---
title: "Sellar/Parasellar Mass With Skull Base Invasion"
docid: "9465656a-fba7-46d3-8538-2307f2441151"
authors:
- key: "e0282a62-994d-4550-a127-1eb773b1e920"
value: "Blair A. Winegar, MD"
- key: "5cff4116-3654-4b3a-bb75-5ebe0b8c9850"
value: "Anne G. Osborn, MD, FACR"
breadcrumbs:
-
name: "Brain"
slug: "brain"
treeNodeId: "6d8829f1-14d7-45af-8675-255189aa526a"
-
name: "Differential Diagnosis"
slug: "differential-diagnosis"
treeNodeId: "a7fdd139-664e-4bb8-8d18-400e4733ff60"
-
name: "Sella/Juxtasellar, Pineal Region"
slug: "sellajuxtasellar-pineal-region"
treeNodeId: "5e38b9c1-3137-47e3-aa83-1fc82cb4099a"
-
name: "Anatomically Based Differentials"
slug: "anatomically-based-differentials"
treeNodeId: "7a51b2ca-8fee-4c16-aff3-b7189f68ea60"
-
name: "Sellar/Parasellar Mass With Skull Base Invasion"
slug: "sellarparasellar-mass-with-skull-b-"
treeNodeId: null
category: "Brain"
documentVersionId: "144664c4-89e2-415f-836d-1f31c40a378f"
imageCount: 29
lastUpdated: "01/26/23"
pageDescription: "Sellar/Parasellar Mass With Skull Base Invasion"
pageKeywords: "Brain, Differential Diagnosis, Sella/Juxtasellar, Pineal Region, Anatomically Based Differentials, Sellar/Parasellar Mass With Skull Base Invasion"
pageTitle: "Sellar/Parasellar Mass With Skull Base Invasion | STATdx"
enhancedTitle: "Sellar/Parasellar Mass With Skull Base Invasion"
type: "DDX"
references: true
breadcrumbs:
- "Brain"
- "Differential Diagnosis"
- "Sella/Juxtasellar, Pineal Region"
- "Anatomically Based Differentials"
- "Sellar/Parasellar Mass With Skull Base Invasion"
---
# ESSENTIAL INFORMATION
- ## Key Differential Diagnosis Issues
- Pattern of skull base involvement
- Included: Lesion(s) with permeative, infiltrative, destructive features
- Invasive macroadenoma, metastases, lymphoma
- Excluded: Lesion(s) with expansile, erosive pattern (e.g., trigeminal schwannoma, aneurysm)
- Anatomic origin
- Included: Involvement from lesions mostly above or lateral to central base of skull (BOS)
- Excluded: Involvement due to cephalad extension from structures below central BOS
- Sphenoid sinus (e.g., aggressive polyposis, invasive fungal sinusitis)
- Nasopharynx (carcinomas with direct or perineural extension)
- Specific origin of mass helpful
- Pituitary gland
- Macroadenoma
- Less common lymphoma, metastasis
- Cavernous sinus (CS)/dura
- Metastasis, lymphoma, meningioma, myeloma
- Less common hemangiomas, histiocytoses
- Clivus
- Metastasis, lymphoma, myeloma, chordoma
- Petrooccipital fissure
- Chondrosarcoma
- Key imaging findings help
- Look for pituitary gland separate from mass
- If cannot find, mass probably of pituitary origin
- Adult: Macroadenoma > metastasis, lymphoma, pseudotumor
- Child: Histiocytosis > macroadenoma, leukemia
- Intracranial dural involvement
- Adult: Metastasis, meningioma, lymphoma, pseudotumor
- Child: Histiocytosis, leukemia
- Associated multiple enhancing cranial nerves
- Adult: Metastases, lymphoma
- Child: Leukemia
- ## Helpful Clues for Common Diagnoses
- **Pituitary Macroadenoma**
- Pituitary gland = mass
- Most commonly invades upward through diaphragma sellae
- Less common = inferior extension
- Rare but important = invasion, destruction of central BOS
- If adult man with invasive, destructive central BOS mass, check prolactin prior to surgery, biopsy
- Infrasellar pituitary adenoma
- Extremely rare tumors, completely within sphenoid body
- Develop from ectopic pituitary tissue in remnants of Rathke pouch
- **Metastases**
- May arise from many sellar/parasellar tissues (e.g., pituitary gland, dura, osseous BOS)
- Can involve, infiltrate pituitary gland/stalk
- Extend into central BOS, CSs
- Look for other lesions (e.g. calvarium, brain)
- ## Helpful Clues for Less Common Diagnoses
- **Meningioma****, Skull Base**
- Most common = suprasellar mass extending into CS
- Frequent associated osseous changes: Hyperostosis, sclerosis
- Look for pituitary gland separate from mass
- Pituitary usually displaced inferiorly, laterally
- Occasionally can be elevated
- Beware: Meningiomas occasionally appear aggressive, invade adjacent skull (mimic metastasis, lymphoma, etc.)
- **Lymphoma, Metastatic, Intracranial**
- Metastatic > primary lymphoma in/around central BOS, sella/CSs
- Uni- > bilateral CS involvement
- May infiltrate pituitary gland, stalk, cranial nerves, dura
- Isointense, avidly enhancing, reduced diffusion
- **Myeloma**
- Multifocal or solitary (plasmacytoma)
- Central BOS > > pituitary, CS
- Bilateral > unilateral CS
- Usually elevates, displaces pituitary gland but occasionally invades gland, stalk
- ## Helpful Clues for Rare Diagnoses
- **Pseudotumor, Intracranial**
- 90% of intracranial pseudotumors occur without orbital disease
- Originates in CS, dura
- Smooth > "lumpy-bumpy" dural thickening, enhancement
- Typically ↓ following steroids
- May be part of IgG4-related disease
- Less common: Posterior extension from orbit
- Tolosa-Hunt syndrome (painful ophthalmoplegia) = CS involved
- Uni- > bilateral disease
- Look for associated meningeal thickening (can be extensive)
- Rare variant = idiopathic invasive pseudotumor
- Can invade, destroy bone, mimic neoplasm or aggressive infection
- Child > > adult
- **Langerhans Cell Histiocytosis**
- Osteolysis ± soft tissue mass
- Varies from small, punched-out lesion to widespread, diffuse involvement
- Variable brain lesions (pituitary stalk/gland, meninges > parenchyma, choroid plexus)
- **Thrombophlebitis, Cavernous Sinus**
- Mimic: Osteolysis central BOS rare
- Usually secondary to paranasal sinus infection
- Look for dural thickening, filling defects in CS
- **Chordoma, Extraosseous**
- Typical chordoma originates in clivus
- Destructive midline mass
- May indent ("thumb") pons
- Rare: Extraosseous origin
- Laterally located mass in CS, Meckel cave
- Osseous invasion secondary
- Typically hyperintense on T2WI, strong uniform enhancement
- **Chondrosarcoma**
- Typically centered on petrooccipital fissure
- Rare sellar/parasellar location
- Possible chondroid tumor matrix calcification
- High T2 signal with scattered hypointense foci (calcifications), heterogeneous enhancement
- High ADC map value (≥ 2.0 x 10⁻³ mm²/sec)
- **Leukemia**
- Paranasal sinus/orbit involvement typical
- May extend into 1 or both CSs, pituitary gland/stalk
- **Hemangioma**
- True vasoformative neoplasm of CS, dura
- May mimic meningioma
- If child without neurofibromatosis type 2 lesion that looks like meningioma, consider hemangioma
- If large, may involve adjacent bone
- **Erdheim-Chester Disease**
- Rare non-Langerhans cell histiocytosis
- Disseminated xanthogranulomatous infiltrative disease
- Adults > children
- Long bones > brain, CS, orbits (rare)
## References
# Selected References
1. [Goulam-Houssein S et al: IgG4-related intracranial disease. Neuroradiol J. 32(1):29-35, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30320530%5Bpmid%5D)
1. [Kunimatsu A et al: Skull base tumors and tumor-like lesions: a pictorial review. Pol J Radiol. 82:398-409, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=28811848%5Bpmid%5D)
1. [Sharma M et al: Pituitary chondrosarcoma presenting as a sellar and suprasellar mass with parasellar extension: an unusual presentation. Iran J Pathol. 11(2):161-6, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27499779%5Bpmid%5D)
1. [Koiso T et al: Malignant lymphoma in the parasellar region. Case Rep Med. 2014:747280, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24660002%5Bpmid%5D)
1. [Yeom KW et al: Diffusion-weighted MRI: distinction of skull base chordoma from chondrosarcoma. AJNR Am J Neuroradiol. 34(5):1056-61, S1, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=23124635%5Bpmid%5D)
1. [Chen X et al: Clival invasion on multi-detector CT in 390 pituitary macroadenomas: correlation with sex, subtype and rates of operative complication and recurrence. AJNR Am J Neuroradiol. 32(4):785-9, 2011](http://www.ncbi.nlm.nih.gov/pubmed/?term=21436342%5Bpmid%5D)
## Images
### Selected Images
 with suprasellar extension
with suprasellar extension  and skull base invasion
and skull base invasion  .](images/app.statdx.com_image_thumbnail_08d04109-a126-406c-b98f-5670f35ffed6_annotated_true_size_900_quality_90_3ad6e337.jpg)
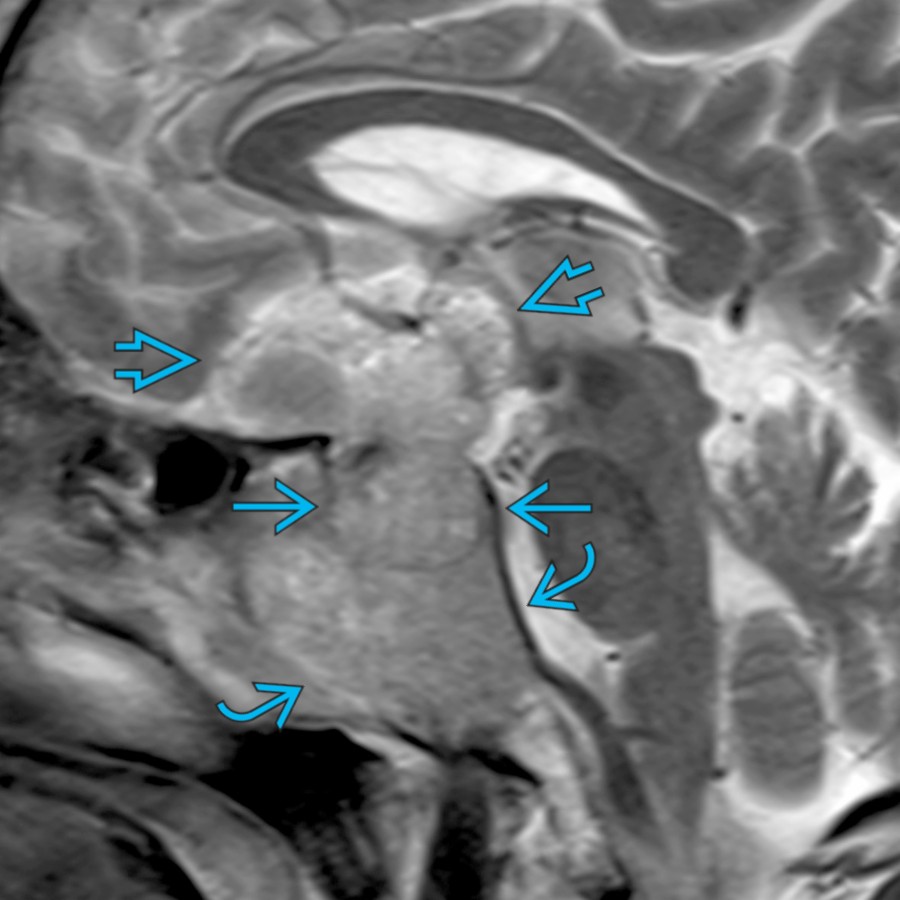
**Pituitary Macroadenoma**
*Sagittal T2 MR shows a heterogeneous mass indistinguishable from the pituitary gland, which expands the sella with suprasellar extension and skull base invasion .*
**Pituitary Macroadenoma**
*Sagittal T2 MR shows a heterogeneous mass indistinguishable from the pituitary gland, which expands the sella with suprasellar extension and skull base invasion .*

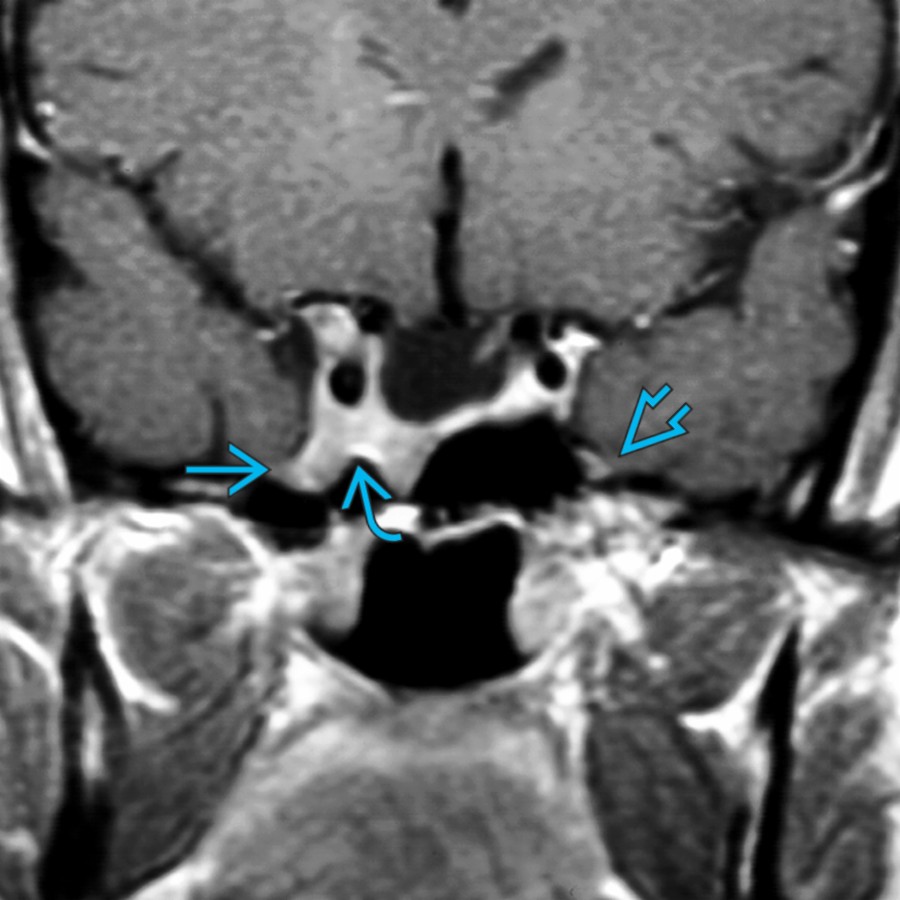
**Pituitary Macroadenoma**
*Coronal T1 C+ FS MR in the same patient shows a heterogeneous, hypoenhancing mass that invades the skull base and encases the bilateral internal carotid artery (ICA) without luminal narrowing in this case of invasive pituitary macroadenoma.*

**Metastases**
*Coronal CECT in a patient with metastatic breast carcinoma shows a large sellar/parasellar mass with extension to the cavernous sinus and destruction of the adjacent central skull base.*

**Metastases**
*Sagittal T1 MR shows an infiltrative T1-hypointense lesion in the pituitary gland and clivus with adjacent dural thickening . An additional cervical spine osseous lesion is present in this case of metastatic prostate cancer.*

**Meningioma, Skull Base**
*Axial T2 FS MR demonstrates a large central and posterior skull base mass with extension to the sella (cavernous sinus) along the petroclival ligament and petrous bone . Note the decrease in the caliber of the encased cavernous carotid artery .*

**Meningioma, Skull Base**
*Coronal T1 C+ MR in the same patient shows homogeneous enhancement of the mass. Note the normal pituitary gland is compressed and displaced to the right. Surgical pathology was consistent with a meningioma.*

**Lymphoma, Metastatic, Intracranial**
*Sagittal T1 C+ MR demonstrates an enhancing mass invading the pituitary gland, stalk , central skull base, and nasopharynx . Note the dural involvement with thickening and enhancement of the dura.*

**Myeloma**
*Coronal T1 C+ FS MR shows a destructive, enhancing mass within the skull base with intracranial and extracranial extension. Additional enhancing osseous lesions in the mandible and skull are present in this case of myeloma.*

**Pseudotumor, Intracranial**
*Coronal T1 C+ MR demonstrates an infiltrating lesion in the right parasellar region involving the cavernous sinus and Meckel cave. The adjacent skull base shows abnormal marrow enhancement . Endoscopic biopsy revealed an inflammatory pseudotumor.*

**Pseudotumor, Intracranial**
*Axial T1 C+ FS MR shows an infiltrative, enhancing lesion in the central skull base with adjacent dural thickening and involving the petrous ICA canals in this biopsy-proven inflammatory pseudotumor.*

**Langerhans Cell Histiocytosis**
*Sagittal T1 C+ MR demonstrates an extensive, enhancing mass involving the pituitary gland and stalk , central skull base, and nasopharynx. This patient was a 6-year-old with a history of sinus treatment and new-onset right vision loss.*

**Chordoma, Extraosseous**
*Coronal T2 MR shows a lobulated, hyperintense chordoma in the right sellar/parasellar region. Note the displacement of the pituitary gland .*

**Chondrosarcoma**
*Axial T2 FS MR shows a hyperintense mass with internal hypointense chondroid matrix centered in the right central skull base with mild mass effect upon the pituitary gland in this case of chondrosarcoma.*

**Leukemia**
*Axial T1 C+ MR in a patient with acute lymphoblastic leukemia and multiple cranial neuropathies shows enhancing soft tissue in the cavernous sinuses and along the trigeminal nerves. Note the involvement of the adjacent sphenoid .*

**Hemangioma**
*Axial T1 C+ MR in a 13-year-old shows an enormous left cavernous invasive, enhancing mass . An initial trigeminal schwannoma or meningioma differential diagnosis gave way to the surgical pathologic diagnosis of a hemangioma.*

**Erdheim-Chester Disease**
*Axial T1 C+ MR in a patient with Erdheim-Chester disease reveals large bilateral cavernous sinuses and a mass that invades the skull base with multifocal enhancing cerebellar lesions . (Courtesy M. Warmuth-Metz, MD.)*
### Additional Images
**Pituitary Macroadenoma**
*Sagittal T2 MR shows a heterogeneous mass indistinguishable from the pituitary gland, which expands the sella with suprasellar extension and skull base invasion .*

**Pituitary Macroadenoma**
*Sagittal T2 MR shows a heterogeneous mass indistinguishable from the pituitary gland, which expands the sella with suprasellar extension and skull base invasion .*

**Pituitary Macroadenoma**
*Coronal T1 C+ FS MR in the same patient shows a heterogeneous, hypoenhancing mass that invades the skull base and encases the bilateral internal carotid artery (ICA) without luminal narrowing in this case of invasive pituitary macroadenoma.*

**Metastases**
*Coronal CECT in a patient with metastatic breast carcinoma shows a large sellar/parasellar mass with extension to the cavernous sinus and destruction of the adjacent central skull base.*

**Metastases**
*Sagittal T1 MR shows an infiltrative T1-hypointense lesion in the pituitary gland and clivus with adjacent dural thickening . An additional cervical spine osseous lesion is present in this case of metastatic prostate cancer.*

**Meningioma, Skull Base**
*Axial T2 FS MR demonstrates a large central and posterior skull base mass with extension to the sella (cavernous sinus) along the petroclival ligament and petrous bone . Note the decrease in the caliber of the encased cavernous carotid artery .*

**Meningioma, Skull Base**
*Coronal T1 C+ MR in the same patient shows homogeneous enhancement of the mass. Note the normal pituitary gland is compressed and displaced to the right. Surgical pathology was consistent with a meningioma.*

**Lymphoma, Metastatic, Intracranial**
*Sagittal T1 C+ MR demonstrates an enhancing mass invading the pituitary gland, stalk , central skull base, and nasopharynx . Note the dural involvement with thickening and enhancement of the dura.*

**Myeloma**
*Coronal T1 C+ FS MR shows a destructive, enhancing mass within the skull base with intracranial and extracranial extension. Additional enhancing osseous lesions in the mandible and skull are present in this case of myeloma.*

**Pseudotumor, Intracranial**
*Coronal T1 C+ MR demonstrates an infiltrating lesion in the right parasellar region involving the cavernous sinus and Meckel cave. The adjacent skull base shows abnormal marrow enhancement . Endoscopic biopsy revealed an inflammatory pseudotumor.*

**Pseudotumor, Intracranial**
*Axial T1 C+ FS MR shows an infiltrative, enhancing lesion in the central skull base with adjacent dural thickening and involving the petrous ICA canals in this biopsy-proven inflammatory pseudotumor.*

**Langerhans Cell Histiocytosis**
*Sagittal T1 C+ MR demonstrates an extensive, enhancing mass involving the pituitary gland and stalk , central skull base, and nasopharynx. This patient was a 6-year-old with a history of sinus treatment and new-onset right vision loss.*

**Chordoma, Extraosseous**
*Coronal T2 MR shows a lobulated, hyperintense chordoma in the right sellar/parasellar region. Note the displacement of the pituitary gland .*

**Chondrosarcoma**
*Axial T2 FS MR shows a hyperintense mass with internal hypointense chondroid matrix centered in the right central skull base with mild mass effect upon the pituitary gland in this case of chondrosarcoma.*

**Leukemia**
*Axial T1 C+ MR in a patient with acute lymphoblastic leukemia and multiple cranial neuropathies shows enhancing soft tissue in the cavernous sinuses and along the trigeminal nerves. Note the involvement of the adjacent sphenoid .*

**Hemangioma**
*Axial T1 C+ MR in a 13-year-old shows an enormous left cavernous invasive, enhancing mass . An initial trigeminal schwannoma or meningioma differential diagnosis gave way to the surgical pathologic diagnosis of a hemangioma.*

**Erdheim-Chester Disease**
*Axial T1 C+ MR in a patient with Erdheim-Chester disease reveals large bilateral cavernous sinuses and a mass that invades the skull base with multifocal enhancing cerebellar lesions . (Courtesy M. Warmuth-Metz, MD.)*
### Additional Images
 , orbit
, orbit  , and sphenoid sinus
, and sphenoid sinus  .](80293d2a-07da-421c-b377-33d57c05155b)
**Meningioma, Skull Base**
*Axial CECT shows an "en plaque" meningioma that involves the left cavernous sinus , orbit , and sphenoid sinus .*

**Chordoma, Extraosseous**
*Coronal T1 C+ MR demonstrates a mildly enhancing lesion in the left cavernous sinus and Meckel cave from chordoma with central skull base destruction .*

**Pituitary Macroadenoma**
*Sagittal T2 MR shows a hyperintense extensively invasive mass . The pituitary gland cannot be identified separately from the lesion in this male patient with elevated prolactin and an invasive macroadenoma.*

**Meningioma, Skull Base**
*Coronal T1 C+ MR shows a large, enhancing mass that elevates and displaces the pituitary gland . Note the bone erosion . A transsphenoidal biopsy specimen disclosed a typical meningioma.*

**Pseudotumor, Intracranial**
*Coronal T1 C+ MR in a patient with multiple left-sided cranial neuropathies shows an enhancing left cavernous sinus mass extending into the skull base and nasopharynx . Note dural involvement . Symptoms resolved completely with steroids.*

**Langerhans Cell Histiocytosis**
*Coronal T1 C+ FS MR in a patient with Langerhans cell histiocytosis shows an extensive destructive central mass that erodes the skull base and infiltrates the pituitary gland and cavernous sinuses.*

**Hemangioma**
*Coronal T1 C+ MR in a 13-year-old patient demonstrates a large hemangioma involving the sella , cavernous sinus , and floor of the middle cranial fossa .*

**Meningioma, Skull Base**
*Axial CECT shows an "en plaque" meningioma that involves the left cavernous sinus , orbit , and sphenoid sinus .*

**Chordoma, Extraosseous**
*Coronal T1 C+ MR demonstrates a mildly enhancing lesion in the left cavernous sinus and Meckel cave from chordoma with central skull base destruction .*

**Pituitary Macroadenoma**
*Sagittal T2 MR shows a hyperintense extensively invasive mass . The pituitary gland cannot be identified separately from the lesion in this male patient with elevated prolactin and an invasive macroadenoma.*

**Meningioma, Skull Base**
*Coronal T1 C+ MR shows a large, enhancing mass that elevates and displaces the pituitary gland . Note the bone erosion . A transsphenoidal biopsy specimen disclosed a typical meningioma.*

**Pseudotumor, Intracranial**
*Coronal T1 C+ MR in a patient with multiple left-sided cranial neuropathies shows an enhancing left cavernous sinus mass extending into the skull base and nasopharynx . Note dural involvement . Symptoms resolved completely with steroids.*

**Langerhans Cell Histiocytosis**
*Coronal T1 C+ FS MR in a patient with Langerhans cell histiocytosis shows an extensive destructive central mass that erodes the skull base and infiltrates the pituitary gland and cavernous sinuses.*

**Hemangioma**
*Coronal T1 C+ MR in a 13-year-old patient demonstrates a large hemangioma involving the sella , cavernous sinus , and floor of the middle cranial fossa .*
 . Note the displacement of the pituitary gland .](47b3cc21-cd6a-4102-897b-b27602c09cb9)
**Chordoma, Extraosseous**
*Axial T2 MR reveals a very hyperintense mass that originates in the left cavernous sinus with bone destruction . Note the displacement of the pituitary gland .*

**Myeloma**
*Sagittal T1 MR in a patient with myeloma reveals an infiltrative, destructive lesion with involvement of the cavernous sinus, sphenoid sinus, clivus, and dura. The pituitary gland is seen separate from the mass .*
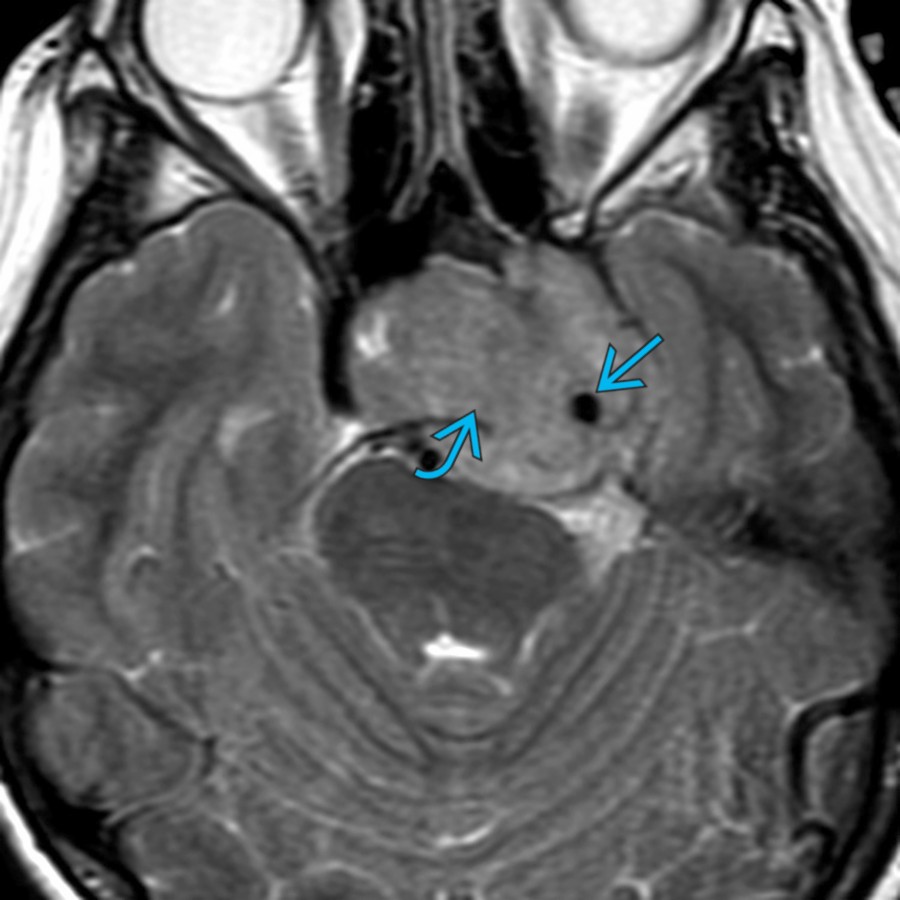
**Pituitary Macroadenoma**
*Axial T2 MR demonstrates a large, lobulated sellar/parasellar mass with extension to the left cavernous sinus. Note encasement of the left cavernous carotid artery .*

**Pituitary Macroadenoma**
*Coronal T1 C+ MR in the same patient shows homogeneous enhancement of the mass. There is involvement of the adjacent skull base , and the pituitary gland was not seen separate from the mass. These findings are typical of a giant pituitary macroadenoma.*
**Metastases**
*Coronal T1 C+ MR shows a mass in the right cavernous sinus extending into the foramen rotundum in a patient with ovarian cancer and right facial numbness. Compare to the normal left side .*

**Chondrosarcoma**
*Coronal T1 C+ MR demonstrates a skull base chondrosarcoma with extension to the right cavernous sinus and Meckel cave. Note the normal enhancing pituitary gland . CT (not shown) demonstrated chondroid-type calcifications in the mass.*
. Note the displacement of the pituitary gland .](47b3cc21-cd6a-4102-897b-b27602c09cb9)
**Chordoma, Extraosseous**
*Axial T2 MR reveals a very hyperintense mass that originates in the left cavernous sinus with bone destruction . Note the displacement of the pituitary gland .*

**Myeloma**
*Sagittal T1 MR in a patient with myeloma reveals an infiltrative, destructive lesion with involvement of the cavernous sinus, sphenoid sinus, clivus, and dura. The pituitary gland is seen separate from the mass .*

**Pituitary Macroadenoma**
*Axial T2 MR demonstrates a large, lobulated sellar/parasellar mass with extension to the left cavernous sinus. Note encasement of the left cavernous carotid artery .*

**Pituitary Macroadenoma**
*Coronal T1 C+ MR in the same patient shows homogeneous enhancement of the mass. There is involvement of the adjacent skull base , and the pituitary gland was not seen separate from the mass. These findings are typical of a giant pituitary macroadenoma.*

**Metastases**
*Coronal T1 C+ MR shows a mass in the right cavernous sinus extending into the foramen rotundum in a patient with ovarian cancer and right facial numbness. Compare to the normal left side .*

**Chondrosarcoma**
*Coronal T1 C+ MR demonstrates a skull base chondrosarcoma with extension to the right cavernous sinus and Meckel cave. Note the normal enhancing pituitary gland . CT (not shown) demonstrated chondroid-type calcifications in the mass.*