---
title: "Sensorineural Hearing Loss in Adult"
docid: "08d468da-fbc3-44f8-8212-6480e0a152c4"
authors:
- key: "eef2f839-5706-47b9-89c3-60d8315b2b3a"
value: "Nicholas A. Koontz, MD"
breadcrumbs:
-
name: "Head and Neck"
slug: "head-and-neck"
treeNodeId: "ed24ed8c-5d57-4629-879b-447b82d2973d"
-
name: "Differential Diagnosis"
slug: "differential-diagnosis"
treeNodeId: "40d68862-8975-4dde-ac2b-ebc43ab0fb5c"
-
name: "CPA-IAC and Posterior Fossa"
slug: "cpa-iac-and-posterior-fossa"
treeNodeId: "c590eedb-4a3b-4158-a04f-ad880564c992"
-
name: "Clinically Based Differentials"
slug: "clinically-based-differentials"
treeNodeId: "55dd15ac-e67d-48dd-8134-f52884dab28b"
-
name: "Sensorineural Hearing Loss in Adult"
slug: "sensorineural-hearing-loss-in-adult"
treeNodeId: null
category: "Head and Neck"
documentVersionId: "2268573f-6f13-4d60-b402-841d07de264c"
imageCount: 32
lastUpdated: "07/24/18"
pageDescription: "Sensorineural Hearing Loss in Adult"
pageKeywords: "Head and Neck, Differential Diagnosis, CPA-IAC and Posterior Fossa, Clinically Based Differentials, Sensorineural Hearing Loss in Adult"
pageTitle: "Sensorineural Hearing Loss in Adult | STATdx"
enhancedTitle: "Sensorineural Hearing Loss in Adult"
type: "DDX"
references: true
breadcrumbs:
- "Head and Neck"
- "Differential Diagnosis"
- "CPA-IAC and Posterior Fossa"
- "Clinically Based Differentials"
- "Sensorineural Hearing Loss in Adult"
---
# ESSENTIAL INFORMATION
- ## Key Differential Diagnosis Issues
- Many diagnoses cause sensorineural hearing loss (SNHL)
- Relative statistical incidence of major differential diagnoses
- **Vestibular schwannoma**: **90%** of lesions causing SNHL
- CPA meningioma, epidermoid cyst, aneurysm: 5% of all lesions causing SNHL
- All other diagnoses in SNHL differential diagnosis list: 5%
- Best imaging tool
- MR best for SNHL patients
- High-resolution/volumetric T2: Best for surgical anatomy, nerve of origin, & fundal CSF cap in setting of vestibular schwannoma
- T1 C+ T1 fat-saturated: Helps make labyrinthitis, vestibular neuritis, Ramsay Hunt syndrome diagnoses
- Increasing role of pre- & postcontrast 3D FLAIR in assessing sudden (onset < 72 hours) SNHL
- Differentiates vascular (methemoglobin → bright inner ear signal on T1 C- & 3D FLAIR C-) from inflammatory (proteinaceous exudate → bright inner ear signal only on 3D FLAIR C-) etiologies
- Inner ear enhancement on 3D FLAIR C+ identifies blood-labyrinth barrier breakdown
- ## Helpful Clues for Common Diagnoses
- **Vestibular Schwannoma**
- Morphology
- "Ice cream on cone" mass aligned with CPA-IAC
- Imaging findings
- T1 C+ MR: Enhancing lesion ± intramural cysts
- High-resolution/volumetric T2: Fundal cap size, relationship of tumor to cochlear nerve canal, & (if small) nerve of origin
- GRE/SWI: ± microhemorrhages with blooming artifact
- **Meningioma in CPA**
- Morphology
- Dural-based mass often asymmetric to porus acusticus
- Imaging findings
- T1 C+ MR: Enhancing mass ± dural tails ± CSF-vascular cleft between mass & brainstem
- **Epidermoid Cyst in CPA**
- Morphology
- Insinuating with brainstem margin
- Imaging findings
- T1 C+ MR: Nonenhancing mass may be difficult to see
- DWI: Reduced diffusivity makes diagnosis
- **Aneurysm in CPA**
- Morphology
- Ovoid or fusiform CPA mass; rarely in IAC
- Imaging findings
- T1 & T1 C+ MR: Complex signal mass from wall calcification, clot, & flow
- MRA, CTA, or catheter angiography confirmatory
- **T-Bone****Fracture**
- T-bone CT essential; imaging findings
- Transverse, longitudinal, or complex fracture crosses inner ear structures ± pneumolabyrinth
- ## Helpful Clues for Less Common Diagnoses
- **Cochlear Otosclerosis**
- Pathophysiology: Etiology unknown; osteodystrophy of otic capsule
- Imaging findings
- Bone CT: Radiolucent foci in bony labyrinth
- T1 C+ MR: Multiple enhancing foci in bony labyrinth
- **Metastases in CPA-IAC**
- Imaging findings
- T1 C+ MR: Multiple enhancing lesions involving flocculus, choroid plexus, pia-arachnoid, or dura
- **Facial Nerve Schwannoma in CPA-IAC**
- Imaging findings
- Bone CT: Labyrinthine segment facial nerve canal enlarged = labyrinthine tail
- T1 C+ MR: Enhancing tubular mass affects CPA-IAC & labyrinthine segment of facial nerve
- **Lipoma in CPA-IAC**
- Imaging findings
- NECT: Fatty lesion of CPA, IAC ± inner ear
- T1 MR: High-signal lesion as above; fat saturation suppresses fat signal
- **Large Endolymphatic Sac Anomaly (IP-2)**
- Most common lesion found in children with bilateral congenital SNHL
- Imaging findings
- Bone CT: Large bony vestibular aqueduct ± mild cochlear malformation
- Axial CT: ≥ 1 mm at midpoint, ≥ 2 mm at operculum
- MR: Large endolymphatic sac & duct ± incomplete cochlear partitioning &/or deficient modiolus
- **Intralabyrinthine Schwannoma**
- Name based on anatomic location: Intracochlear, intralabyrinthine, vestibulocochlear, transmodiolar, transmacular, & transotic types
- Imaging findings
- T1 C+ MR: Intralabyrinthine enhancing lesion
- High-resolution T2 MR: Focal filling defect within high-signal intralabyrinthine fluid
- **Labyrinthitis**
- Imaging findings
- T1 C+ MR: Diffuse (less commonly focal) enhancement of labyrinth
- Facial or vestibulocochlear nerves may also enhance
- **Vestibulocochlear****Neuritis**
- Imaging findings: T1 C+ MR: Linear enhancement in CPA-IAC cisterns
- **Paget Disease in T-Bone**
- Clinical: Patient > 50 years of age
- Imaging findings
- Bone CT: Expansile bony lesion with cotton-wool appearance; may involve otic capsule
- T1 C+ MR: Heterogeneous enhancement within expanded T-bone, skull base, & calvarium
- **Fibrous Dysplasia****in****T-Bone**
- Clinical: Patient < 30 years of age
- Imaging findings
- Bone CT: Expansile lesion with ground-glass/sclerotic & cystic components; spares otic capsule
- MR: Expansile lesion with heterogeneous signal
- T1 C+ MR: Heterogeneous avid enhancement mixed with areas of minimal to no enhancement
- ## Helpful Clues for Rare Diagnoses
- **Endolymphatic Sac Tumor**
- Tumor centered in endolymphatic duct or sac area of posterior T-bone
- Imaging findings
- Bone CT: Spiculated or coarse calcifications within tumor matrix with thin posterior marginal calcification
- T1 MR: Multifocal high-signal tumor foci (blood products in tumor matrix)
- **Sarcoidosis in CPA**
- Laboratory: CSF lymphocystosis; increased blood angiotensin-converting enzyme (ACE)
- Morphology: En plaque, nodular, or linear masses
- Imaging findings
- T1 C+ MR: Multifocal dural-based enhancing lesions
- **Superficial Siderosis****in****CPA-IAC**
- Clinical: Bilateral SNHL with ataxia
- Imaging findings
- GRE/SWI MR: Blooming dark signal (hemosiderin) along surface of cerebellum & cranial nerves
- MR may also be used to identify site of chronic bleeding: Surgical site, aneurysm, tumor, or arteriovenous malformation, including spin
- **IAC/Temporal Bone Facial Nerve Venous Malformation ("Hemangioma")**
- Imaging findings
- CT: Punctate calcification in IAC lesion
- T1 C+ MR: Enhancing lesion in IAC with focal low-signal areas (calcifications)
- **Ramsay Hunt Syndrome**
- Clinical: External ear vesicles ± CNVII or CNVIII neuropathy
- Imaging findings: T1 C+ MR: Linear enhancing foci in IAC
- **Susac Syndrome (Retinocochleocerebral Vasculopathy)**
- Clinical: Classic triad of branch retinal artery occlusions, SNHL (often with vestibular symptoms), & encephalopathy (including headaches)
- Imaging findings
- T2/FLAIR MR: Multifocal white matter (WM) lesions, often round & involving mid callosal region
- T1 C+ MR: Variable enhancement of WM lesions; ± leptomeningeal enhancement
## References
# Selected References
1. [Coffey N et al: Imaging findings in sensorineural hearing loss: a pictorial essay. Can Assoc Radiol J. 68(2):106-115, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=27209216%5Bpmid%5D)
1. [Conte G et al: MR imaging in sudden sensorineural hearing loss. Time to Talk. AJNR Am J Neuroradiol. ePub, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=28546251%5Bpmid%5D)
1. [Lee JI et al: Prognostic Value of Labyrinthine 3D-FLAIR Abnormalities in Idiopathic Sudden Sensorineural Hearing Loss. AJNR Am J Neuroradiol. 37(12):2317-2322, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27516239%5Bpmid%5D)
1. [Naganawa S et al: Heavily T₂-Weighted 3D-FLAIR Improves the Detection of Cochlear Lymph Fluid Signal Abnormalities in Patients with Sudden Sensorineural Hearing Loss. Magn Reson Med Sci. 15(2):203-11, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=26597430%5Bpmid%5D)
1. [Pakdaman MN et al: Blood-Labyrinth Barrier Permeability in Menière Disease and Idiopathic Sudden Sensorineural Hearing Loss: Findings on Delayed Postcontrast 3D-FLAIR MRI. AJNR Am J Neuroradiol. ePub, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27256854%5Bpmid%5D)
1. [Cerqueira AC et al: Superficial siderosis of the central nervous system: an unusual cause of sensorineural hearing loss. Arq Neuropsiquiatr. 68(3):469-71, 2010](http://www.ncbi.nlm.nih.gov/pubmed/?term=20602058%5Bpmid%5D)
1. [Goyault G et al: Leptomeningeal carcinomatosis and sensorineural hearing loss: correlation of labyrinthine enhancement patterns with symptoms. J Neuroradiol. 36(2):98-101, 2009](http://www.ncbi.nlm.nih.gov/pubmed/?term=19144408%5Bpmid%5D)
1. [Thamburaj K et al: Intratumoral microhemorrhages on T2*-weighted gradient-echo imaging helps differentiate vestibular schwannoma from meningioma. AJNR Am J Neuroradiol. 29(3):552-7, 2008](http://www.ncbi.nlm.nih.gov/pubmed/?term=18079187%5Bpmid%5D)
1. [Daniels RL et al: Causes of unilateral sensorineural hearing loss screened by high-resolution fast spin echo magnetic resonance imaging: review of 1,070 consecutive cases. Am J Otol. 21(2):173-80, 2000](http://www.ncbi.nlm.nih.gov/pubmed/?term=10733180%5Bpmid%5D)
1. [Davidson HC et al: MR evaluation of vestibulocochlear anomalies associated with large endolymphatic duct and sac. AJNR Am J Neuroradiol. 20(8):1435-41, 1999](http://www.ncbi.nlm.nih.gov/pubmed/?term=10512225%5Bpmid%5D)
1. [Swartz JD: Sensorineural hearing deficit: a systematic approach based on imaging findings. Radiographics. 16(3):561-74, 1996](http://www.ncbi.nlm.nih.gov/pubmed/?term=8897624%5Bpmid%5D)
## Images
### Selected Images
 with avid, heterogeneous enhancement. Note tumor growth along the location of the vestibular nerve within the posterior IAC
with avid, heterogeneous enhancement. Note tumor growth along the location of the vestibular nerve within the posterior IAC  .](images/app.statdx.com_image_thumbnail_d3735149-87ba-4946-a6be-f0b1f08d305f_annotated_true_size_900_quality_90_530bc584132808c88933cbc23f234521e5322f13.jpg)
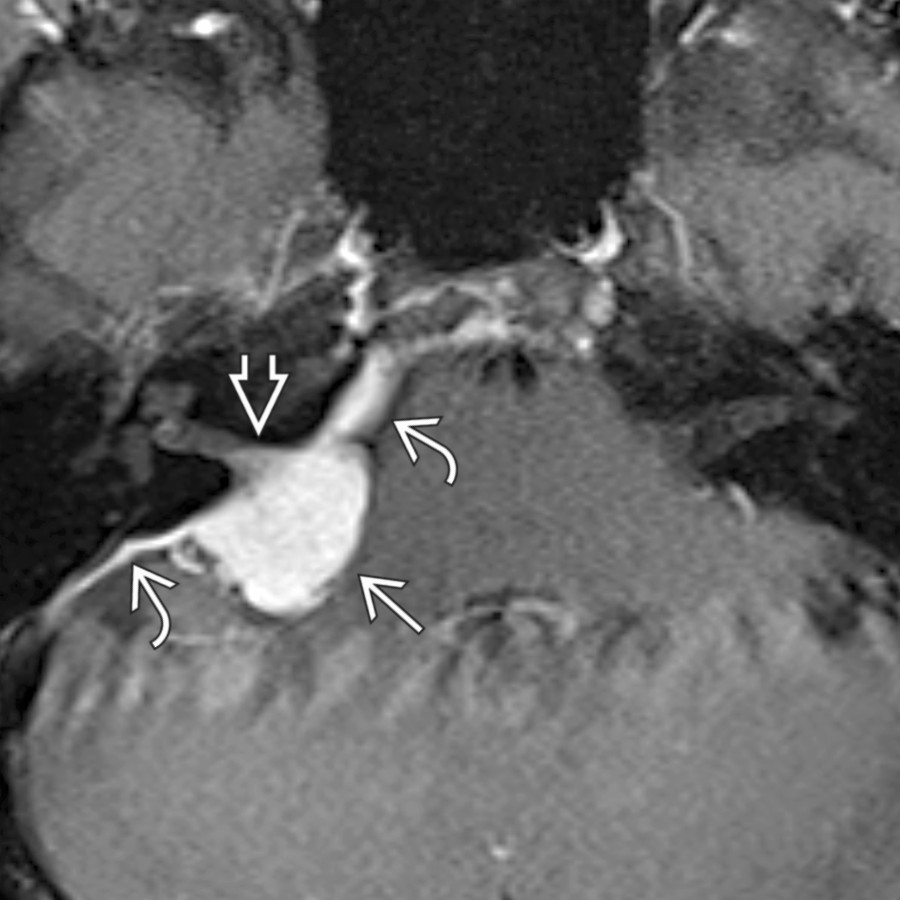
**Vestibular Schwannoma**
*Axial T1 C+ FS MR shows the typical appearance of a CPA-IAC vestibular schwannoma with avid, heterogeneous enhancement. Note tumor growth along the location of the vestibular nerve within the posterior IAC .*
**Vestibular Schwannoma**
*Axial T1 C+ FS MR shows the typical appearance of a CPA-IAC vestibular schwannoma with avid, heterogeneous enhancement. Note tumor growth along the location of the vestibular nerve within the posterior IAC .*

**Vestibular Schwannoma**
*Axial T1 C+ FS MR shows the typical appearance of a CPA-IAC vestibular schwannoma with avid, heterogeneous enhancement. Note tumor growth along the location of the vestibular nerve within the posterior IAC .*

**Vestibular Schwannoma**
*Axial T1 C+ FS MR shows the typical appearance of a CPA-IAC vestibular schwannoma with avid, heterogeneous enhancement. Note tumor growth along the location of the vestibular nerve within the posterior IAC .*
 from microhemorrhage, a feature that can help distinguish CPA-IAC schwannoma from meningioma.](images/app.statdx.com_image_thumbnail_0bd14ef9-fa2b-49f4-a274-290f0a016831_annotated_true_size_900_quality_90_8295787439dc0641cc294b36bcc813f2b7179fbb.jpg)
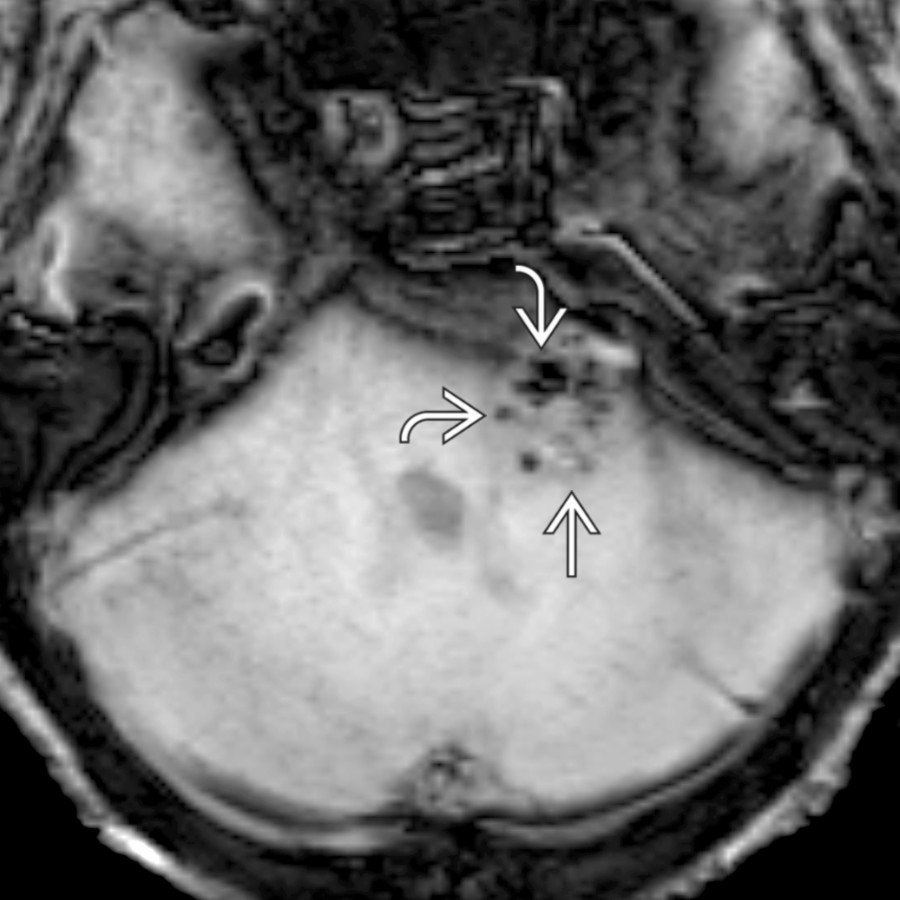
**Vestibular Schwannoma**
*Axial SWI MR in a CPA-IAC vestibular schwannoma shows punctate foci of gradient susceptibility from microhemorrhage, a feature that can help distinguish CPA-IAC schwannoma from meningioma.*
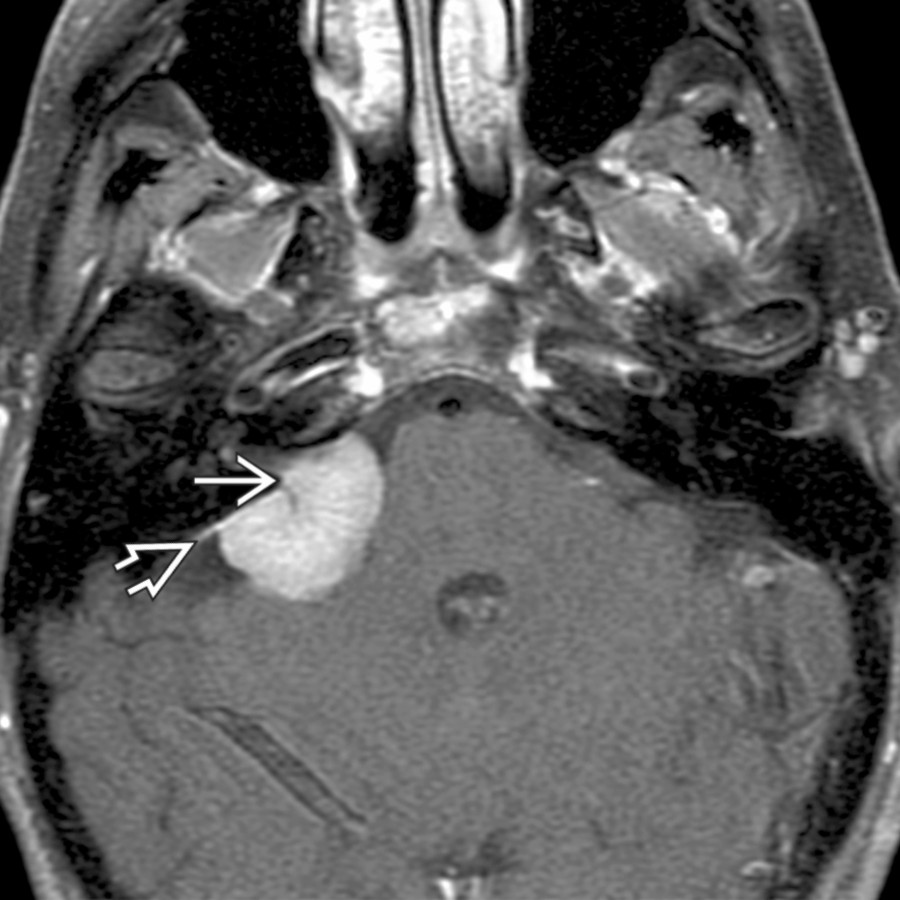
**Meningioma in CPA**
*Axial T1 C+ FS MR shows the typical appearance of a CPA meningioma , which is avidly enhancing and extends into the IAC . Note the characteristic dural tails , which help differentiate meningioma from schwannoma.*

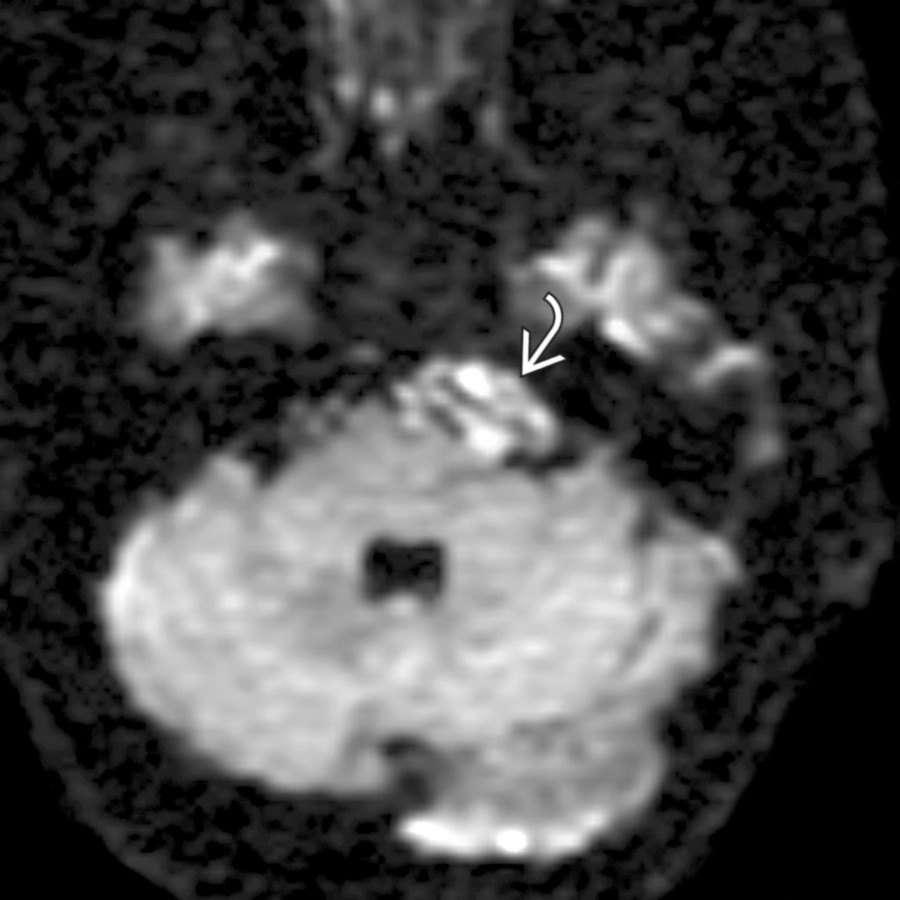
**Epidermoid Cyst in CPA**
*Axial DTI trace image through the posterior fossa shows a typical epidermoid cyst with reduced diffusivity. Note the scalloped, insinuating margins , which frequently encase cranial nerves and vessels and can make surgical resection fraught with peril.*
**Vestibular Schwannoma**
*Axial SWI MR in a CPA-IAC vestibular schwannoma shows punctate foci of gradient susceptibility from microhemorrhage, a feature that can help distinguish CPA-IAC schwannoma from meningioma.*

**Meningioma in CPA**
*Axial T1 C+ FS MR shows the typical appearance of a CPA meningioma , which is avidly enhancing and extends into the IAC . Note the characteristic dural tails , which help differentiate meningioma from schwannoma.*

**Epidermoid Cyst in CPA**
*Axial DTI trace image through the posterior fossa shows a typical epidermoid cyst with reduced diffusivity. Note the scalloped, insinuating margins , which frequently encase cranial nerves and vessels and can make surgical resection fraught with peril.*
 posterolaterally.](images/app.statdx.com_image_thumbnail_0a837932-9add-4268-8d4b-971743940ea0_annotated_true_size_900_quality_90_95859beecf4cdc34a5d2e7593427c4e9d7713a8b.jpg)
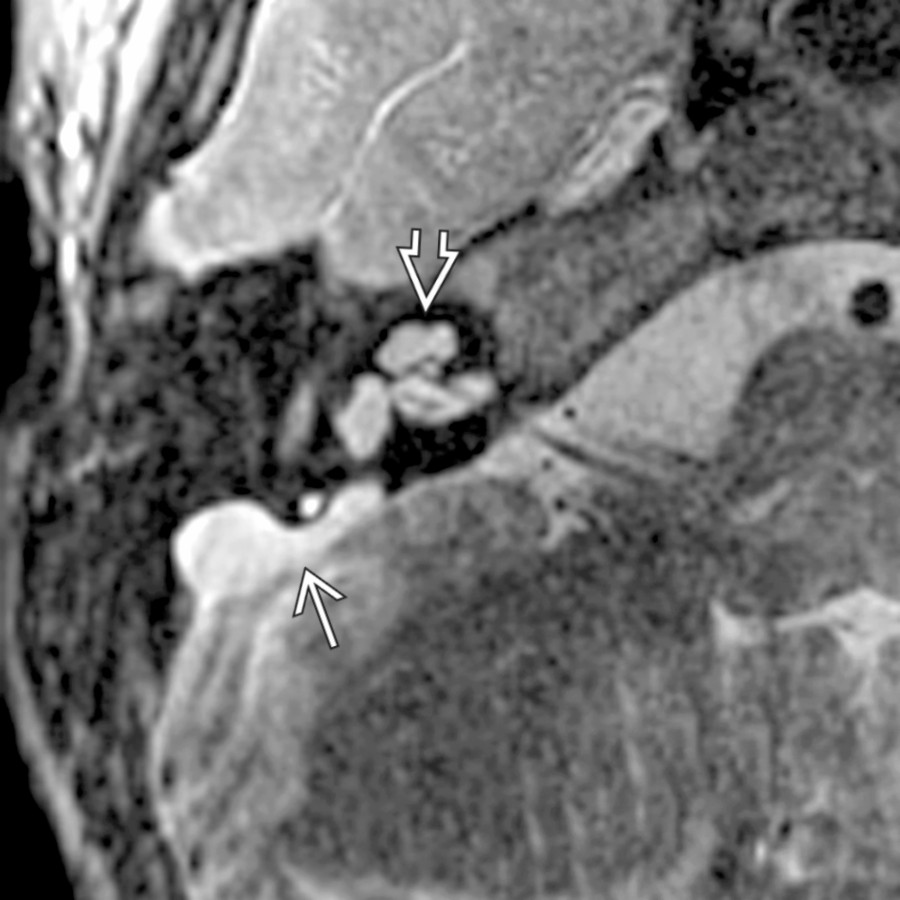
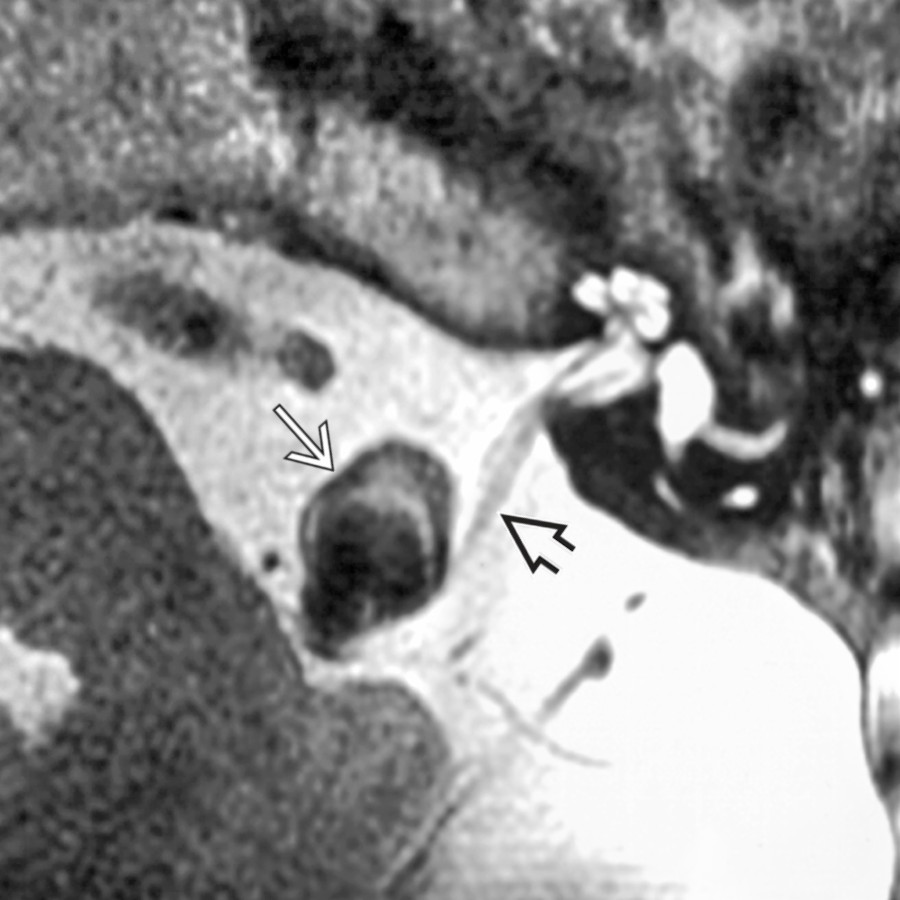
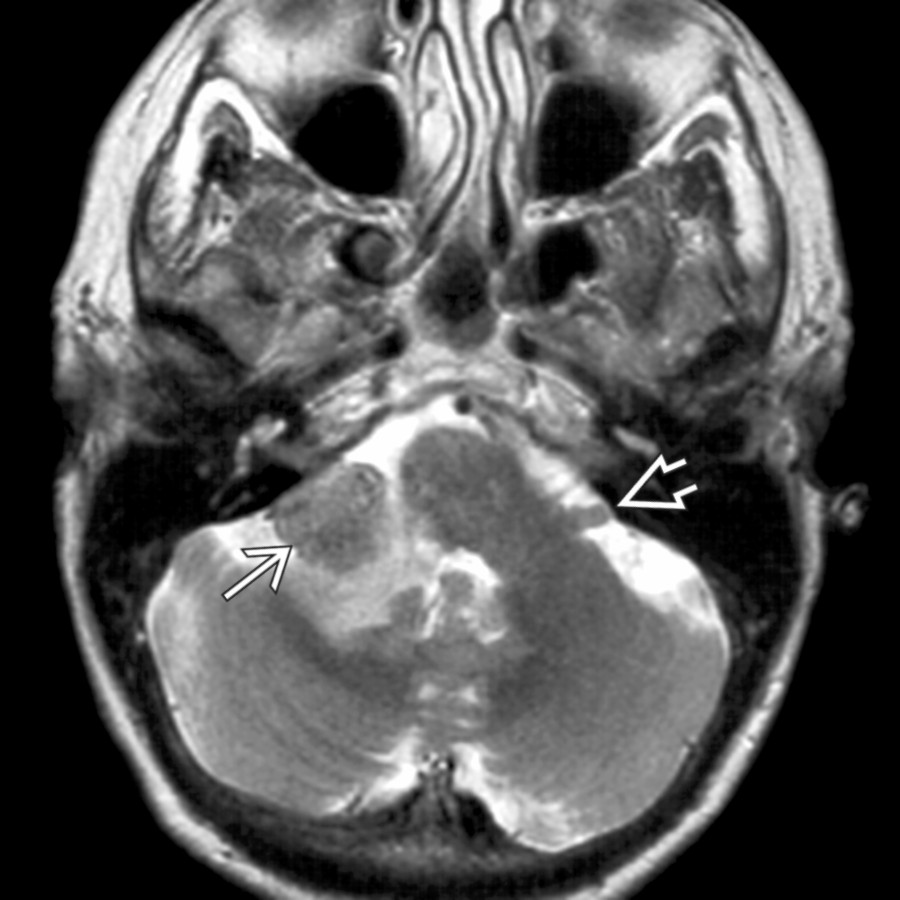
**Aneurysm in CPA**
*Axial T2WI MR shows a CPA vertebral artery aneurysm as an ovoid mass with complex wall signal, which bows the vestibulocochlear nerve posterolaterally.*
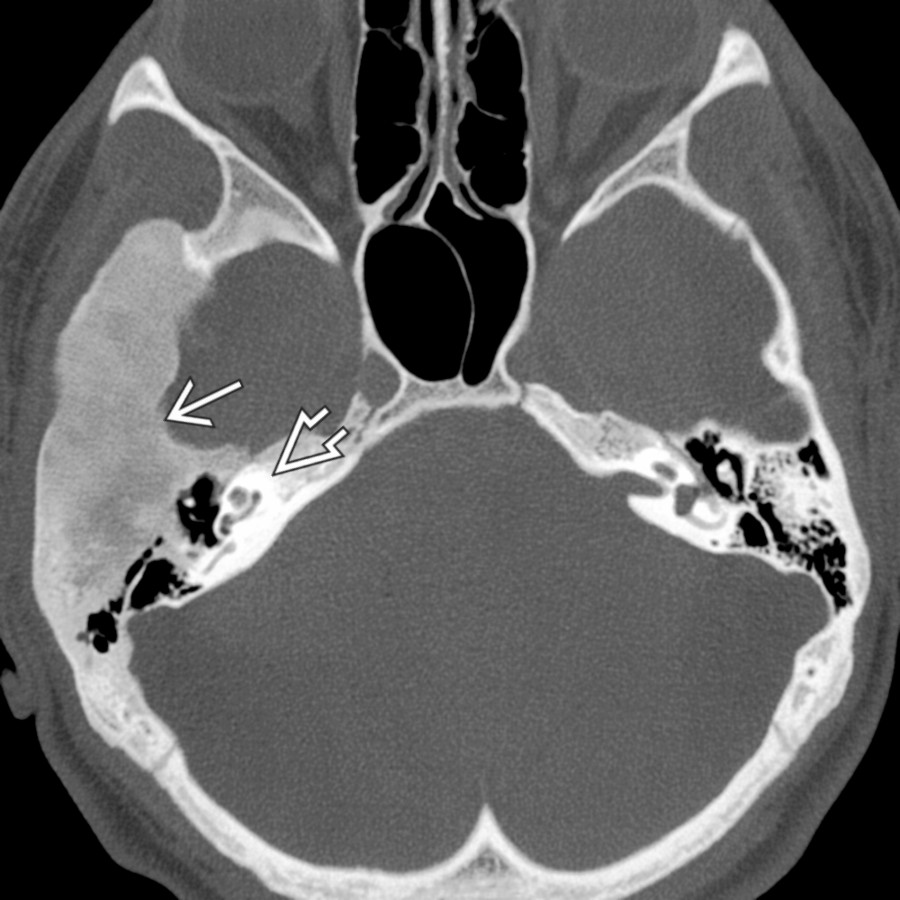
**T-Bone Fracture**
*Axial bone CT shows a complex, transversely oriented T-bone fracture that involves the otic capsule and disrupts the cochlea . The mastoid air cells and middle ear are opacified with blood, corresponding with hemotympanum on otoscopy.*
**Cochlear Otosclerosis**
*Axial bone CT shows cochlear otosclerosis yielding SNHL. Note confluent otic capsule lucency adjacent to the cochlea. Patients commonly have fenestral involvement with lucency near the fissula ante fenestram , contributing a conductive component to hearing loss. Note the prior partial ossicular replacement prosthesis .*
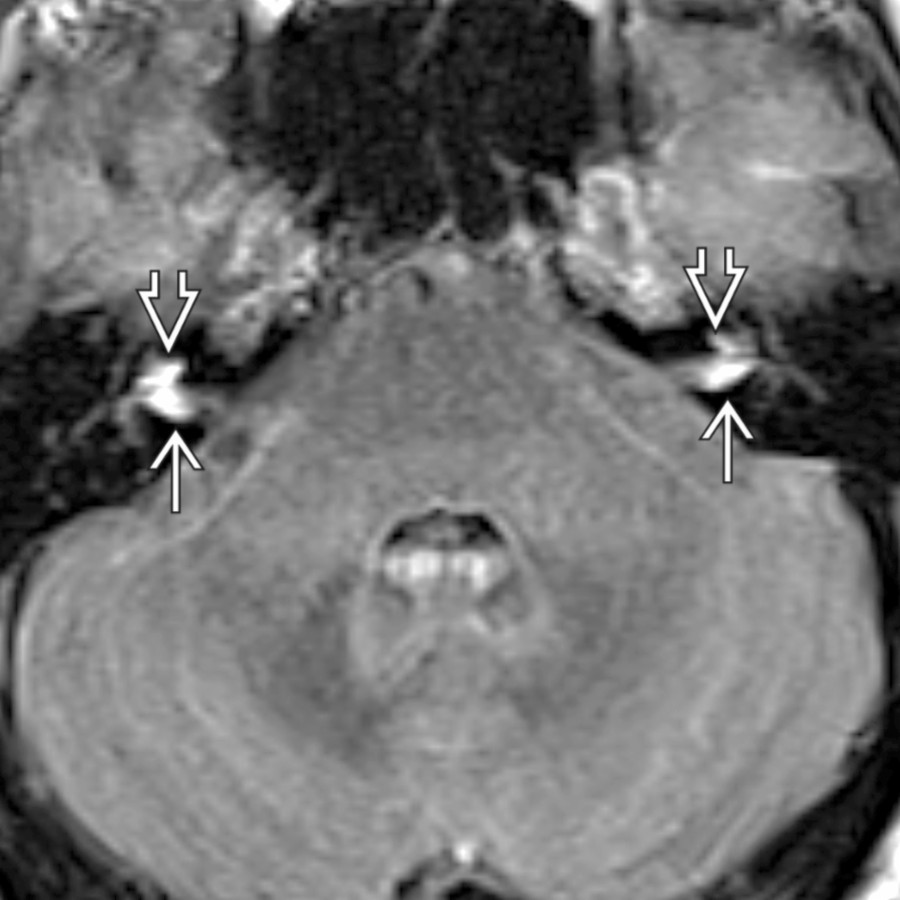
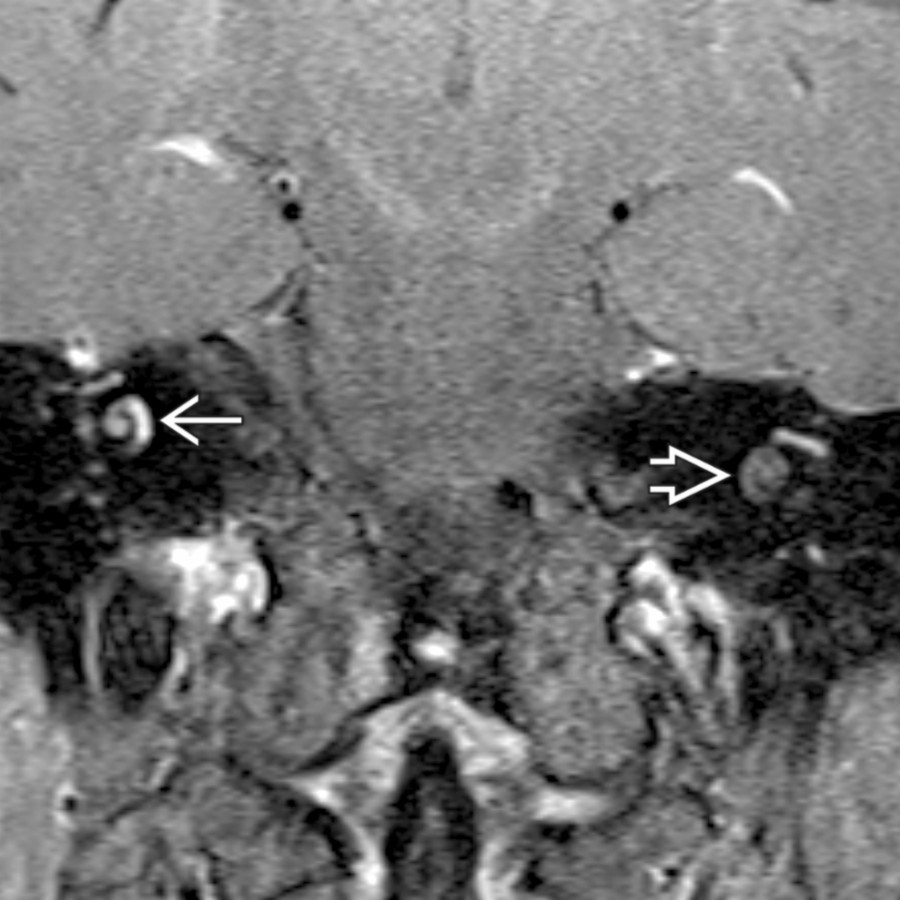
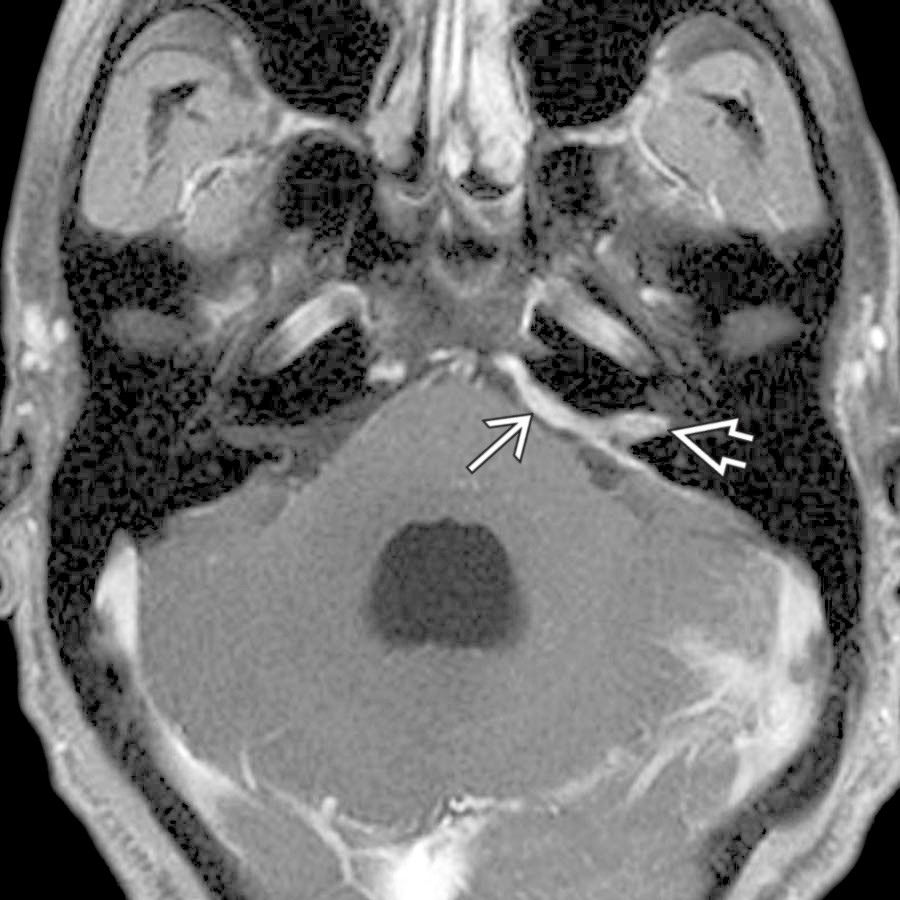
**Metastases in CPA-IAC**
*Axial FLAIR C+ MR shows leptomeningeal metastases from melanoma with enhancement at the fundus of bilateral IACs extending into the basal turn of the cochlea bilaterally.*

**Facial Nerve Schwannoma in CPA-IAC**
*Axial T1 C+ SPGR MR shows a facial nerve schwannoma involving the left CPA-IAC. In this case, the labyrinthine tail of enhancement extends to the asymmetrically enhancing geniculate ganglion region , following the expected course of the facial nerve.*

**Lipoma in CPA-IAC**
*Coronal T1 MR of a left CPA-IAC lipoma shows a T1-bright lobular mass extending into the IAC . The presence of chemical shift artifact at the tumor-CSF (i.e., water) margin confirms the presence of fat within this mass.*
**Large Endolymphatic Sac Anomaly (IP-2)**
*Axial T2WI FS MR shows a large endolymphatic sac along the posterior wall of the T-bone associated with a malformed cochlea (modiolar deficiency, incomplete apical septation, and bulbous apical turn) .*
**Intralabyrinthine Schwannoma**
*Coronal T1 C+ FS MR of an intracochlear schwannoma shows abnormal enhancement in the middle turn of the right cochlea . Note the normal postcontrast appearance of the contralateral cochlea for comparison .*
**Aneurysm in CPA**
*Axial T2WI MR shows a CPA vertebral artery aneurysm as an ovoid mass with complex wall signal, which bows the vestibulocochlear nerve posterolaterally.*

**T-Bone Fracture**
*Axial bone CT shows a complex, transversely oriented T-bone fracture that involves the otic capsule and disrupts the cochlea . The mastoid air cells and middle ear are opacified with blood, corresponding with hemotympanum on otoscopy.*

**Cochlear Otosclerosis**
*Axial bone CT shows cochlear otosclerosis yielding SNHL. Note confluent otic capsule lucency adjacent to the cochlea. Patients commonly have fenestral involvement with lucency near the fissula ante fenestram , contributing a conductive component to hearing loss. Note the prior partial ossicular replacement prosthesis .*

**Metastases in CPA-IAC**
*Axial FLAIR C+ MR shows leptomeningeal metastases from melanoma with enhancement at the fundus of bilateral IACs extending into the basal turn of the cochlea bilaterally.*

**Facial Nerve Schwannoma in CPA-IAC**
*Axial T1 C+ SPGR MR shows a facial nerve schwannoma involving the left CPA-IAC. In this case, the labyrinthine tail of enhancement extends to the asymmetrically enhancing geniculate ganglion region , following the expected course of the facial nerve.*

**Lipoma in CPA-IAC**
*Coronal T1 MR of a left CPA-IAC lipoma shows a T1-bright lobular mass extending into the IAC . The presence of chemical shift artifact at the tumor-CSF (i.e., water) margin confirms the presence of fat within this mass.*

**Large Endolymphatic Sac Anomaly (IP-2)**
*Axial T2WI FS MR shows a large endolymphatic sac along the posterior wall of the T-bone associated with a malformed cochlea (modiolar deficiency, incomplete apical septation, and bulbous apical turn) .*

**Intralabyrinthine Schwannoma**
*Coronal T1 C+ FS MR of an intracochlear schwannoma shows abnormal enhancement in the middle turn of the right cochlea . Note the normal postcontrast appearance of the contralateral cochlea for comparison .*
 due to marked inflammation.](images/app.statdx.com_image_thumbnail_339d6bcb-3739-4e06-8be4-a945b3e4d948_annotated_true_size_900_quality_90_2dcc16a8e0232f44a5755936e65bd2492e198879.jpg)
**Labyrinthitis**
*Axial T1 C+ FS MR in a patient with acute otomastoiditis complicated by labyrinthitis shows enhancement in the cochlea . There is additional vestibulocochlear neuritis with linear enhancement at the IAC fundus . Note enhancing mastoid/middle ear disease and dural enhancement due to marked inflammation.*
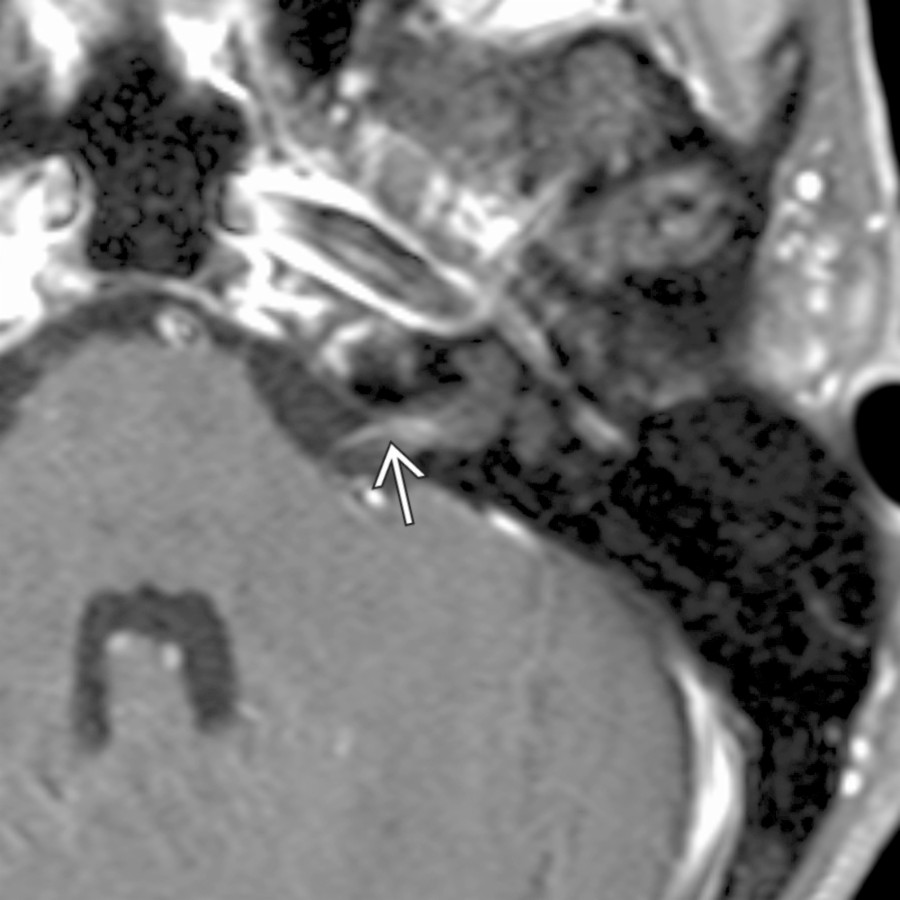
**Vestibulocochlear Neuritis**
*Axial T1 C+ FS MR shows vestibulocochlear neuritis in a patient with rapid onset of sensorineural hearing loss. Note the area of linear enhancement in the proximal IAC .*
### Additional Images
**Fibrous Dysplasia in T-Bone**
*Axial bone CT shows expansile ground-glass density focus of fibrous dysplasia affecting the squamous, tympanic, & mastoid portions of the T-bone. Note relative sparing of the otic capsule .*

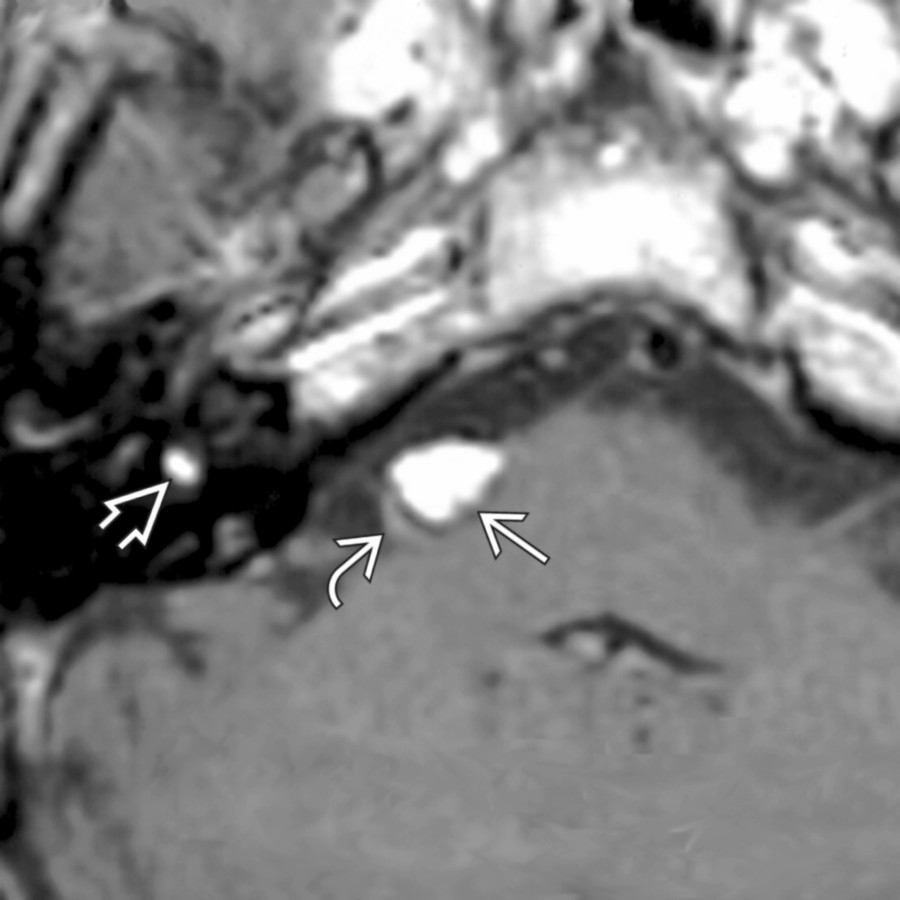
**Endolymphatic Sac Tumor**
*Axial T1WI MR reveals a tumor along the posterior wall of the T-bone with high-signal foci that is highly suggestive of an endolymphatic sac tumor.*
**Sarcoidosis in CPA**
*Axial T1 C+ FS MR demonstrates thick enhancing dural-based sarcoidosis in the left CPA and IAC mimicking en plaque meningioma.*

**Superficial Siderosis in CPA-IAC**
*Axial T2* GRE MR shows superficial siderosis on the surface of the posterior fossa structures (linear low signal), including cerebellar folia , flocculi , and vestibulocochlear nerves .*

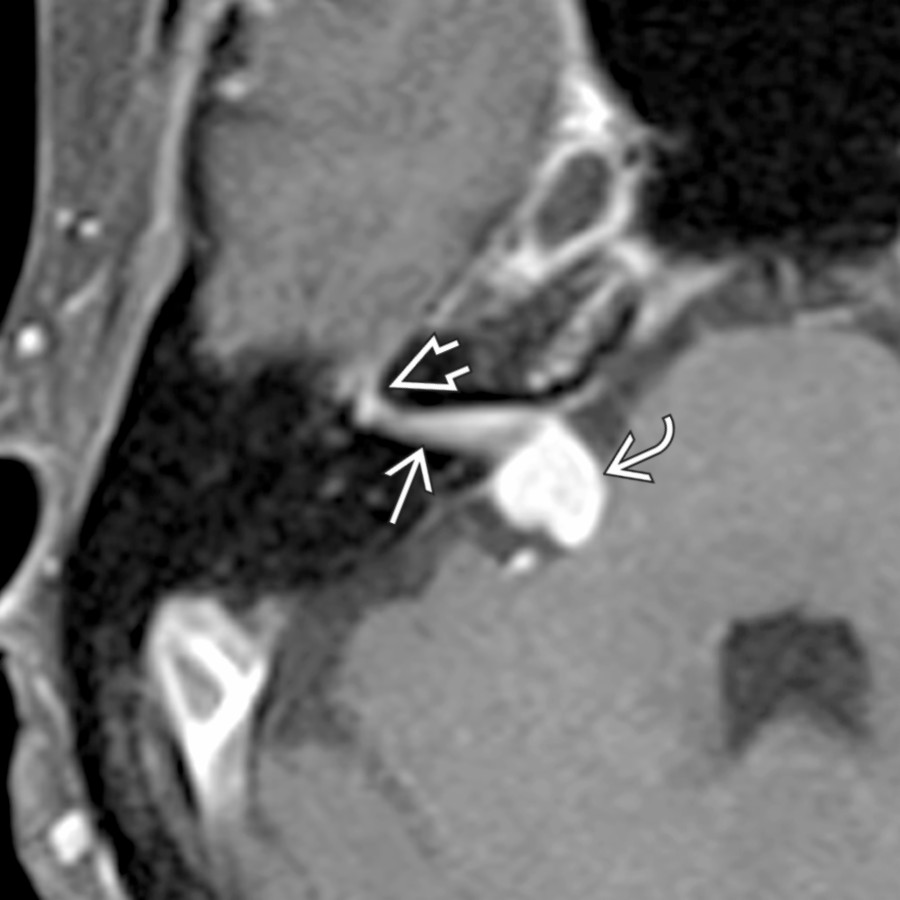
**IAC/Temporal Bone Facial Nerve Venous Malformation ("Hemangioma")**
*Axial bone CT reveals punctate calcifications in the IAC suggesting the diagnosis of IAC hemangioma. Enhanced MR showed an enhancing mass in this location.*

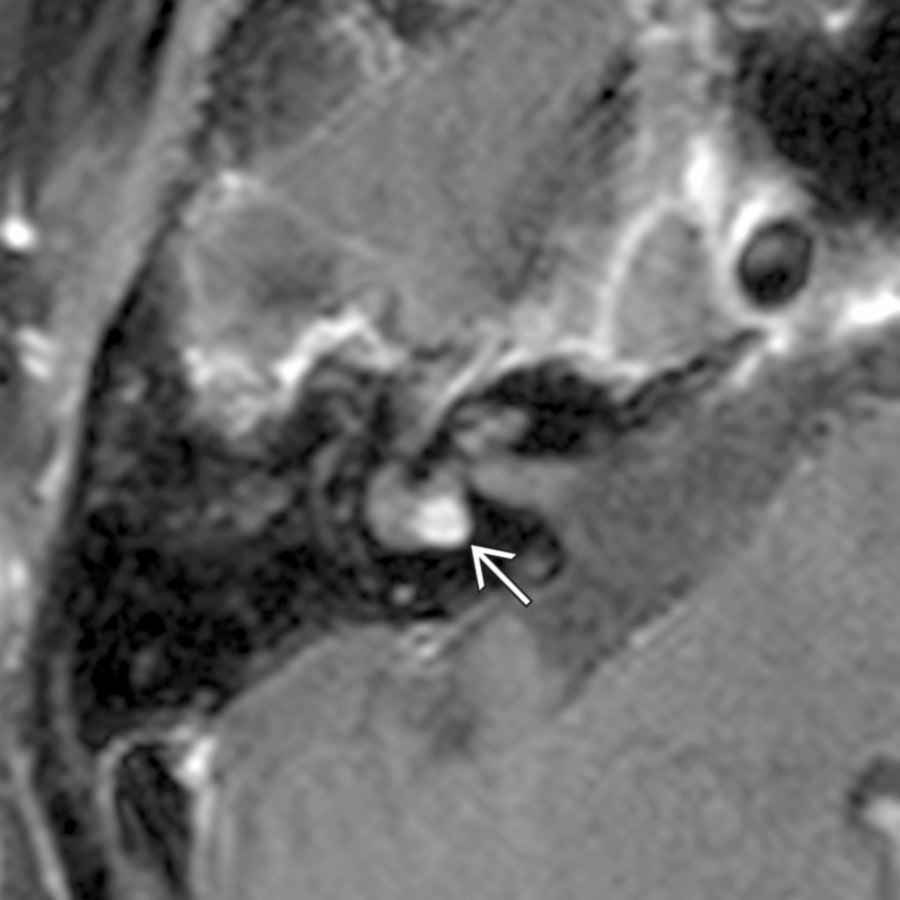
**Ramsay Hunt Syndrome**
*Axial T1 C+ MR shows area of crescentic enhancement in the IAC fundus associated with tympanic segment of the facial nerve asymmetric enhancement . EAC vesicles were present, characteristic of Ramsey Hunt syndrome.*
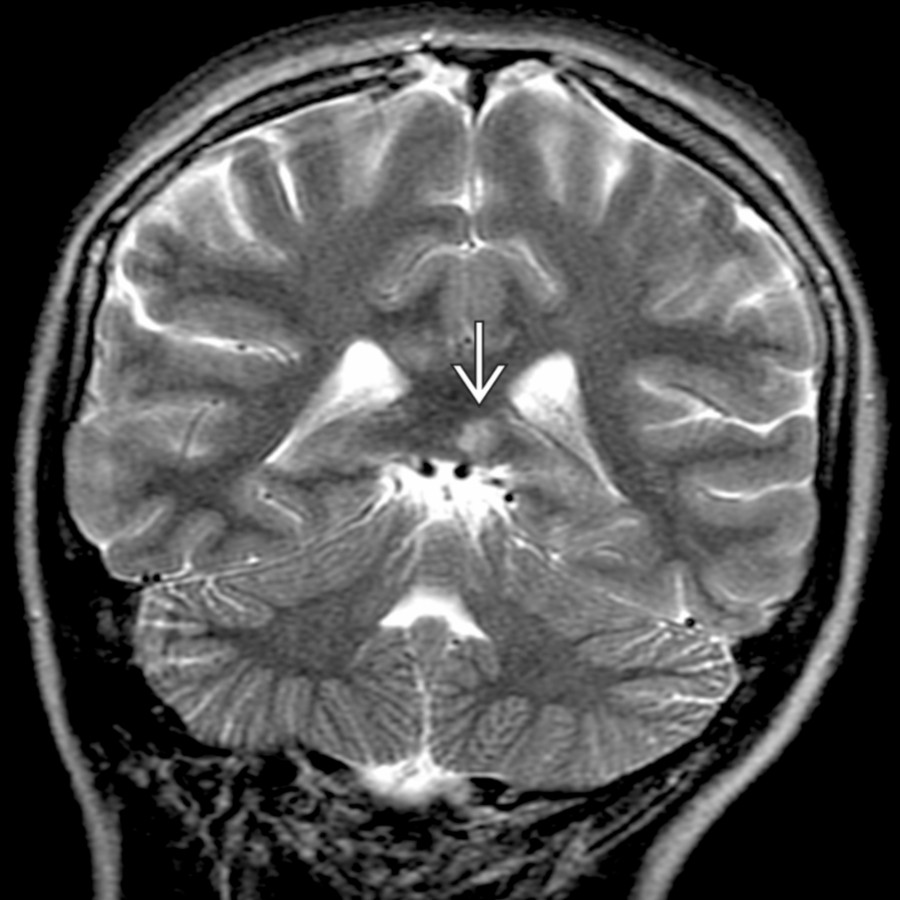
**Susac Syndrome (Retinocochleocerebral Vasculopathy)**
*Coronal T2 FS MR in a patient with retinocochleocerebral vasculopathy (Susac syndrome) shows a characteristic round, hyperintense lesion in the splenium of the corpus callosum .*

**Vestibular Schwannoma**
*Axial T1 C+ FS MR shows typical mid sized CPA-IAC vestibular schwannoma. "Ice cream" (CPA component) "on cone" (IAC component) morphology is highly suggestive of this diagnosis.*
**Meningioma in CPA**
*Axial T1 C+ FS MR shows the sessile morphology of meningioma as it "sits" on the posterior T-bone wall. Note the characteristic dural tail and dural artery feeding the tumor center.*
**Epidermoid Cyst in CPA**
*Axial DWI MR shows a CPA epidermoid identified by its reduced diffusivity . CPA epidermoids often are not directly over the porus acusticus, as in this case.*

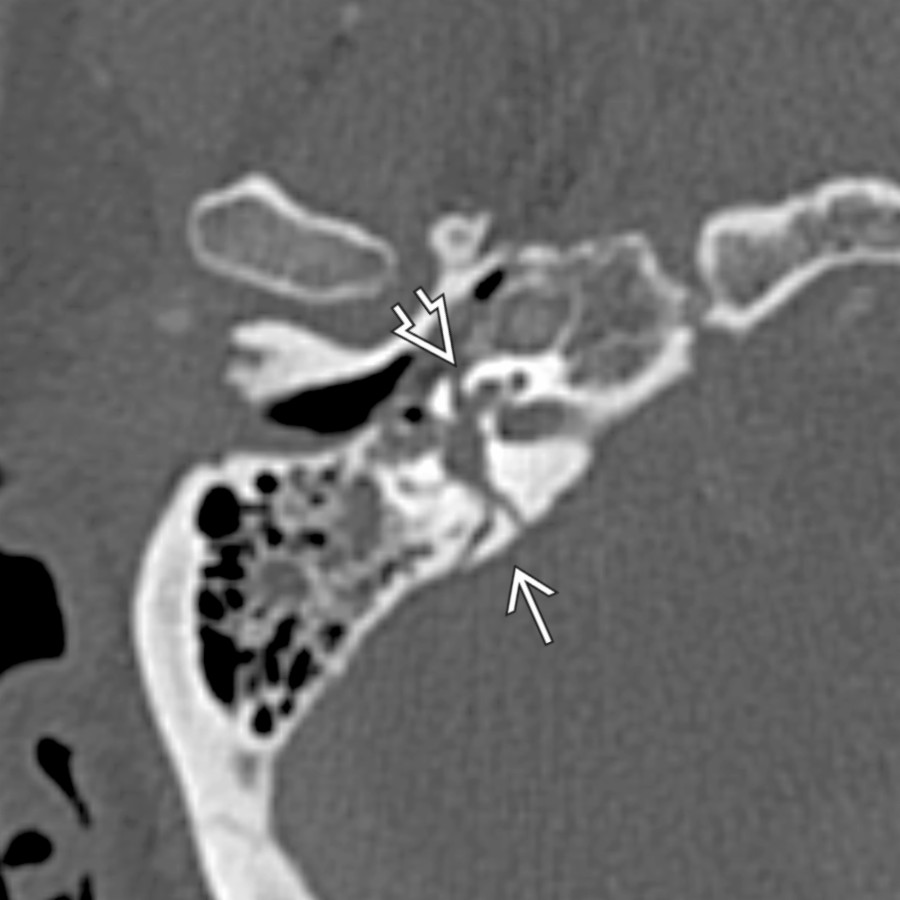
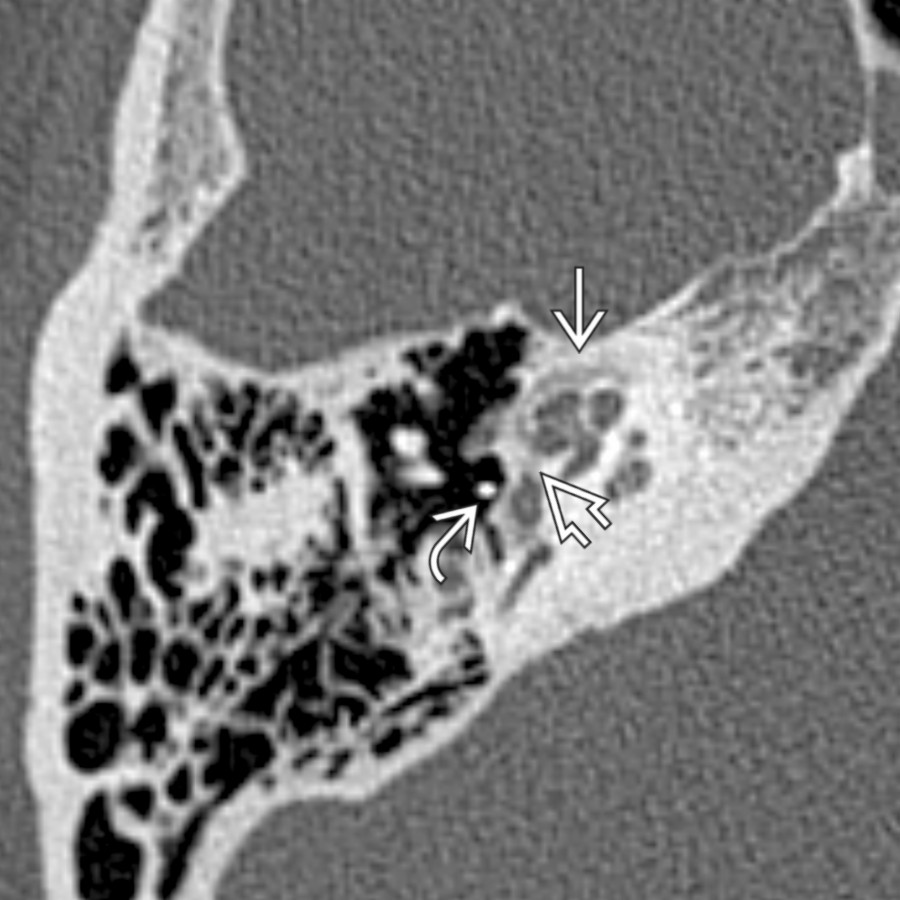
**T-Bone Fracture**
*Axial bone CT shows an oblique T-bone fracture traversing the oval window and extending to the IAC area . Notice the air bubble (pneumolabyrinth) along the anterior margin of the vestibule .*

**Cochlear Otosclerosis**
*Axial bone CT shows severe otosclerosis as radiolucent foci along the medial middle ear wall (fenestral otosclerosis) and within the bony labyrinth (cochlear otosclerosis).*
**Metastases in CPA-IAC**
*Axial T2WI MR demonstrates a right floccular metastasis with associated high-signal cerebellar and brachium pontis edema. A normal left flocculus is also seen.*
**Facial Nerve Schwannoma in CPA-IAC**
*Axial T1 C+ FS MR reveals an enhancing facial nerve schwannoma traversing the CPA and IAC into the facial nerve labyrinthine segment . This labyrinthine tail is characteristic.*
**Lipoma in CPA-IAC**
*Axial T1 MR demonstrates a CPA and intravestibular lipoma. Notice that the CPA lipoma effaces the most proximal vestibulocochlear nerve bundle . These lesions are left alone.*
**Intralabyrinthine Schwannoma**
*Axial T1 C+ FS MR demonstrates a nodule of enhancing tissue in the vestibule of the inner ear secondary to intralabyrinthine schwannoma. CT of the T-bone was normal.*

**Paget Disease in T-Bone**
*Axial bone CT shows late-phase Paget disease with diffuse bony expansion with areas of demineralization . Notice that the bony labyrinth along the anterior cochlear surface is involved .*

**Labyrinthitis**
*Axial T1 C+ FS MR shows enhancement of the middle ear , inner ear membranous labyrinth , and IAC in this pediatric patient with acute actinomycosis.*
due to marked inflammation.](images/app.statdx.com_image_thumbnail_339d6bcb-3739-4e06-8be4-a945b3e4d948_annotated_true_size_900_quality_90_2dcc16a8e0232f44a5755936e65bd2492e198879.jpg)
**Labyrinthitis**
*Axial T1 C+ FS MR in a patient with acute otomastoiditis complicated by labyrinthitis shows enhancement in the cochlea . There is additional vestibulocochlear neuritis with linear enhancement at the IAC fundus . Note enhancing mastoid/middle ear disease and dural enhancement due to marked inflammation.*

**Vestibulocochlear Neuritis**
*Axial T1 C+ FS MR shows vestibulocochlear neuritis in a patient with rapid onset of sensorineural hearing loss. Note the area of linear enhancement in the proximal IAC .*
### Additional Images

**Fibrous Dysplasia in T-Bone**
*Axial bone CT shows expansile ground-glass density focus of fibrous dysplasia affecting the squamous, tympanic, & mastoid portions of the T-bone. Note relative sparing of the otic capsule .*

**Endolymphatic Sac Tumor**
*Axial T1WI MR reveals a tumor along the posterior wall of the T-bone with high-signal foci that is highly suggestive of an endolymphatic sac tumor.*

**Sarcoidosis in CPA**
*Axial T1 C+ FS MR demonstrates thick enhancing dural-based sarcoidosis in the left CPA and IAC mimicking en plaque meningioma.*

**Superficial Siderosis in CPA-IAC**
*Axial T2* GRE MR shows superficial siderosis on the surface of the posterior fossa structures (linear low signal), including cerebellar folia , flocculi , and vestibulocochlear nerves .*

**IAC/Temporal Bone Facial Nerve Venous Malformation ("Hemangioma")**
*Axial bone CT reveals punctate calcifications in the IAC suggesting the diagnosis of IAC hemangioma. Enhanced MR showed an enhancing mass in this location.*

**Ramsay Hunt Syndrome**
*Axial T1 C+ MR shows area of crescentic enhancement in the IAC fundus associated with tympanic segment of the facial nerve asymmetric enhancement . EAC vesicles were present, characteristic of Ramsey Hunt syndrome.*

**Susac Syndrome (Retinocochleocerebral Vasculopathy)**
*Coronal T2 FS MR in a patient with retinocochleocerebral vasculopathy (Susac syndrome) shows a characteristic round, hyperintense lesion in the splenium of the corpus callosum .*

**Vestibular Schwannoma**
*Axial T1 C+ FS MR shows typical mid sized CPA-IAC vestibular schwannoma. "Ice cream" (CPA component) "on cone" (IAC component) morphology is highly suggestive of this diagnosis.*

**Meningioma in CPA**
*Axial T1 C+ FS MR shows the sessile morphology of meningioma as it "sits" on the posterior T-bone wall. Note the characteristic dural tail and dural artery feeding the tumor center.*

**Epidermoid Cyst in CPA**
*Axial DWI MR shows a CPA epidermoid identified by its reduced diffusivity . CPA epidermoids often are not directly over the porus acusticus, as in this case.*

**T-Bone Fracture**
*Axial bone CT shows an oblique T-bone fracture traversing the oval window and extending to the IAC area . Notice the air bubble (pneumolabyrinth) along the anterior margin of the vestibule .*

**Cochlear Otosclerosis**
*Axial bone CT shows severe otosclerosis as radiolucent foci along the medial middle ear wall (fenestral otosclerosis) and within the bony labyrinth (cochlear otosclerosis).*

**Metastases in CPA-IAC**
*Axial T2WI MR demonstrates a right floccular metastasis with associated high-signal cerebellar and brachium pontis edema. A normal left flocculus is also seen.*

**Facial Nerve Schwannoma in CPA-IAC**
*Axial T1 C+ FS MR reveals an enhancing facial nerve schwannoma traversing the CPA and IAC into the facial nerve labyrinthine segment . This labyrinthine tail is characteristic.*

**Lipoma in CPA-IAC**
*Axial T1 MR demonstrates a CPA and intravestibular lipoma. Notice that the CPA lipoma effaces the most proximal vestibulocochlear nerve bundle . These lesions are left alone.*

**Intralabyrinthine Schwannoma**
*Axial T1 C+ FS MR demonstrates a nodule of enhancing tissue in the vestibule of the inner ear secondary to intralabyrinthine schwannoma. CT of the T-bone was normal.*

**Paget Disease in T-Bone**
*Axial bone CT shows late-phase Paget disease with diffuse bony expansion with areas of demineralization . Notice that the bony labyrinth along the anterior cochlear surface is involved .*

**Labyrinthitis**
*Axial T1 C+ FS MR shows enhancement of the middle ear , inner ear membranous labyrinth , and IAC in this pediatric patient with acute actinomycosis.*