopic Features
- Neuronal loss, astrocytic plaques, and tufts of abnormal fibers are highly characteristic of typical PSP
- Neurofibrillary tangles and neuropil threads in globus pallidus, subthalamic nucleus, substantia nigra; cerebral cortex relatively preserved except for perirolandic cortex
- Tau pathology is also noted in glia: Tufted astrocytes (hallmark of PSP), coiled bodies of oligodendrocyte
# CLINICAL ISSUES
- ## Presentation
- ### Most common signs/symptoms
- PSP-RS (Richardson syndrome): More common classic type
- Classic, more common presentation of lurching gait, axial dystonia, vertical supranuclear palsy
- PSP-P (parkinsonian type) 1/3 patients
- Bradykinesia, rigidity, normal eye movements, and transient response to levodopa
- Postural instability and frequent falls, oculomotor findings, cognitive and behavioral change, memory problems, sleep disturbance, apathy
- Most common cause of atypical parkinsonian syndrome
- 2nd most common neurodegenerative cause of parkinsonism overall
- Clinical criteria for "probable" PSP
- Probable PSP is diagnosed when clinical features with high specificity are present
- Gradually progressive bradykinetic/akinetic disorder
- Vertical gaze palsy and slowing of vertical saccades
- Prominent postural instability with falls in 1st year
- Cognitive dysfunction
- Sporadic occurrence, onset at age 40 or later
- No evidence for competing diagnostic possibilities
- Exclusion criteria
- Recent encephalitis, alien limb syndrome, cortical sensory defects or temporoparietal atrophy, psychosis unrelated to dopaminergic treatment, important cerebellar signs, severe asymmetric parkinsonian signs, relevant structural abnormality of basal ganglia on neuroimaging
- Severe cerebral leukoencephalopathy, relevant structural abnormality (e.g., NPH; basal ganglia, diencephalic, mesencephalic, pontine or medullary infarctions, hemorrhages, hypoxic-ischemic lesions, tumors, or malformations)
- ## Demographics
- ### Age
- Generally 45-75 years
- Peak onset: 65 years
- ### Sex
- No sex predominance
- ### Epidemiology
- Prevalence: 3-7 cases per 100,000
- ## Natural History & Prognosis
- Most common atypical parkinsonian syndrome with variable disease course
- Survival from time of symptom onset in PSP ranges from 5.3-9.7 years
- Neuropsychiatric symptoms develop > 50% patients within 2 years of disease onset
- ## Treatment
- Symptomatic
- Levodopa may help rigidity and bradykinesia of PSP
- Mitochondrial nutrient coenzyme Q10 can give modest benefit
- ## Variant PSP Syndrome
- PSP with Richardson syndrome (PSP-RS),
- PSP with predominant parkinsonism (PSP-P)
- PSP with predominant oculomotor dysfunction (PSP-OM)
- PSP with predominant postural instability (PSP-PI)
- PSP with progressive gait freezing (PSP-PGF)
- PSP with predominant frontal presentation (PSP-F)
- PSP with predominant speech/language disorder (PSP-SL)
- PSP with predominant corticobasal syndrome (PSP-CBS)
- PSP with predominant cerebellar ataxia (PSP-C)
- PSP with predominant primary lateral sclerosis (PSP-PLS)
# DIAGNOSTIC CHECKLIST
- ## Consider
- Consider PSP when MR shows marked midbrain atrophy in patients with atypical parkinsonism, vertical gaze palsy, and cognitive dysfunction
- ## Image Interpretation Pearls
- Sagittal images helpful in identifying penguin silhouette sign
- Minimal or no lobar atrophy
fff14e0c-5958-4336-93e1-26ef6cac9c30
## References
# Selected References
1. [Agarwal S et al: Progressive supranuclear palsy. StatPearls. 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=30252354%5Bpmid%5D)
1. [Eraslan C et al: MRI evaluation of progressive supranuclear palsy: differentiation from Parkinson's disease and multiple system atrophy. Neurol Res. 41(2):110-7, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30373485%5Bpmid%5D)
1. [Giagkou N et al: Progressive supranuclear palsy. Int Rev Neurobiol. 149:49-86, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=31779824%5Bpmid%5D)
1. [Grimm MJ et al: How to apply the movement disorder society criteria for diagnosis of progressive supranuclear palsy. Mov Disord. 34(8):1228-32, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30884545%5Bpmid%5D)
1. [Smith MD et al: Imaging in the diagnosis of progressive supranuclear palsy. J Neurol. 266(2):545-7, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30542948%5Bpmid%5D)
1. [Talai AS et al: Improved automatic morphology-based classification of parkinson's disease and progressive supranuclear palsy. Clin Neuroradiol. 29(4):605-14, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30218110%5Bpmid%5D)
1. [Krismer F et al: Diagnosis of PSP-P: can a newly developed MRPI make the difference? Parkinsonism Relat Disord. 54:1-2, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=30236828%5Bpmid%5D)
1. [Quattrone A et al: A new MR imaging index for differentiation of progressive supranuclear palsy-parkinsonism from Parkinson's disease. Parkinsonism Relat Disord. 54:3-8, 2018](http://www.ncbi.nlm.nih.gov/pubmed/?term=30068492%5Bpmid%5D)
1. [Booth TC et al: The role of functional dopamine-transporter SPECT imaging in parkinsonian syndromes, part 1. AJNR Am J Neuroradiol. 36(2):229-35, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=24904053%5Bpmid%5D)
1. [Booth TC et al: The role of functional dopamine-transporter SPECT imaging in parkinsonian syndromes, part 2. AJNR Am J Neuroradiol. 36(2):236-44, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=24924549%5Bpmid%5D)
1. [Josephs KA: Key emerging issues in progressive supranuclear palsy and corticobasal degeneration. J Neurol. 262(3):783-8, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=25701010%5Bpmid%5D)
1. [Broski SM et al: Structural and functional imaging in parkinsonian syndromes. Radiographics. 34(5):1273-92, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=25208280%5Bpmid%5D)
1. [Colosimo C et al: Fifty years of progressive supranuclear palsy. J Neurol Neurosurg Psychiatry. 85(8):938-44, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24013274%5Bpmid%5D)
1. [Golbe LI: Progressive supranuclear palsy. Semin Neurol. 34(2):151-9, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24963674%5Bpmid%5D)
1. [Stamelou M et al: Atypical parkinsonism: an update. Curr Opin Neurol. 26(4):401-5, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=23812308%5Bpmid%5D)
1. [Williams DR et al: Parkinsonian syndromes. Continuum (Minneap Minn). 19(5 Movement Disorders):1189-212, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=24092286%5Bpmid%5D)
1. [Williams DR et al: Progressive supranuclear palsy: clinicopathological concepts and diagnostic challenges. Lancet Neurol. 8(3):270-9, 2009](http://www.ncbi.nlm.nih.gov/pubmed/?term=19233037%5Bpmid%5D)
1. [Quattrone A et al: MR imaging index for differentiation of progressive supranuclear palsy from Parkinson disease and the Parkinson variant of multiple system atrophy. Radiology. 246(1):214-21, 2008](http://www.ncbi.nlm.nih.gov/pubmed/?term=17991785%5Bpmid%5D)
1. [Rizzo G et al: Diffusion-weighted brain imaging study of patients with clinical diagnosis of corticobasal degeneration, progressive supranuclear palsy and Parkinson's disease. Brain. 131(Pt 10):2690-700, 2008](http://www.ncbi.nlm.nih.gov/pubmed/?term=18819991%5Bpmid%5D)
1. [Oba H et al: New and reliable MRI diagnosis for progressive supranuclear palsy. Neurology. 64(12):2050-5, 2005](http://www.ncbi.nlm.nih.gov/pubmed/?term=15985570%5Bpmid%5D)
1. [Adachi M et al: Morning glory sign: a particular MR finding in progressive supranuclear palsy. Magn Reson Med Sci. 3(3):125-32, 2004](http://www.ncbi.nlm.nih.gov/pubmed/?term=16093629%5Bpmid%5D)
1. [Righini A et al: MR imaging of the superior profile of the midbrain: differential diagnosis between progressive supranuclear palsy and Parkinson disease. AJNR Am J Neuroradiol. 25(6):927-32, 2004](http://www.ncbi.nlm.nih.gov/pubmed/?term=15205125%5Bpmid%5D)
## Images
### Selected Images
 (penguin or hummingbird sign) and atrophy of the superior colliculus
(penguin or hummingbird sign) and atrophy of the superior colliculus  is shown.](images/app.statdx.com_image_thumbnail_92756026-0a08-4a23-b04a-da6f4a40d18e_size_168_quality_85_052df857_20251014T204728Z.jpg)
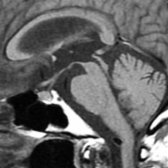
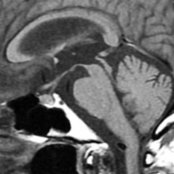
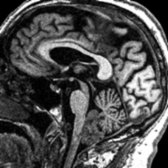
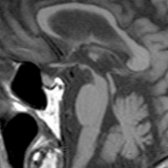
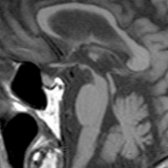
*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*
*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*
*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*
*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*
*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*
*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*
*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*

*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*

*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*

*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*

*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*

*Midline sagittal T1WI of 65-year-old man with progressive supranuclear palsy shows asymmetric atrophy of the midbrain. Slight concave appearance of the superior surface of the midbrain (penguin or hummingbird sign) and atrophy of the superior colliculus is shown.*
 (morning glory or Mickey Mouse sign) due to atrophy.](images/app.statdx.com_image_thumbnail_6565b1b3-3f60-4cad-b595-4dca64fe7b05_size_168_quality_85_704457b5_20251014T204728Z.jpg)
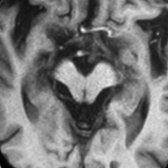
*Axial T1WI in the same patient shows concave appearance of lateral surface of midbrain (morning glory or Mickey Mouse sign) due to atrophy.*
*Axial T1WI in the same patient shows concave appearance of lateral surface of midbrain (morning glory or Mickey Mouse sign) due to atrophy.*
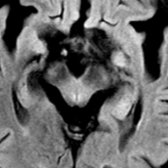
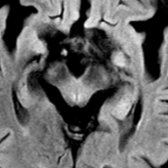
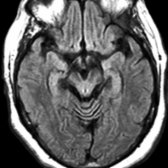
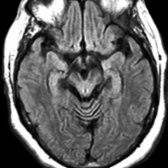
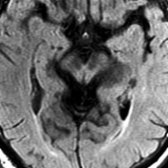
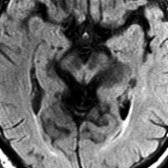
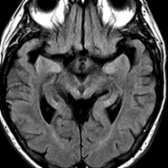
*Axial FLAIR in same patient shows subtle periaqueductal hyperintense signal . Note decreased AP diameter of the midbrain due to atrophy. AP diameter < 17 mm has 75% positive predictive value in differentiating progressive supranuclear palsy from multisystem atrophy.*
*Axial FLAIR in same patient shows subtle periaqueductal hyperintense signal . Note decreased AP diameter of the midbrain due to atrophy. AP diameter < 17 mm has 75% positive predictive value in differentiating progressive supranuclear palsy from multisystem atrophy.*
*Axial T1WI in the same patient shows concave appearance of lateral surface of midbrain (morning glory or Mickey Mouse sign) due to atrophy.*

*Axial T1WI in the same patient shows concave appearance of lateral surface of midbrain (morning glory or Mickey Mouse sign) due to atrophy.*

*Axial FLAIR in same patient shows subtle periaqueductal hyperintense signal . Note decreased AP diameter of the midbrain due to atrophy. AP diameter < 17 mm has 75% positive predictive value in differentiating progressive supranuclear palsy from multisystem atrophy.*

*Axial FLAIR in same patient shows subtle periaqueductal hyperintense signal . Note decreased AP diameter of the midbrain due to atrophy. AP diameter < 17 mm has 75% positive predictive value in differentiating progressive supranuclear palsy from multisystem atrophy.*
 , and midbrain .](images/app.statdx.com_image_thumbnail_8452163c-579f-4684-8e69-a6da03d45918_size_168_quality_85_85ffb8a6_20251014T204728Z.jpg)
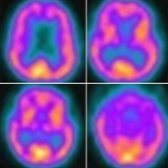
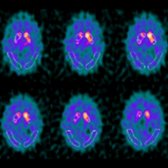
*Axial reformatted FDG PET in the same patient shows diffuse decreased metabolic activity in bilateral frontal lobes , striata (right > > left) , thalami , and midbrain .*
*Axial reformatted FDG PET in the same patient shows diffuse decreased metabolic activity in bilateral frontal lobes , striata (right > > left) , thalami , and midbrain .*
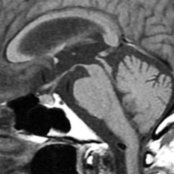
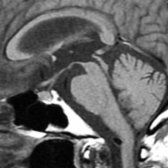
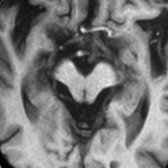
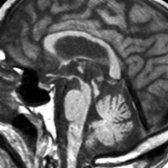
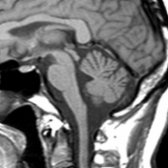
*Midline sagittal T1WI in a 67-year-old woman with extrapyramidal symptoms, vertical superior gaze palsy, and gait instability due to progressive supranuclear palsy shows flat surface profile of the cephalad surface of midbrain (hummingbird or penguin sign) .*

*Midline sagittal T1WI in a 67-year-old woman with extrapyramidal symptoms, vertical superior gaze palsy, and gait instability due to progressive supranuclear palsy shows flat surface profile of the cephalad surface of midbrain (hummingbird or penguin sign) .*
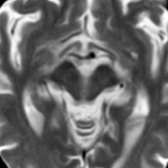
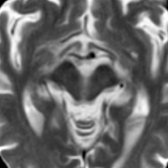
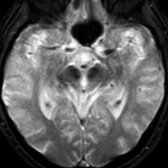
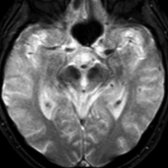
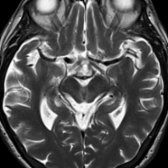
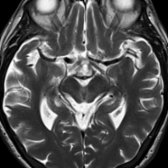
*Axial T2 MR in the same patient shows abnormal concavity of the lateral margin of midbrain tegmentum referred to as the morning glory or Mickey Mouse sign.*
*Axial T2 MR in the same patient shows abnormal concavity of the lateral margin of midbrain tegmentum referred to as the morning glory or Mickey Mouse sign.*
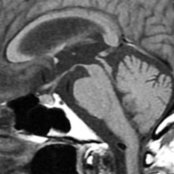
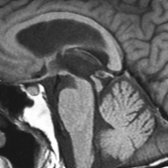
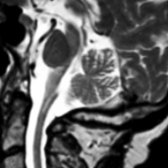
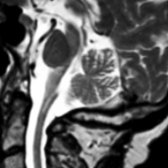
*Sagittal T1WI MR (3D MPRAGE) in an 80-year-old woman with PSP shows striking midbrain volume loss, with the penguin or hummingbird sign manifested by a concave upper border of the midbrain . Note extreme thinning of the tectal plate . An incidental subependymoma was found.*

*Sagittal T1WI MR (3D MPRAGE) in an 80-year-old woman with PSP shows striking midbrain volume loss, with the penguin or hummingbird sign manifested by a concave upper border of the midbrain . Note extreme thinning of the tectal plate . An incidental subependymoma was found.*
*Axial FLAIR MR in the same patient shows the tectal plate is extremely thin , the lateral aspects of the midbrain are concave (morning glory sign), and the cerebral peduncles are atrophic.*
*Axial FLAIR MR in the same patient shows the tectal plate is extremely thin , the lateral aspects of the midbrain are concave (morning glory sign), and the cerebral peduncles are atrophic.*
*Sagittal T2WI MR in a patient with PSP shows diminished midbrain volume and thinned tectum .*
*Sagittal T2WI MR in a patient with PSP shows diminished midbrain volume and thinned tectum .*
*Axial reformatted FDG PET in the same patient shows diffuse decreased metabolic activity in bilateral frontal lobes , striata (right > > left) , thalami , and midbrain .*

*Axial reformatted FDG PET in the same patient shows diffuse decreased metabolic activity in bilateral frontal lobes , striata (right > > left) , thalami , and midbrain .*

*Midline sagittal T1WI in a 67-year-old woman with extrapyramidal symptoms, vertical superior gaze palsy, and gait instability due to progressive supranuclear palsy shows flat surface profile of the cephalad surface of midbrain (hummingbird or penguin sign) .*

*Midline sagittal T1WI in a 67-year-old woman with extrapyramidal symptoms, vertical superior gaze palsy, and gait instability due to progressive supranuclear palsy shows flat surface profile of the cephalad surface of midbrain (hummingbird or penguin sign) .*

*Axial T2 MR in the same patient shows abnormal concavity of the lateral margin of midbrain tegmentum referred to as the morning glory or Mickey Mouse sign.*

*Axial T2 MR in the same patient shows abnormal concavity of the lateral margin of midbrain tegmentum referred to as the morning glory or Mickey Mouse sign.*

*Sagittal T1WI MR (3D MPRAGE) in an 80-year-old woman with PSP shows striking midbrain volume loss, with the penguin or hummingbird sign manifested by a concave upper border of the midbrain . Note extreme thinning of the tectal plate . An incidental subependymoma was found.*

*Sagittal T1WI MR (3D MPRAGE) in an 80-year-old woman with PSP shows striking midbrain volume loss, with the penguin or hummingbird sign manifested by a concave upper border of the midbrain . Note extreme thinning of the tectal plate . An incidental subependymoma was found.*

*Axial FLAIR MR in the same patient shows the tectal plate is extremely thin , the lateral aspects of the midbrain are concave (morning glory sign), and the cerebral peduncles are atrophic.*

*Axial FLAIR MR in the same patient shows the tectal plate is extremely thin , the lateral aspects of the midbrain are concave (morning glory sign), and the cerebral peduncles are atrophic.*

*Sagittal T2WI MR in a patient with PSP shows diminished midbrain volume and thinned tectum .*

*Sagittal T2WI MR in a patient with PSP shows diminished midbrain volume and thinned tectum .*
 . This indicates nigrostriatal neuronal loss in bilateral striata. This cannot distinguish between idiopathic Parkinson disease (PD) and atypical PD.](images/app.statdx.com_image_thumbnail_b70f08e9-414e-479f-939d-7d172de5247c_size_168_quality_85_384955e2_20251014T204728Z.jpg)
*I-123 Ioflupane (DaTscan) SPECT images with axial reformats show segmentation of striata to anterior, mid, and posterior regions. Note significant decrease in radiotracer uptake right mid and posterior segments of right and mild decrease in left posterior segment . This indicates nigrostriatal neuronal loss in bilateral striata. This cannot distinguish between idiopathic Parkinson disease (PD) and atypical PD.*
*I-123 Ioflupane (DaTscan) SPECT images with axial reformats show segmentation of striata to anterior, mid, and posterior regions. Note significant decrease in radiotracer uptake right mid and posterior segments of right and mild decrease in left posterior segment . This indicates nigrostriatal neuronal loss in bilateral striata. This cannot distinguish between idiopathic Parkinson disease (PD) and atypical PD.*
### Additional Images
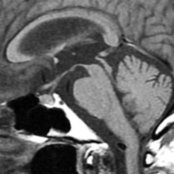
*Sagittal T1WI MR in a patient with progressive supranuclear palsy shows markedly diminished size of midbrain relative to pons. The cephalad surface of the midbrain appears concave , in contrast to the normal convex superior profile.*

*Sagittal T1WI MR in a patient with progressive supranuclear palsy shows markedly diminished size of midbrain relative to pons. The cephalad surface of the midbrain appears concave , in contrast to the normal convex superior profile.*
*Axial FLAIR MR in the same patient shows striking atrophy of the midbrain tectum (colliculi) and concave margins of the midbrain tegmentum .*
*Axial FLAIR MR in the same patient shows striking atrophy of the midbrain tectum (colliculi) and concave margins of the midbrain tegmentum .*
*Sagittal T1WI MR in a patient with progressive supranuclear palsy shows marked atrophy of the midbrain relative to pons. There is upper concavity of the midbrain tegmentum with a "penguin" or "hummingbird" sign and thinning of superior tectum .*
*Sagittal T1WI MR in a patient with progressive supranuclear palsy shows marked atrophy of the midbrain relative to pons. There is upper concavity of the midbrain tegmentum with a "penguin" or "hummingbird" sign and thinning of superior tectum .*

*Sagittal T1WI MR in normal healthy subject shows normal appearance of superior and inferior colliculi .*
*Sagittal T1WI MR in normal healthy subject shows normal appearance of superior and inferior colliculi .*
*Axial FLAIR MR in the same patient shows volume loss of the midbrain with concavity of lateral margin of tegmentum , termed the "morning glory" sign, characteristic of PSP.*

*Axial FLAIR MR in the same patient shows volume loss of the midbrain with concavity of lateral margin of tegmentum , termed the "morning glory" sign, characteristic of PSP.*
*Axial T2* GRE MR in patient with PSP shows no evidence for abnormal iron accumulation in the midbrain, which helps to distinguish PSP from PD.*
*Axial T2* GRE MR in patient with PSP shows no evidence for abnormal iron accumulation in the midbrain, which helps to distinguish PSP from PD.*
*Axial T2* GRE MR shows no evidence for abnormal iron accumulation in the striatum, another location in which iron is commonly found in PD.*
*Axial T2* GRE MR shows no evidence for abnormal iron accumulation in the striatum, another location in which iron is commonly found in PD.*
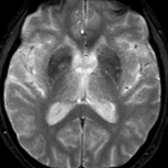
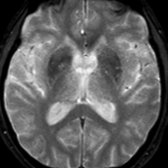
*Axial T2WI MR in the same patient shows volume loss of the midbrain with thinned tectum and concave lateral midbrain margins .*
*Axial T2WI MR in the same patient shows volume loss of the midbrain with thinned tectum and concave lateral midbrain margins .*
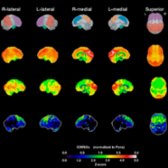
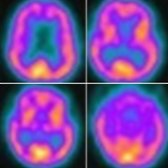
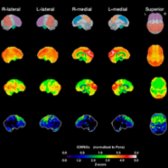
*PET scan with stereotaxic surface projections in the same patient is shown. The top row is the reference map. The 2nd row illustrates glucose metabolism in elderly normal controls (n = 27). The 3rd row is the patient's glucose metabolism map. The 4th row is the Z-score map. The glucose metabolism and Z-score maps show markedly reduced metabolism in both frontal lobes. (Courtesy N. Foster, MD.)*
*PET scan with stereotaxic surface projections in the same patient is shown. The top row is the reference map. The 2nd row illustrates glucose metabolism in elderly normal controls (n = 27). The 3rd row is the patient's glucose metabolism map. The 4th row is the Z-score map. The glucose metabolism and Z-score maps show markedly reduced metabolism in both frontal lobes. (Courtesy N. Foster, MD.)*
. This indicates nigrostriatal neuronal loss in bilateral striata. This cannot distinguish between idiopathic Parkinson disease (PD) and atypical PD.](images/app.statdx.com_image_thumbnail_b70f08e9-414e-479f-939d-7d172de5247c_size_168_quality_85_384955e2_20251014T204728Z.jpg)
*I-123 Ioflupane (DaTscan) SPECT images with axial reformats show segmentation of striata to anterior, mid, and posterior regions. Note significant decrease in radiotracer uptake right mid and posterior segments of right and mild decrease in left posterior segment . This indicates nigrostriatal neuronal loss in bilateral striata. This cannot distinguish between idiopathic Parkinson disease (PD) and atypical PD.*

*I-123 Ioflupane (DaTscan) SPECT images with axial reformats show segmentation of striata to anterior, mid, and posterior regions. Note significant decrease in radiotracer uptake right mid and posterior segments of right and mild decrease in left posterior segment . This indicates nigrostriatal neuronal loss in bilateral striata. This cannot distinguish between idiopathic Parkinson disease (PD) and atypical PD.*
### Additional Images

*Sagittal T1WI MR in a patient with progressive supranuclear palsy shows markedly diminished size of midbrain relative to pons. The cephalad surface of the midbrain appears concave , in contrast to the normal convex superior profile.*

*Sagittal T1WI MR in a patient with progressive supranuclear palsy shows markedly diminished size of midbrain relative to pons. The cephalad surface of the midbrain appears concave , in contrast to the normal convex superior profile.*

*Axial FLAIR MR in the same patient shows striking atrophy of the midbrain tectum (colliculi) and concave margins of the midbrain tegmentum .*

*Axial FLAIR MR in the same patient shows striking atrophy of the midbrain tectum (colliculi) and concave margins of the midbrain tegmentum .*

*Sagittal T1WI MR in a patient with progressive supranuclear palsy shows marked atrophy of the midbrain relative to pons. There is upper concavity of the midbrain tegmentum with a "penguin" or "hummingbird" sign and thinning of superior tectum .*

*Sagittal T1WI MR in a patient with progressive supranuclear palsy shows marked atrophy of the midbrain relative to pons. There is upper concavity of the midbrain tegmentum with a "penguin" or "hummingbird" sign and thinning of superior tectum .*

*Sagittal T1WI MR in normal healthy subject shows normal appearance of superior and inferior colliculi .*

*Sagittal T1WI MR in normal healthy subject shows normal appearance of superior and inferior colliculi .*

*Axial FLAIR MR in the same patient shows volume loss of the midbrain with concavity of lateral margin of tegmentum , termed the "morning glory" sign, characteristic of PSP.*

*Axial FLAIR MR in the same patient shows volume loss of the midbrain with concavity of lateral margin of tegmentum , termed the "morning glory" sign, characteristic of PSP.*

*Axial T2* GRE MR in patient with PSP shows no evidence for abnormal iron accumulation in the midbrain, which helps to distinguish PSP from PD.*

*Axial T2* GRE MR in patient with PSP shows no evidence for abnormal iron accumulation in the midbrain, which helps to distinguish PSP from PD.*

*Axial T2* GRE MR shows no evidence for abnormal iron accumulation in the striatum, another location in which iron is commonly found in PD.*

*Axial T2* GRE MR shows no evidence for abnormal iron accumulation in the striatum, another location in which iron is commonly found in PD.*

*Axial T2WI MR in the same patient shows volume loss of the midbrain with thinned tectum and concave lateral midbrain margins .*

*Axial T2WI MR in the same patient shows volume loss of the midbrain with thinned tectum and concave lateral midbrain margins .*

*PET scan with stereotaxic surface projections in the same patient is shown. The top row is the reference map. The 2nd row illustrates glucose metabolism in elderly normal controls (n = 27). The 3rd row is the patient's glucose metabolism map. The 4th row is the Z-score map. The glucose metabolism and Z-score maps show markedly reduced metabolism in both frontal lobes. (Courtesy N. Foster, MD.)*

*PET scan with stereotaxic surface projections in the same patient is shown. The top row is the reference map. The 2nd row illustrates glucose metabolism in elderly normal controls (n = 27). The 3rd row is the patient's glucose metabolism map. The 4th row is the Z-score map. The glucose metabolism and Z-score maps show markedly reduced metabolism in both frontal lobes. (Courtesy N. Foster, MD.)*