---
title: "Stroke Therapy"
docid: "eecb2d0f-ef14-44df-be8e-137567226412"
authors:
- key: "bccfc1a3-a6b8-4707-b2bf-589d9650f769"
value: "Jared Halpin, MD"
- key: "8fe1db5b-d23b-459d-9ab0-0cba2c16a0ac"
value: "Coleman O. Martin, MD"
breadcrumbs:
-
name: "Interventional Radiology"
slug: "interventional-radiology"
treeNodeId: "20225e4f-e0f0-447f-8bfc-151c06ebe73f"
-
name: "Procedures"
slug: "procedures"
treeNodeId: "4f9c2b36-60f0-40e8-8cfc-c1482c9f1ed0"
-
name: "Arterial Procedures"
slug: "arterial-procedures"
treeNodeId: "b554f24b-18b5-4e89-8f22-d22849ead8e7"
-
name: "Cranial Revascularization"
slug: "cranial-revascularization"
treeNodeId: "9c47d8e4-b6c5-4251-93f0-1f0554c79fd4"
-
name: "Stroke Therapy"
slug: "stroke-therapy"
treeNodeId: null
category: "Interventional Radiology"
cmeTopicId: "f63224f3-1455-4b82-a813-021294fdd3ad"
documentVersionId: "44037350-bdbf-46ea-91e6-1a6faa35f508"
imageCount: 36
lastUpdated: "05/13/22"
pageDescription: "Stroke Therapy"
pageKeywords: "Interventional Radiology, Procedures, Arterial Procedures, Cranial Revascularization, Stroke Therapy"
pageTitle: "Stroke Therapy | STATdx"
enhancedTitle: "Stroke Therapy"
type: "PROCEDURE"
references: true
breadcrumbs:
- "Interventional Radiology"
- "Procedures"
- "Arterial Procedures"
- "Cranial Revascularization"
- "Stroke Therapy"
---
# KEY FACTS
- ## Terminology
- **Stroke**: Rapidly developing loss of brain function(s) due to disturbance in blood supply to brain
- **Core infarct**: Central area of severe ischemia/evolving infarction; unlikely to respond to treatment
- **Ischemic penumbra**: Surrounding ischemic tissue rim between normally perfused brain and evolving infarction
- ## Preprocedure
- Noncontrast head CT: Exclude hemorrhage, evaluate extent of core infarct [Alberta Stroke Program Early CT Score (ASPECTS)]
- CTA head/neck ± CT head perfusion: Localize arterial occlusion, detection of penumbra
- Thrombectomy inclusion criteria
- Large vessel occlusion; symptoms ≤ 6-8 hours
- Significant neurologic symptoms [National Institute of Health Stroke Scale (NIHSS) > 4]
- Minimal ischemic burden (ASPECTS ≥ 6)
- Salvageable tissue by perfusion imaging
- Absolute contraindication: Hemorrhage/well-established acute infarct involving > 1/3 of affected vascular territory
- ## Procedure
- Thrombectomy with stent retriever
- Placement of balloon guide catheter in internal carotid artery (ICA) or subclavian artery
- Deploy stent retriever device across thrombus, wait 5 min
- Balloon occlusion of ICA/subclavian while retracting device and thrombus into guide catheter
- Aspiration thrombectomy, angioplasty ± stenting, intraarterial thrombolysis as backup in select cases
- ## Post Procedure
- Successful recanalization: 72-93%
- Good clinical outcome: 51-60%
- Intracerebral hemorrhage: 3.6%
# TERMINOLOGY
- ## Definitions
- **Stroke**: Acute loss of brain function(s) due to disturbance in blood supply to brain
- Ischemic stroke: Embolic or thrombotic occlusion of arterial supply to brain (80% of strokes)
- 3 major clinical ischemic stroke subtypes
- Large artery/atherosclerotic strokes (40-50%)
- Cardioembolic disease (20-25%)
- Lacunar infarction (20-30%)
- Hemorrhagic stroke: Rupture/bleeding from brain blood vessel (15% of strokes)
- Nontraumatic subarachnoid hemorrhage (5%)
- Vasculitis
- Venous infarction (< 1%)
- **Core infarct**: Central area of severe ischemia/evolving infarction; unlikely to respond to treatment
- Severely reduced to almost nonexistent blood flow
- Inadequate supply of oxygen and glucose
- Neuronal and glial necrosis
- Irreversible damage; no response to reperfusion
- **Ischemic penumbra**: Surrounding rim of ischemic tissue between normally perfused tissue and area of evolving infarction
- Parenchymal tissue at risk of eventual infarction
- Dependent upon collateral perfusion
- Collateral circulation inadequate to maintain neuronal oxygen/glucose demand indefinitely
- May remain viable for several hours
- Target of acute stroke intervention
- **Endovascular therapy (ET)**: Standard of care for acute ischemic stroke with emergent large vessel occlusion (ELVO)
- Potential reperfusion techniques
- Intravenous (IV) thrombolysis [IV tissue plasminogen activator (tPA)]
- Mechanical thrombectomy (stent retriever, aspiration catheter)
- Balloon angioplasty/stenting
- Intraarterial (IA) thrombolysis
- **Stroke-related scales/grades**
- **National Institute of Health Stroke Scale (NIHSS)**
- Clinical assessment tool used to quantify neurologic impairment caused by acute stroke
- Predictor of short- and long-term outcome
# PREPROCEDURE
- ## Indications
- **IV tPA**
- Patients with acute neurologic deficit expected to result in long-term disability
- NECT shows no hemorrhage and no large infarct
- Clearly defined onset time (last known well time) and presentation within 3-4.5 hours of symptom onset
- No contraindication to tPA
- **ET**
- Patients with large vessel occlusions documented by CTA, DSA, or MRA
- Anterior circulation: When revascularization is feasible within 6-8 hours of symptom onset
- Posterior circulation: Time window undefined but within ≤ 12-24 hours of symptom onset
- NIHSS > 4, exceptions for cases of isolated aphasia or hemianopsia
- No large infarct on NECT [Alberta Stroke Program Early CT Score (ASPECTS) ≥ 6]
- Significant area of salvageable tissue seen on perfusion imaging
- ## Contraindications
- **Absolute contraindications to ET**
- Intracranial hemorrhage (ICH)
- Established acute infarct involving > 1/3 of affected vascular territory
- ASPECTS ≤ 5 has greater risk of hemorrhage
- CNS lesion with elevated likelihood of hemorrhage during revascularization
- Abscess
- Aneurysm
- Brain tumor
- Established bacterial endocarditis
- **Relative contraindications (general)**
- Mild or rapidly improving deficits
- Stroke or ICH in same territory within 3 months
- Suspected bacterial endocarditis
- Life expectancy < 1 year from other causes
- ## Preprocedure Imaging
- **Noncontrast head CT**
- Exclude ICH
- Look for established infarct (frank hypodensity)
- Calculate ASPECT score
- 10-point grading scale for severity of middle cerebral artery (MCA) stroke on NECT
- 1 point deducted from initial score of 10 for every region involved
- Caudate, putamen, internal capsule, insular cortex, and 6 regions of MCA cortex (3 superior, 3 inferior)
- **CTA head and neck**
- Localize site of arterial occlusion(s) or stenosis
- Evaluate for vascular tortuosity or variant vascular anatomy
- **CT head perfusion**
- Mean transit time
- Average blood transit time through brain region
- Highly sensitive parameter for detection of brain tissue oligemia
- Time to peak/TMax
- Time to peak density of contrast through brain region
- Highly sensitive parameter for detection of brain tissue oligemia
- Cerebral blood flow (CBF)
- Blood volume moving through brain
- Reasonable marker for extent of impending infarction
- Cerebral blood volume (CBV)
- Total blood volume in given unit volume of brain
- Reasonable marker for core infarct
- Larger core infarct is marker for poor outcome
- CBF/CBV mismatch defines extent of penumbra
- **MR diffusion (DWI) and MR perfusion (PWI) imaging**
- Added screening time and scan time limits usefulness in emergent stroke evaluation
- DWI most reliable estimate of core infarct
- DWI/PWI mismatch defines extent of penumbra
- Helpful in basilar distribution stroke where CT perfusion is less accurate
- ## Getting Started
- Things to check
- Focused clinical history/physical examination
- Pinpoint time of onset of stroke symptoms
- If symptoms present upon awakening, consider onset as when patient was last symptom free
- Obtain NIHSS
- Assess thrombolysis inclusion vs. exclusion
- Exclude conditions that mimic stroke (e.g., seizure, toxic/metabolic syndromes, hypoglycemia, tumor)
- Allergies to sedatives, contrast
- Current medications, including any anticoagulants
- Laboratory parameters
- Electrolytes, estimated glomerular filtration rate (eGFR)
- CBC
- Platelet count > 50,000/μL
- Coagulation profile
- Consent for procedure
- Discuss risk of hemorrhagic stroke, vascular injury, allergic reaction, renal failure, access site hematoma
- ### Medications
- IV tPA****
- Infuse 0.9 mg/kg (maximum 90 mg) over 60 minutes; bolus first 10% of dose over 1 minute
- Maintain systolic blood pressure (SBP) < 180 mm Hg; diastolic blood pressure (DBP) < 105 mm Hg
- If new severe headache, acute hypertension, or nausea, obtain head CT
- Acceptable to stop infusion to perform thrombectomy or continue infusion during thrombectomy
- Patient management after thrombolysis
- No anticoagulation/antiplatelet therapy for 24 hours
- Procedural sedation
- Usually performed without sedation or with light sedation using fentanyl and midazolam if needed
- Use of general anesthesia is associated with worse neurologic outcomes
- Posterior circulation stroke may require airway support
- ### Equipment list
- Sheaths/guide catheters
- Various proprietary designs
- Femoral arterial sheath
- Balloon guide catheter for flow arrest during withdrawal of thrombus
- Guidewires
- Hydrophilic 0.035" or 0.038" guidewire
- Microwire for use with appropriate microcatheter
- Equipment for mechanical thrombectomy
- Stent retrievers for ensnaring and withdrawing thrombus
- Reperfusion catheters for local aspiration of thrombus
- May do combined stent retriever, local aspiration, and balloon guide technique
- Angioplasty balloons for concomitant angioplasty and carotid stenting
- Rapid-exchange or monorail systems preferred
# PROCEDURE
- ## Patient Position/Location
- Supine position, biplane angiography suite
- ## Procedure Steps
- **Diagnostic angiogram**
- Sterilely prepare/drape skin of access site
- Transfemoral access site preferred; transbrachial or transcarotid access if needed
- Conscious sedation if necessary
- Obtain femoral arterial access
- Place femoral artery access sheath
- 4-6 Fr (for diagnostic angiogram)
- 8 Fr (for thrombectomy with balloon guide)
- Select desired carotid/vertebral artery with Glidewire/diagnostic catheter
- Use diagnostic catheter to obtain DSA images
- Carotid/vertebral DSA: Evaluates collateral circulation/filling of vessels distal to occlusion
- Include cervical and cranial views
- Obtain magnified images of target vessel(s), document vascular occlusion
- **Thrombectomy with stent retriever device**
- Useful for occlusions out to M3 segment in MCA or P1 segment in posterior cerebral artery
- Advance balloon guide catheter over wire into internal carotid artery (ICA)
- Navigate microwire/microcatheter into occluded segment
- Pass occlusion site with microwire/microcatheter
- Obtain DSA; verify position of microcatheter tip within vessel, distal to thrombus
- Advance stent retriever device and deploy across thrombus
- Wait 5 minutes for device to interact with thrombus
- Inflate balloon at guide catheter tip within ICA for temporary occlusion
- Aspirate lumen of balloon guide catheter
- Check for thrombus within device or aspirate
- Check Touhy valve for thrombus
- Deflate balloon
- Verify backflow of blood out from balloon guide to ensure thrombus not trapped within guide catheter
- Obtain DSA run through guide catheter to evaluate for residual thrombus or distal emboli
- Assess thrombolysis in cerebral ischemia (TICI) score
- If needed, reload stent retriever device for additional passes
- Average 1.6 passes required
- Atherosclerotic stenosis or dissection can be treated with angioplasty/stenting in select cases
- Cervical run of ICA to ensure no spasm or dissection from guide catheter
- Pull guide catheter to iliac artery; pelvic run to ensure proper placement of sheath for hemostatic closure device
- **Thrombectomy with aspiration catheter**
- Most useful for occlusion within large straight segments, such as paraclinoid ICA, M1, or basilar
- Position long 6-Fr (or larger) sheath in carotid or subclavian artery
- Choose reperfusion catheter size based on occluded vessel diameter
- Advance reperfusion catheter into target vessel over microcatheter/microwire
- Confirm catheter position with DSA imaging
- Engage proximal face of thrombus with reperfusion catheter and aspirate by syringe or aspiration pump
- Follow results with DSA angiography
- **Thrombectomy combining stent retriever and local aspiration**
- Useful when balloon guide catheter placement in ICA not possible or contraindicated
- Position long 6-Fr sheath or balloon guide catheter in carotid or subclavian artery
- Choose reperfusion catheter based on occluded artery diameter
- Navigate reperfusion catheter over microcatheter and microwire to target artery
- Pass occlusion with microcatheter and deploy stent retriever device across thrombus
- While reperfusion catheter is being aspirated, withdraw stent retrieval device into catheter
- Search for thrombus ensnared in device or aspirate
- Repeat if necessary
- **Intracranial angioplasty ± stenting** (not FDA approved for acute stroke)
- Use if recanalization attempts unsuccessful due to underlying stenosis
- Angioplasty balloon size based on occluded vessel
- Use balloon slightly smaller than vessel caliber
- Recommend noncompliant angioplasty balloon
- Advance balloon into occluded segment, inflate
- Perform follow-up DSA
- **Associated cervical carotid stenosis/occlusion**
- Acute stenting of high-grade stenosis/occlusion may be required to achieve access for thrombectomy
- Probing stump of occluded ICA often reveals residual lumen in acute stroke
- Advance microcatheter to distal ICA
- Angiogram through microcatheter will demonstrate thrombus burden within ICA
- Place exchange wire in distal ICA to facilitate placement of distal embolic protection filter device, if possible
- Occluded ICA may have to initially be predilated with very small balloon
- Vagus nerve induced bradycardia may be profound
- Premedicate with atropine or glycopyrrolate
- Stent retriever use after stenting
- Requires placement of balloon guide catheter distal to stent or use of reperfusion catheter
- Avoid retracting stent retriever through ICA stent
- In setting of significant ischemic burden, consider ASA monotherapy vs. clopidogrel without load
- **Associated vertebral ostial stenosis with basilar occlusion**
- If possible, perform thrombectomy through contralateral (nondiseased) vertebral artery
- If thrombectomy requires intervention through stenotic/occluded vertebral ostium
- Angioplasty vertebral ostium without distal embolic protection
- Use reperfusion catheter in basilar ± stent retriever
- Stent vertebral ostium after basilar intervention complete
- **Extracranial carotid/vertebral dissection/stroke**
- Similar approach to cervical carotid stenosis/occlusion
- Distal embolic protection often not possible due to dissection extending to skull base
- Cross dissection with microcatheter
- Verify microcatheter placement in true lumen with DSA run
- Over exchange wire, place self-expanding stent(s)
- Stent often traps flap and thrombus, restoring flow
- ## Findings and Reporting
- Location/characteristics of lesion
- Devices/medications used intraprocedurally
- Procedure times
- Door to groin time
- Time of reperfusion
- TICI grade of perfusion after stroke intervention
- Angiographic degree of reperfusion
- 0: No perfusion beyond occlusion
- 1: Penetration past occlusion but no perfusion
- 2a: Partial perfusion; incomplete distal branch filling of < 50% of territory of occluded vessel
- 2b: Partial perfusion; incomplete distal branch filling of ≥ 50% of territory of occluded vessel
- 2c: Near-complete perfusion; no clearly visible thrombus but delayed contrast runoff
- 3: Full perfusion; filling of all distal branches of expected territory in normal fashion
- Complications
- ## Alternative Procedures/Therapies
- ### Radiologic
- Direct carotid access if unable to select common carotid artery/ICA due to tortuosity
- IA tPA
- Once considered primary treatment, now only in rare select cases
- Combined strategies: IV followed by thrombectomy
- ### Surgical
- Hemicraniectomy for large MCA strokes to avoid herniation from edema
# POST PROCEDURE
- ## Things to Do
- Patient management after IA therapy
- Admission to ICU
- Neurologic exam/vital signs q 15 minutes 2 hours, q 30 minutes for 6 hours, q 1 hour for 24 hours
- Maintain SBP of 100-160 mm Hg
- Head CT for any neurologic status changes
- Postprocedure medications (procedure dependent)
- If carotid stent required
- ASA 325 mg, clopidogrel 150- to 300-mg loading dose (if ischemic burden low)
- Maintain on daily clopidogrel 75 mg for 4-6 weeks, daily ASA 325 mg indefinitely
- Atropine or glycopyrrolate for vagus nerve-mediated bradycardia/hypotension; pressors if needed
# OUTCOMES
- ## Complications
- Brain hemorrhage
- May categorize postthrombolysis hemorrhagic transformations (HT) by CT-based classification of European Cooperative Acute Stroke Study (ECASS)
- No HT
- Hemorrhagic infarct type 1 (HI1): Small petechiae
- HI2: Medium petechiae
- Parenchymal hematoma type 1 (PH1): HI large (≤ 30% of infarcted area; mild mass effect)
- PH2: Hematoma (≥ 30% of infarcted area; significant mass effect)
- Mechanical thrombectomy complications
- Device-related complications
- Vascular perforation
- Arterial dissection
- Embolization to previously uninvolved territory
- Worsening brain infarction
- Malignant brain edema of infarcted territory
- Bleeding/hematoma at arterial access site
- Angioplasty/stenting complications
- Similar device-related complications
- Vascular perforation
- Arterial dissection
- Vagus nerve-mediated bradycardia/hypotension
- ## Management of Complications
- Asymptomatic/small hemorrhage (< 30 mL)
- Tight blood pressure control (SBP < 160 mm Hg)
- Frequent neurologic exams
- Reverse anticoagulation
- Consider giving clotting factors/platelets
- Symptomatic, significant hemorrhage (> 30 mL)
- Reverse anticoagulation
- Consider: Ventriculostomy (symptomatic hydrocephalus); craniotomy (clot evacuation)
- ## Expected Outcomes
- Mechanical thrombectomy
- Successful recanalization (72-93%)
- Good clinical outcome; modified Rankin scale ≤ 2 at 90 days (51-60%)
- Slight disability; able to look after own affairs without assistance, but unable to carry out all previous activities
- Significant procedural complications (1-3%)
- Symptomatic intracerebral hemorrhage (3.6%)
- Mortality (10-12%)
- Lower success rate and higher morbidity/mortality with basilar artery occlusions
330162ac-9d2d-4184-8687-392681ef35a5
## References
# Selected References
1. [Roaldsen MB et al: Intravenous thrombolytic treatment and endovascular thrombectomy for ischaemic wake-up stroke. Cochrane Database Syst Rev. 12:CD010995, 2021](http://www.ncbi.nlm.nih.gov/pubmed/?term=34850380%5Bpmid%5D)
1. [Weller JM et al: Endovascular treatment for acute stroke in cerebral amyloid angiopathy. Stroke. 52(10):e581-5, 2021](http://www.ncbi.nlm.nih.gov/pubmed/?term=34412512%5Bpmid%5D)
1. [Campbell BCV et al: Stroke. Lancet. 396(10244):129-42, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=32653056%5Bpmid%5D)
1. [Herpich F et al: Management of acute ischemic stroke. Crit Care Med. 48(11):1654-63, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=32947473%5Bpmid%5D)
1. [Sairanen T et al: Should we thrombolyse prior to endovascular treatment in acute stroke? Clin Neurol Neurosurg. 177:117-22, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30446414%5Bpmid%5D)
1. [Berkhemer OA et al: A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 372(1):11-20, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=25517348%5Bpmid%5D)
1. [Goyal M et al: Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 372(11):1019-30, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=25671798%5Bpmid%5D)
1. [Saver JL et al: Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 372(24):2285-95, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=25882376%5Bpmid%5D)
1. [Sheth SA et al: M2 occlusions as targets for endovascular therapy: comprehensive analysis of diffusion/perfusion MRI, angiography, and clinical outcomes. J Neurointerv Surg. 7(7):478-83, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=24821842%5Bpmid%5D)
1. [Campbell BC et al: A multicenter, randomized, controlled study to investigate EXtending the time for Thrombolysis in Emergency Neurological Deficits with Intra-Arterial therapy (EXTEND-IA). Int J Stroke. 9(1):126-32, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24207098%5Bpmid%5D)
1. [Nguyen TN et al: Balloon guide catheter improves revascularization and clinical outcomes with the Solitaire device: analysis of the North American Solitaire Acute Stroke Registry. Stroke. 45(1):141-5, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24302483%5Bpmid%5D)
1. [Davis MJ et al: Anesthetic management and outcome in patients during endovascular therapy for acute stroke. Anesthesiology. 116(2):396-405, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22222475%5Bpmid%5D)
1. [Saver JL et al: Solitaire flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel-group, non-inferiority trial. Lancet. 380(9849):1241-9, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22932715%5Bpmid%5D)
1. [Konstas AA et al: CT perfusion imaging of acute stroke: the need for arrival time, delay insensitive, and standardized postprocessing algorithms? Radiology. 254(1):22-5, 2010](http://www.ncbi.nlm.nih.gov/pubmed/?term=20032139%5Bpmid%5D)
1. [Konstas AA et al: Theoretic basis and technical implementations of CT perfusion in acute ischemic stroke, part 1: Theoretic basis. AJNR Am J Neuroradiol. 30(4):662-8, 2009](http://www.ncbi.nlm.nih.gov/pubmed/?term=19270105%5Bpmid%5D)
1. [Konstas AA et al: Theoretic basis and technical implementations of CT perfusion in acute ischemic stroke, part 2: technical implementations. AJNR Am J Neuroradiol. 30(5):885-92, 2009](http://www.ncbi.nlm.nih.gov/pubmed/?term=19299489%5Bpmid%5D)
1. Hurst RW et al: Interventional Neuroradiology. New York: Informa Healthcare, 2008
1. [Smith WS et al: Mechanical thrombectomy for acute ischemic stroke: final results of the Multi MERCI trial. Stroke. 39(4):1205-12, 2008](http://www.ncbi.nlm.nih.gov/pubmed/?term=18309168%5Bpmid%5D)
1. Gonzalez RG et al: Acute Ischemic Stroke: Imaging and Intervention. Berlin Heidelberg: Springer-Verlag, 2006
1. [Hacke W et al: Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA. 274(13):1017-25, 1995](http://www.ncbi.nlm.nih.gov/pubmed/?term=7563451%5Bpmid%5D)
1. [Bonita R et al: Recovery of motor function after stroke. Stroke. 19(12):1497-500, 1988](http://www.ncbi.nlm.nih.gov/pubmed/?term=3201508%5Bpmid%5D)
1. [van Swieten JC et al: Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 19(5):604-7, 1988](http://www.ncbi.nlm.nih.gov/pubmed/?term=3363593%5Bpmid%5D)
1. [Mahoney FI et al: Functional evaluation: the Barthel Index. Md State Med J. 14:61-5, 1965](http://www.ncbi.nlm.nih.gov/pubmed/?term=14258950%5Bpmid%5D)
1. [Rankin J: Cerebral vascular accidents in patients over the age of 60. II. Prognosis. Scott Med J. 2(5):200-15, 1957](http://www.ncbi.nlm.nih.gov/pubmed/?term=13432835%5Bpmid%5D)
## Images
### Selected Images
 . The anterior temporal branch of the right MCA remains patent
. The anterior temporal branch of the right MCA remains patent  . The appearance is typical of an embolic occlusion.](images/app.statdx.com_image_thumbnail_77c1e3c7-7635-4c44-930c-be164ebede7c_annotated_true_size_900_quality_90_9dd3d252f7518896dc8cdcffc66749076fe41865.jpg)
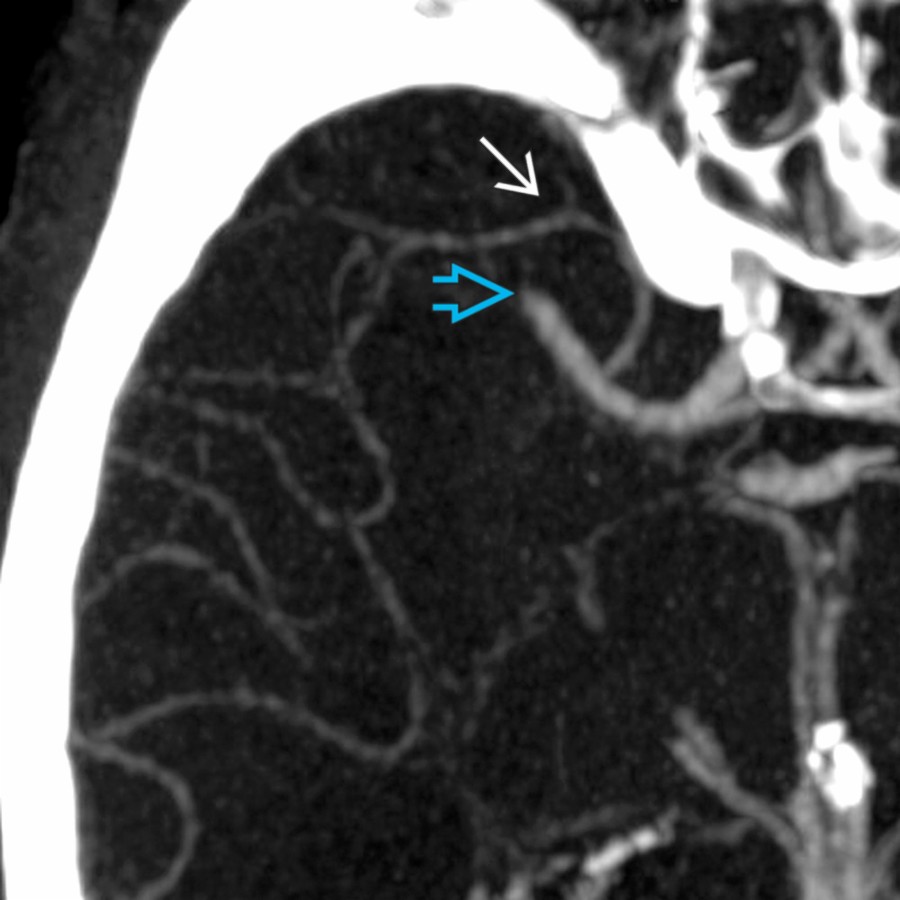
**Preprocedural Planning: Acute Stroke Intervention (Initial CTA)**
*Reformatted CTA shows occlusion of the right middle cerebral artery (MCA), M1 segment . The anterior temporal branch of the right MCA remains patent . The appearance is typical of an embolic occlusion.*
**Preprocedural Planning: Acute Stroke Intervention (Initial CTA)**
*Reformatted CTA shows occlusion of the right middle cerebral artery (MCA), M1 segment . The anterior temporal branch of the right MCA remains patent . The appearance is typical of an embolic occlusion.*
**Preprocedural Planning: Acute Stroke Intervention (Initial CTA)**
*Reformatted CTA shows occlusion of the right middle cerebral artery (MCA), M1 segment . The anterior temporal branch of the right MCA remains patent . The appearance is typical of an embolic occlusion.*

**Preprocedural Planning: Acute Stroke Intervention (Initial CTA)**
*Reformatted CTA shows occlusion of the right middle cerebral artery (MCA), M1 segment . The anterior temporal branch of the right MCA remains patent . The appearance is typical of an embolic occlusion.*
 compared to the left side due to the MCA occlusion. MTT, which measures average blood transit time through a given region of the brain, is a sensitive parameter for restricted perfusion, as seen with embolic occlusion.](images/app.statdx.com_image_thumbnail_d66bd34e-1bf8-4b49-91ed-e3964f321c4e_annotated_true_size_900_quality_90_69b6656b449e0b6cd18757a05d9e6ab73826e1cf.jpg)
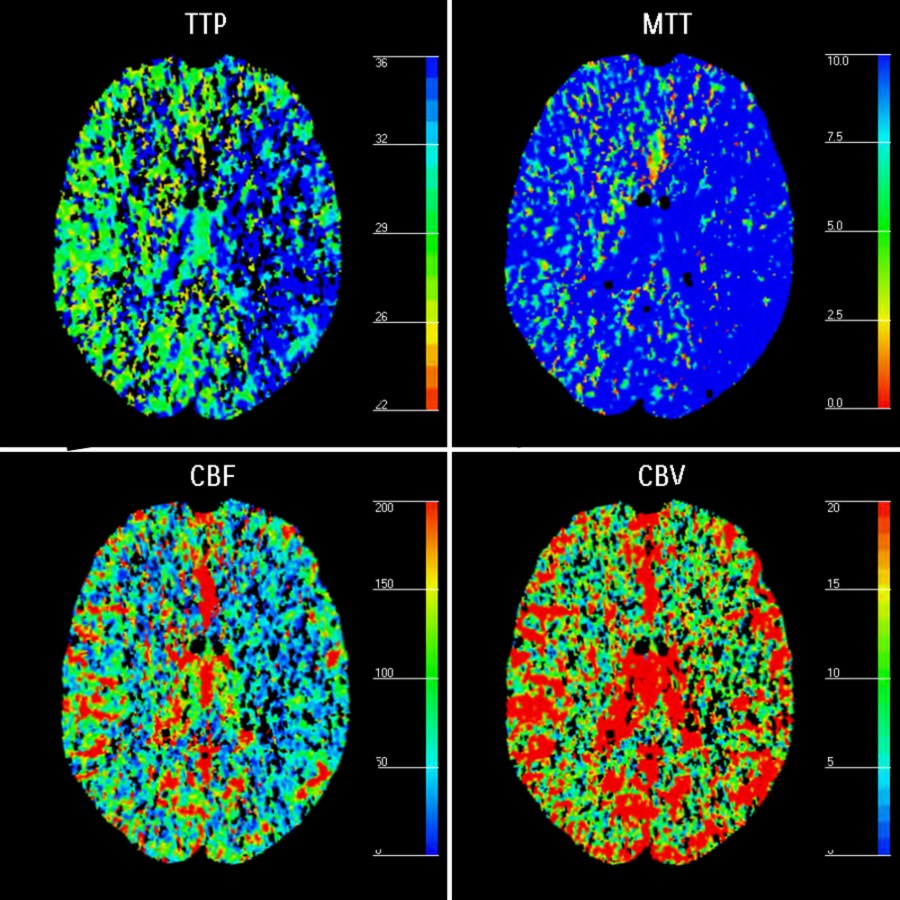
**Preprocedural Planning: Acute Stroke Intervention (CT Perfusion)**
*CT brain perfusion shows a prolonged mean transit time (MTT) in right MCA territory compared to the left side due to the MCA occlusion. MTT, which measures average blood transit time through a given region of the brain, is a sensitive parameter for restricted perfusion, as seen with embolic occlusion.*

**Preprocedural Planning: Acute Stroke Intervention (CT Perfusion)**
*CT brain perfusion shows a prolonged mean transit time (MTT) in right MCA territory compared to the left side due to the MCA occlusion. MTT, which measures average blood transit time through a given region of the brain, is a sensitive parameter for restricted perfusion, as seen with embolic occlusion.*
 , corresponding to the CTA. Acute stroke therapy with mechanical thrombectomy was then performed.](images/app.statdx.com_image_thumbnail_8b759bfe-0bc5-45bd-9ac2-6a7a345e9349_annotated_true_size_900_quality_90_7427aefce266fe14bf4a91eb2689f8e232717a6b.jpg)
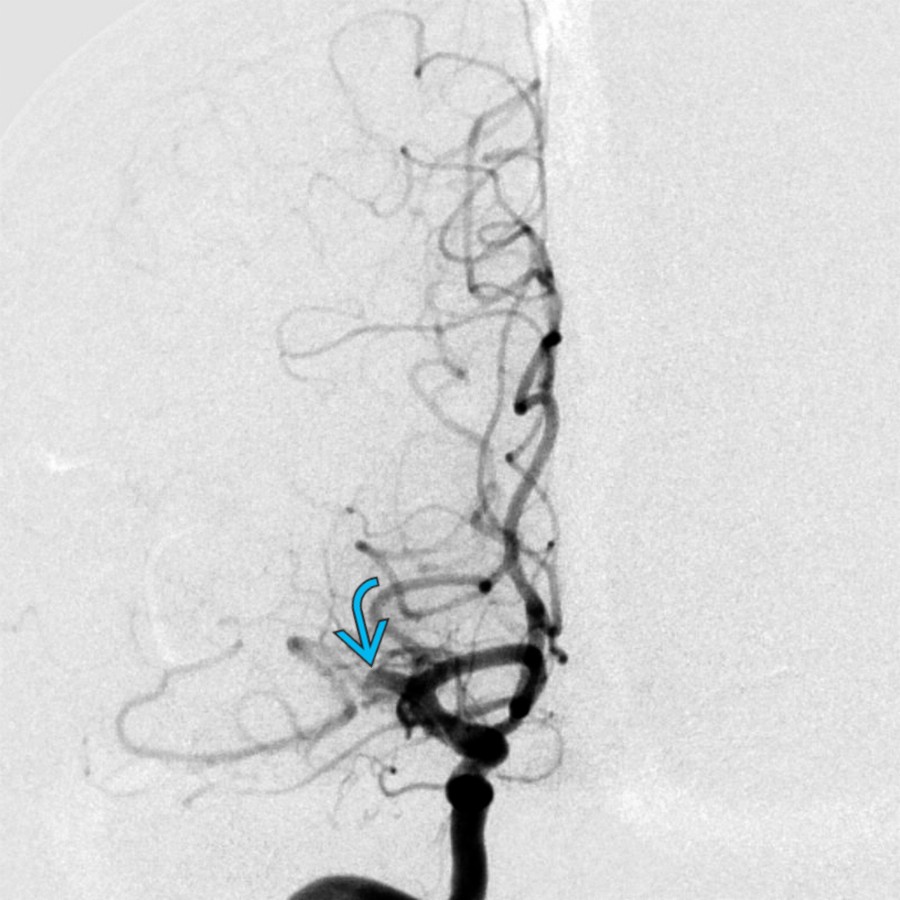
**Intraprocedural: Acute Stroke Intervention (Initial Cerebral Angiography)**
*Right internal carotid DSA shows occlusion of the right MCA, M1 segment , corresponding to the CTA. Acute stroke therapy with mechanical thrombectomy was then performed.*
**Intraprocedural: Acute Stroke Intervention (Initial Cerebral Angiography)**
*Right internal carotid DSA shows occlusion of the right MCA, M1 segment , corresponding to the CTA. Acute stroke therapy with mechanical thrombectomy was then performed.*
 and distal branches
and distal branches  , which were previously nonperfused. The anterior temporal branch
, which were previously nonperfused. The anterior temporal branch  remains patent and is again seen arising from the mid-M1 segment.](images/app.statdx.com_image_thumbnail_578395b5-a256-411d-aea0-e2a1f061e480_annotated_true_size_900_quality_90_01f4ba0f6dccc92ed13115254251c71d94b4ae3e.jpg)
**Intraprocedural: Acute Stroke Intervention (Completion Arteriogram)**
*Right internal carotid DSA following mechanical thrombectomy shows a patent MCA and distal branches , which were previously nonperfused. The anterior temporal branch remains patent and is again seen arising from the mid-M1 segment.*

**Preprocedural Planning: Left ICA Occlusion (Dense ICA Terminus)**
*NECT in a 52-year-old man presenting with acute-onset right hemiplegia, aphasia, and neglect demonstrates dense left internal carotid artery (ICA) terminus .*
**Preprocedural Planning: Left ICA Occlusion (Large Ischemic Penumbra)**
*CT perfusion in the same patient demonstrates a large ischemic penumbra in the left MCA and anterior carotid artery (ACA) territory secondary to the left ICA occlusion.*
**Intraprocedural: Left ICA Occlusion (DSA Confirmation)**
*Lateral DSA demonstrates a filling defect within the distal left ICA , consistent with acute thromboembolus. There is no filling of the left ACA or MCA. The left posterior communicating artery is patent.*
**Intraprocedural: Acute Stroke Intervention (Completion Arteriogram)**
*Right internal carotid DSA following mechanical thrombectomy shows a patent MCA and distal branches , which were previously nonperfused. The anterior temporal branch remains patent and is again seen arising from the mid-M1 segment.*

**Preprocedural Planning: Left ICA Occlusion (Dense ICA Terminus)**
*NECT in a 52-year-old man presenting with acute-onset right hemiplegia, aphasia, and neglect demonstrates dense left internal carotid artery (ICA) terminus .*

**Preprocedural Planning: Left ICA Occlusion (Large Ischemic Penumbra)**
*CT perfusion in the same patient demonstrates a large ischemic penumbra in the left MCA and anterior carotid artery (ACA) territory secondary to the left ICA occlusion.*

**Intraprocedural: Left ICA Occlusion (DSA Confirmation)**
*Lateral DSA demonstrates a filling defect within the distal left ICA , consistent with acute thromboembolus. There is no filling of the left ACA or MCA. The left posterior communicating artery is patent.*
 deployed across the left ICA terminus occlusion.](images/app.statdx.com_image_thumbnail_6fa4758a-8c24-4b8f-9add-fea490ce0d74_annotated_true_size_900_quality_90_7a5658fde2672ffc399aa7ae69264e890c842997.jpg)
**Intraprocedural: Left ICA Occlusion (Solitaire Deployed)**
*Lateral unsubtracted angiogram shows the Solitaire device deployed across the left ICA terminus occlusion.*
![Lateral DSA from the left ICA demonstrates complete restoration of flow to the left ICA territory [thrombolysis in cerebral ischemia (TICI) 3]. This was obtained after 1 pass with the Solitaire 4 x 40-mm device.](images/app.statdx.com_image_thumbnail_3b91212e-959a-490e-98c2-3aa5193b3e5f_annotated_true_size_900_quality_90_8f488f2c63fe93a459f56194614a9081fc7227c0.jpg)
**Intraprocedural: Left ICA Occlusion (Postthrombectomy Angiogram)**
*Lateral DSA from the left ICA demonstrates complete restoration of flow to the left ICA territory [thrombolysis in cerebral ischemia (TICI) 3]. This was obtained after 1 pass with the Solitaire 4 x 40-mm device.*

**Follow-Up: Left ICA Occlusion (Small Ischemic Infarct)**
*Axial DWI MR demonstrates small areas of acute infarction within the left caudate body and left parietal cortex . These are significantly smaller than the ischemic penumbra on CT perfusion. There was no hemorrhage on GRE sequence (not pictured).*

**Preprocedural Planning: Acute Left MCA Stroke (Initial CT)**
*This 65-year-old man presented with acute onset of right hemiplegia, facial droop, aphasia, and neglect 3.5 hours prior to arrival to ED. National Institute of Health Stroke Scale (NIHSS) was 21. NECT demonstrates no acute hemorrhage or gray-white loss. There is chronic small vessel ischemic disease.*

**Preprocedural Planning: Acute Left MCA Stroke (CT Angiogram)**
*However, 3D reformatted image from the same patient's CT angiogram shows occlusion of the proximal left MCA, M1 segment . The left ACA and fetal left posterior cerebral artery (PCA) remain patent.*

**Intraprocedural: Acute Left MCA Stroke (Initial Angiogram)**
*DSA of the left ICA demonstrates abrupt occlusion of the left MCA, M1 segment . The left ACA and fetal left PCA remain patent.*

**Intraprocedural: Acute Left MCA Stroke (Solitaire Device Deployment)**
*Unsubtracted fluoroscopic image (A) and DSA (B) show deployment of the stent retriever device across the left MCA, M1 segment thrombus . Note that only the distal markers of the Solitaire device are radiopaque.*

**Intraprocedural: Acute Left MCA Stroke (Postthrombectomy DSA)**
*DSA following mechanical thrombectomy shows restoration of flow to the left MCA with TICI 3 flow in the distal branches . Two passes with the Solitaire device were required in this patient. The left ACA and fetal left PCA remain patent.*

**Follow-Up: Acute Left MCA Stroke (DWI MR)**
*Axial DWI MR demonstrates only a punctate area of acute infarction in the left MCA territory . There was no hemorrhage on gradient-echo sequence (not pictured).*

**Preprocedural Planning: Basilar Stroke Intervention (Initial NECT)**
*Axial NECT in a patient with an acute stroke shows a hyperdense basilar artery believed to represent intraluminal clot. NECT is initially obtained in acute stroke to exclude intracranial hemorrhage, which is a thrombolysis contraindication.*

**Intraprocedural: Basilar Stroke Intervention (AP Basilar DSA)**
*Selective AP left vertebral DSA obtained in preparation for transcatheter treatment of acute thrombotic occlusion of the basilar artery shows the level of occlusion is just distal to the anterior inferior cerebellar arteries (AICAs) .*

**Intraprocedural: Basilar Stroke Intervention (Lateral Basilar DSA)**
*The basilar artery occlusion is better demonstrated on the lateral DSA arteriogram, with a meniscus seen at the inferior margin of the occluding thrombus in the basilar artery. In addition to the AICAs , the left posterior inferior cerebellar artery (PICA) remains patent.*
**Intraprocedural: Left ICA Occlusion (Solitaire Deployed)**
*Lateral unsubtracted angiogram shows the Solitaire device deployed across the left ICA terminus occlusion.*
![Lateral DSA from the left ICA demonstrates complete restoration of flow to the left ICA territory [thrombolysis in cerebral ischemia (TICI) 3]. This was obtained after 1 pass with the Solitaire 4 x 40-mm device.](images/app.statdx.com_image_thumbnail_3b91212e-959a-490e-98c2-3aa5193b3e5f_annotated_true_size_900_quality_90_8f488f2c63fe93a459f56194614a9081fc7227c0.jpg)
**Intraprocedural: Left ICA Occlusion (Postthrombectomy Angiogram)**
*Lateral DSA from the left ICA demonstrates complete restoration of flow to the left ICA territory [thrombolysis in cerebral ischemia (TICI) 3]. This was obtained after 1 pass with the Solitaire 4 x 40-mm device.*

**Follow-Up: Left ICA Occlusion (Small Ischemic Infarct)**
*Axial DWI MR demonstrates small areas of acute infarction within the left caudate body and left parietal cortex . These are significantly smaller than the ischemic penumbra on CT perfusion. There was no hemorrhage on GRE sequence (not pictured).*

**Preprocedural Planning: Acute Left MCA Stroke (Initial CT)**
*This 65-year-old man presented with acute onset of right hemiplegia, facial droop, aphasia, and neglect 3.5 hours prior to arrival to ED. National Institute of Health Stroke Scale (NIHSS) was 21. NECT demonstrates no acute hemorrhage or gray-white loss. There is chronic small vessel ischemic disease.*

**Preprocedural Planning: Acute Left MCA Stroke (CT Angiogram)**
*However, 3D reformatted image from the same patient's CT angiogram shows occlusion of the proximal left MCA, M1 segment . The left ACA and fetal left posterior cerebral artery (PCA) remain patent.*

**Intraprocedural: Acute Left MCA Stroke (Initial Angiogram)**
*DSA of the left ICA demonstrates abrupt occlusion of the left MCA, M1 segment . The left ACA and fetal left PCA remain patent.*

**Intraprocedural: Acute Left MCA Stroke (Solitaire Device Deployment)**
*Unsubtracted fluoroscopic image (A) and DSA (B) show deployment of the stent retriever device across the left MCA, M1 segment thrombus . Note that only the distal markers of the Solitaire device are radiopaque.*

**Intraprocedural: Acute Left MCA Stroke (Postthrombectomy DSA)**
*DSA following mechanical thrombectomy shows restoration of flow to the left MCA with TICI 3 flow in the distal branches . Two passes with the Solitaire device were required in this patient. The left ACA and fetal left PCA remain patent.*

**Follow-Up: Acute Left MCA Stroke (DWI MR)**
*Axial DWI MR demonstrates only a punctate area of acute infarction in the left MCA territory . There was no hemorrhage on gradient-echo sequence (not pictured).*

**Preprocedural Planning: Basilar Stroke Intervention (Initial NECT)**
*Axial NECT in a patient with an acute stroke shows a hyperdense basilar artery believed to represent intraluminal clot. NECT is initially obtained in acute stroke to exclude intracranial hemorrhage, which is a thrombolysis contraindication.*

**Intraprocedural: Basilar Stroke Intervention (AP Basilar DSA)**
*Selective AP left vertebral DSA obtained in preparation for transcatheter treatment of acute thrombotic occlusion of the basilar artery shows the level of occlusion is just distal to the anterior inferior cerebellar arteries (AICAs) .*

**Intraprocedural: Basilar Stroke Intervention (Lateral Basilar DSA)**
*The basilar artery occlusion is better demonstrated on the lateral DSA arteriogram, with a meniscus seen at the inferior margin of the occluding thrombus in the basilar artery. In addition to the AICAs , the left posterior inferior cerebellar artery (PICA) remains patent.*
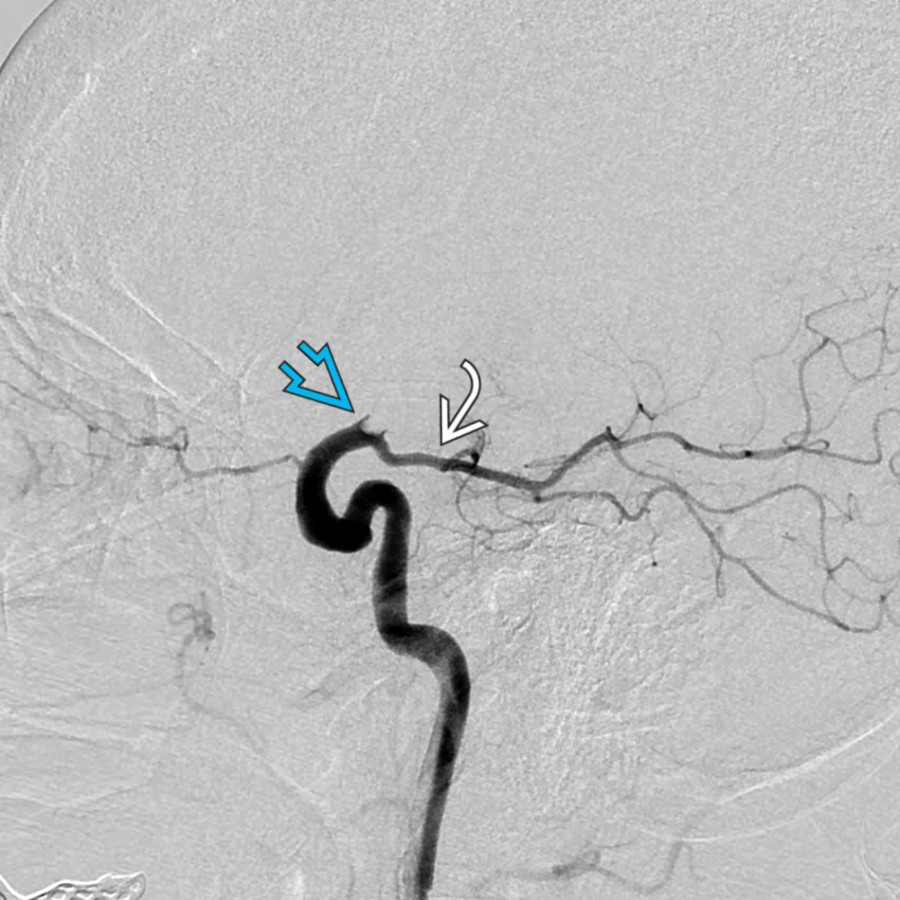
 , which terminates abruptly .](ff9e749a-3276-4a73-9d0c-17c0f90dd72a)
**Intraprocedural: Basilar Stroke Intervention (Postthrombectomy DSA)**
*DSA following thrombectomy shows improved basilar artery patency and flow in the left PCA . There is perfusion of the proximal right PCA , which terminates abruptly .*

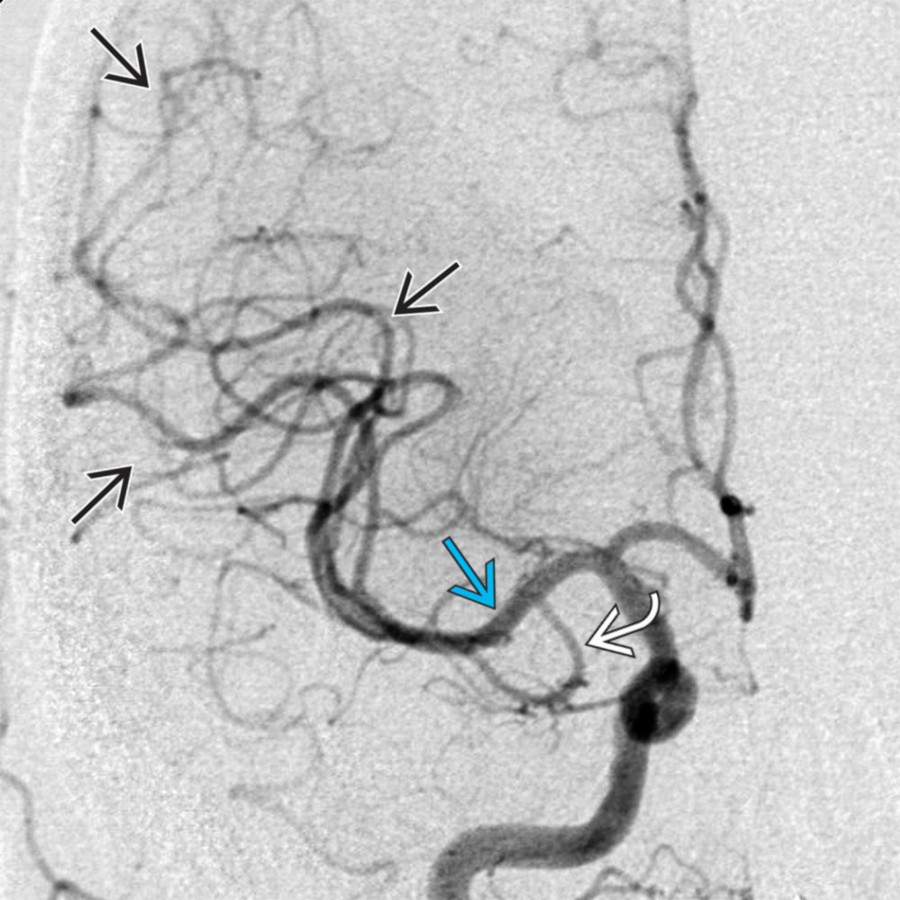
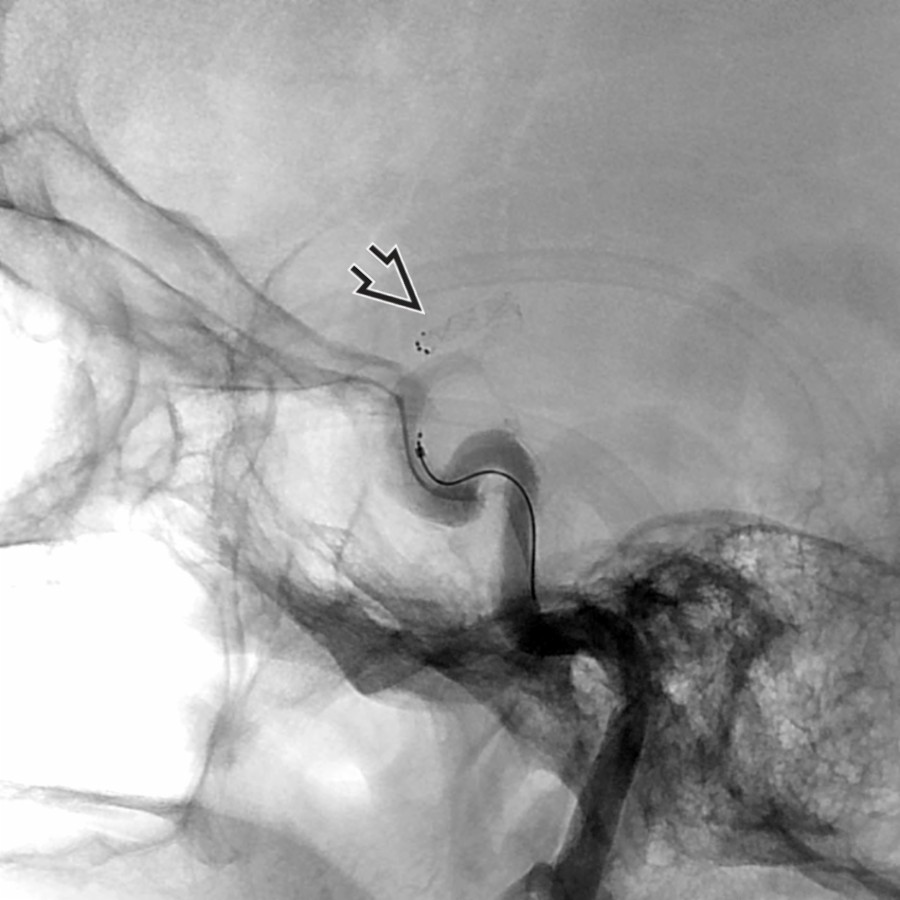
**Intraprocedural: Basilar Stroke Intervention (Advancement of Penumbra)**
*Lateral roadmap fluoroscopy shows that a reperfusion catheter has been advanced distally in the right PCA in an attempt to restore perfusion using thromboaspiration. The patent contralateral left PCA can be seen for comparison.*

**Intraprocedural: Basilar Stroke Intervention (Completion Basilar DSA)**
*Final DSA after aspiration use shows that the right PCA is perfused throughout the entire length. The basilar artery has a normal appearance, as do all branch vessels. This is an example of TICI grade 3 reperfusion.*
### Additional Images

**Acute Left MCA Stroke**
*Axial 3D CTA reformation in a patient who presented within 3 hours of onset of right-sided weakness and right facial droop shows abrupt termination of the left MCA , consistent with occlusion.*

**Acute Left MCA Stroke**
*Axial DWI MR in a patient who presented within 3 hours of onset of right-sided weakness and right facial droop shows an area of restricted diffusion in the left corona radiata , reflecting the ischemic core zone.*

**Acute Left MCA Stroke**
*Axial PWI MR at the same anatomic level in the same patient shows a much more extensive area of decreased perfusion in the left cerebral hemisphere, reflecting ischemic tissue at risk of infarction (penumbra).*

**Acute Left MCA Stroke**
*(A) DWI MR shows restricted diffusion in the left corona radiata , while the corresponding (B) PWI MR shows a more extensive area of decreased perfusion , reflecting cerebral tissue at risk for infarction (penumbra).*

**Basilar Artery Recanalization**
*CT evaluation for stroke shows a hyperdense basilar artery due to a clot.*

**Basilar Artery Recanalization**
*Basilar artery clot/occlusion extending into the left PCA is shown. Note contrast opacification of the right PCA through the posterior communicating artery . There is also some flow in the left PCA through the collateral circulation.*

**Basilar Artery Recanalization**
*Axial CT perfusion shows prolongation of the MTT in the left cerebellar hemisphere in comparison to the contralateral side . Note that there is also MTT prolongation in the left aspect of the pons .*

**Unsuccessful Stroke Intervention: Right Vertebral DSA**
*Selective (A) anteroposterior and (B) lateral right vertebral DSA shows extensive thrombus filling the basilar artery. There are high-grade stenoses of the distal right vertebral artery felt to be the etiology for the acute basilar artery thrombosis. Thrombus also extends into the distal left vertebral artery.*

**Unsuccessful Stroke Intervention: Merci Clot Retrieval**
*Lateral fluoroscopic roadmap image shows (A) that a Merci retrieval device has been advanced into the basilar thrombus for attempted thrombectomy. (B) Subsequently, microwire clot maceration was performed through a microcatheter .*

**Unsuccessful Stroke Intervention: Merci Clot Retrieval**
*Lateral fluoroscopic roadmap image shows a Merci retrieval device has been advanced into the basilar thrombus.*

**Unsuccessful Stroke Intervention: Completion Arteriogram**
*Lateral DSA shows persistent occlusive thrombus in the distal basilar artery and a dissection at the base of the artery. The intervention was unsuccessful despite using multiple techniques for reestablishing perfusion. This represents TICI grade 0 perfusion after stroke intervention.*

**Acute Stroke Intervention: Merci Retrieval System**
*Graphic of Merci device thrombectomy is shown. (A) The device is advanced via a guide catheter across the clot where (B) it is rotated counterclockwise, engaging the clot. (C) The microcatheter, retriever, and clot are withdrawn into the guide catheter while aspirating the clot.*

**Unsuccessful Stroke Intervention: Balloon Angioplasty**
*Lateral fluoroscopic spot radiograph shows that an angioplasty balloon has been inflated in the basilar artery in an attempt to further fragment and macerate the clot. Angioplasty of the vertebrobasilar stenosis was also performed in an attempt to improve arterial inflow.*

**Unsuccessful Stroke Intervention: Initial DWI MR**
*Coronal DWI MR shows increased central and paracentral signal in the pons due to restricted diffusion. This represents the ischemic core and correlates with irreversible injury, which will not respond to reperfusion. PWI evaluates for the presence of penumbra, while DWI/PWI mismatch defines its extent.*
, which terminates abruptly .](ff9e749a-3276-4a73-9d0c-17c0f90dd72a)
**Intraprocedural: Basilar Stroke Intervention (Postthrombectomy DSA)**
*DSA following thrombectomy shows improved basilar artery patency and flow in the left PCA . There is perfusion of the proximal right PCA , which terminates abruptly .*

**Intraprocedural: Basilar Stroke Intervention (Advancement of Penumbra)**
*Lateral roadmap fluoroscopy shows that a reperfusion catheter has been advanced distally in the right PCA in an attempt to restore perfusion using thromboaspiration. The patent contralateral left PCA can be seen for comparison.*

**Intraprocedural: Basilar Stroke Intervention (Completion Basilar DSA)**
*Final DSA after aspiration use shows that the right PCA is perfused throughout the entire length. The basilar artery has a normal appearance, as do all branch vessels. This is an example of TICI grade 3 reperfusion.*
### Additional Images

**Acute Left MCA Stroke**
*Axial 3D CTA reformation in a patient who presented within 3 hours of onset of right-sided weakness and right facial droop shows abrupt termination of the left MCA , consistent with occlusion.*

**Acute Left MCA Stroke**
*Axial DWI MR in a patient who presented within 3 hours of onset of right-sided weakness and right facial droop shows an area of restricted diffusion in the left corona radiata , reflecting the ischemic core zone.*

**Acute Left MCA Stroke**
*Axial PWI MR at the same anatomic level in the same patient shows a much more extensive area of decreased perfusion in the left cerebral hemisphere, reflecting ischemic tissue at risk of infarction (penumbra).*

**Acute Left MCA Stroke**
*(A) DWI MR shows restricted diffusion in the left corona radiata , while the corresponding (B) PWI MR shows a more extensive area of decreased perfusion , reflecting cerebral tissue at risk for infarction (penumbra).*

**Basilar Artery Recanalization**
*CT evaluation for stroke shows a hyperdense basilar artery due to a clot.*

**Basilar Artery Recanalization**
*Basilar artery clot/occlusion extending into the left PCA is shown. Note contrast opacification of the right PCA through the posterior communicating artery . There is also some flow in the left PCA through the collateral circulation.*

**Basilar Artery Recanalization**
*Axial CT perfusion shows prolongation of the MTT in the left cerebellar hemisphere in comparison to the contralateral side . Note that there is also MTT prolongation in the left aspect of the pons .*

**Unsuccessful Stroke Intervention: Right Vertebral DSA**
*Selective (A) anteroposterior and (B) lateral right vertebral DSA shows extensive thrombus filling the basilar artery. There are high-grade stenoses of the distal right vertebral artery felt to be the etiology for the acute basilar artery thrombosis. Thrombus also extends into the distal left vertebral artery.*

**Unsuccessful Stroke Intervention: Merci Clot Retrieval**
*Lateral fluoroscopic roadmap image shows (A) that a Merci retrieval device has been advanced into the basilar thrombus for attempted thrombectomy. (B) Subsequently, microwire clot maceration was performed through a microcatheter .*

**Unsuccessful Stroke Intervention: Merci Clot Retrieval**
*Lateral fluoroscopic roadmap image shows a Merci retrieval device has been advanced into the basilar thrombus.*

**Unsuccessful Stroke Intervention: Completion Arteriogram**
*Lateral DSA shows persistent occlusive thrombus in the distal basilar artery and a dissection at the base of the artery. The intervention was unsuccessful despite using multiple techniques for reestablishing perfusion. This represents TICI grade 0 perfusion after stroke intervention.*

**Acute Stroke Intervention: Merci Retrieval System**
*Graphic of Merci device thrombectomy is shown. (A) The device is advanced via a guide catheter across the clot where (B) it is rotated counterclockwise, engaging the clot. (C) The microcatheter, retriever, and clot are withdrawn into the guide catheter while aspirating the clot.*

**Unsuccessful Stroke Intervention: Balloon Angioplasty**
*Lateral fluoroscopic spot radiograph shows that an angioplasty balloon has been inflated in the basilar artery in an attempt to further fragment and macerate the clot. Angioplasty of the vertebrobasilar stenosis was also performed in an attempt to improve arterial inflow.*

**Unsuccessful Stroke Intervention: Initial DWI MR**
*Coronal DWI MR shows increased central and paracentral signal in the pons due to restricted diffusion. This represents the ischemic core and correlates with irreversible injury, which will not respond to reperfusion. PWI evaluates for the presence of penumbra, while DWI/PWI mismatch defines its extent.*