---
title: "Temporal Bone Facial Nerve Venous Malformation (Hemangioma)"
docid: "dcd6a44e-cbe6-457c-9b03-598a2b874ece"
authors:
- key: "07a2c087-6202-49e7-870b-7aa162d18f06"
value: "Bronwyn E. Hamilton, MD"
- key: "33151213-01b2-4542-9105-342e006b3915"
value: "H. Ric Harnsberger, MD"
breadcrumbs:
-
name: "Head and Neck"
slug: "head-and-neck"
treeNodeId: "ed24ed8c-5d57-4629-879b-447b82d2973d"
-
name: "Diagnosis"
slug: "diagnosis"
treeNodeId: "19b6b986-97d0-40e7-b317-00f0c5cd8fa2"
-
name: "Temporal Bone"
slug: "temporal-bone"
treeNodeId: "9ad7d7b2-b2e4-4de2-be04-55ce607560c9"
-
name: "Intratemporal Facial Nerve"
slug: "intratemporal-facial-nerve"
treeNodeId: "35b77f60-796d-460f-8bac-4a187a150171"
-
name: "Benign and Malignant Tumors"
slug: "benign-and-malignant-tumors"
treeNodeId: "353e7622-0bb3-4dce-96d6-f5f889dad7cb"
-
name: "Temporal Bone Facial Nerve Venous Malformation (Hemangioma)"
slug: "temporal-bone-facial-nerve-venous--"
treeNodeId: null
category: "Head and Neck"
cmeTopicId: "dd372219-4d64-42de-bbf4-f52c566360c5"
documentVersionId: "fc953809-a667-41c7-92f6-3eec505b0896"
imageCount: 14
lastUpdated: "07/30/21"
pageDescription: "Temporal Bone Facial Nerve Venous Malformation (Hemangioma)"
pageKeywords: "Head and Neck, Diagnosis, Temporal Bone, Intratemporal Facial Nerve, Benign and Malignant Tumors, Temporal Bone Facial Nerve Venous Malformation (Hemangioma)"
pageTitle: "Temporal Bone Facial Nerve Venous Malformation (Hemangioma) | STATdx"
enhancedTitle: "Temporal Bone Facial Nerve Venous Malformation (Hemangioma)"
type: "DX"
references: true
ddx: true
anatomy:
- "{'authors': 'Philip R. Chapman, MD; Ryan P. Cabeen, PhD', 'bookmarked': False, 'bookmarkUrl': '/document/bookmark/2f4818dd-6438-405b-8561-5cbbb9c91562', 'category': 'Brain', 'compareUrl': '/compare/document/2f4818dd-6438-405b-8561-5cbbb9c91562/related-anatomy/treeNode?subContext=Facial Nerve (CNVII)', 'documentId': '2f4818dd-6438-405b-8561-5cbbb9c91562', 'documentType': 'ANATOMY', 'documentUrl': '/document/facial-nerve-cnvii/2f4818dd-6438-405b-8561-5cbbb9c91562', 'enhancedTitle': 'Facial Nerve (CNVII)', 'entryDate': '10/20/20', 'imageCount': 27, 'imageUrl': '/image/thumbnail/22d61165-f6cb-4f78-83a6-c5b5d308b29f?size=174&quality=85', 'inCompareCart': False, 'rank': 1, 'referenceCount': 0, 'showCompareButton': False, 'title': 'Facial Nerve (CNVII)'}"
- "{'authors': 'Philip R. Chapman, MD; Ryan P. Cabeen, PhD', 'bookmarked': False, 'bookmarkUrl': '/document/bookmark/498e844d-faca-4c6a-bff1-9c6ad4993e62', 'category': 'Brain', 'compareUrl': '/compare/document/498e844d-faca-4c6a-bff1-9c6ad4993e62/related-anatomy/treeNode?subContext=Vestibulocochlear Nerve (CNVIII)', 'documentId': '498e844d-faca-4c6a-bff1-9c6ad4993e62', 'documentType': 'ANATOMY', 'documentUrl': '/document/vestibulocochlear-nerve-cnviii/498e844d-faca-4c6a-bff1-9c6ad4993e62', 'enhancedTitle': 'Vestibulocochlear Nerve (CNVIII)', 'entryDate': '10/20/20', 'imageCount': 21, 'imageUrl': '/image/thumbnail/8412acd1-87f7-4c42-94a2-55d9e0e4c2b6?size=174&quality=85', 'inCompareCart': False, 'rank': 2, 'referenceCount': 0, 'showCompareButton': False, 'title': 'Vestibulocochlear Nerve (CNVIII)'}"
- "{'authors': 'Surjith Vattoth, MD, FRCR', 'bookmarked': False, 'bookmarkUrl': '/document/bookmark/99aff289-b689-4693-9b41-2adbbda59179', 'category': 'Head and Neck', 'compareUrl': '/compare/document/99aff289-b689-4693-9b41-2adbbda59179/related-anatomy/treeNode?subContext=Middle Ear-Mastoid Anatomy', 'documentId': '99aff289-b689-4693-9b41-2adbbda59179', 'documentType': 'ANATOMY', 'documentUrl': '/document/middle-ear-mastoid-anatomy/99aff289-b689-4693-9b41-2adbbda59179', 'enhancedTitle': 'Middle Ear-Mastoid Anatomy', 'entryDate': '01/12/24', 'imageCount': 33, 'imageUrl': '/image/thumbnail/ed90d25c-345d-44b8-96b9-eb6cae913077?size=174&quality=85', 'inCompareCart': False, 'rank': 3, 'referenceCount': 0, 'showCompareButton': False, 'title': 'Middle Ear-Mastoid Anatomy'}"
- "{'authors': 'Surjith Vattoth, MD, FRCR; Philip R. Chapman, MD; H. Ric Harnsberger, MD', 'bookmarked': False, 'bookmarkUrl': '/document/bookmark/48ee77aa-d460-43f3-a3e2-9fd61632ca4a', 'category': 'Head and Neck', 'compareUrl': '/compare/document/48ee77aa-d460-43f3-a3e2-9fd61632ca4a/related-anatomy/treeNode?subContext=Inner Ear Anatomy', 'documentId': '48ee77aa-d460-43f3-a3e2-9fd61632ca4a', 'documentType': 'ANATOMY', 'documentUrl': '/document/inner-ear-anatomy/48ee77aa-d460-43f3-a3e2-9fd61632ca4a', 'enhancedTitle': 'Inner Ear Anatomy', 'entryDate': '12/18/23', 'imageCount': 20, 'imageUrl': '/image/thumbnail/c7ee4c7e-169b-4857-a76a-de0f0c7d49b7?size=174&quality=85', 'inCompareCart': False, 'rank': 4, 'referenceCount': 0, 'showCompareButton': False, 'title': 'Inner Ear Anatomy'}"
- "{'authors': 'Santhosh Gaddikeri, MD; Philip R. Chapman, MD', 'bookmarked': False, 'bookmarkUrl': '/document/bookmark/98cb2d45-e64c-4295-9662-3470cd46513a', 'category': 'Head and Neck', 'compareUrl': '/compare/document/98cb2d45-e64c-4295-9662-3470cd46513a/related-anatomy/treeNode?subContext=CNVII (Facial Nerve)', 'documentId': '98cb2d45-e64c-4295-9662-3470cd46513a', 'documentType': 'ANATOMY', 'documentUrl': '/document/cnvii-facial-nerve/98cb2d45-e64c-4295-9662-3470cd46513a', 'enhancedTitle': 'CNVII (Facial Nerve)', 'entryDate': '12/06/23', 'imageCount': 39, 'imageUrl': '/image/thumbnail/1f7e56c2-da7a-4445-ac01-44eee0776f17?size=174&quality=85', 'inCompareCart': False, 'rank': 5, 'referenceCount': 0, 'showCompareButton': False, 'title': 'CNVII (Facial Nerve)'}"
- "{'authors': 'Santhosh Gaddikeri, MD; Philip R. Chapman, MD', 'bookmarked': False, 'bookmarkUrl': '/document/bookmark/e9917c41-94c9-46aa-b9d8-b196c375d35b', 'category': 'Head and Neck', 'compareUrl': '/compare/document/e9917c41-94c9-46aa-b9d8-b196c375d35b/related-anatomy/treeNode?subContext=CNVIII (Vestibulocochlear Nerve)', 'documentId': 'e9917c41-94c9-46aa-b9d8-b196c375d35b', 'documentType': 'ANATOMY', 'documentUrl': '/document/cnviii-vestibulocochlear-nerve/e9917c41-94c9-46aa-b9d8-b196c375d35b', 'enhancedTitle': 'CNVIII (Vestibulocochlear Nerve)', 'entryDate': '12/20/23', 'imageCount': 27, 'imageUrl': '/image/thumbnail/dd6d38e6-2cf7-4a62-a73c-26dd75ccdd2b?size=174&quality=85', 'inCompareCart': False, 'rank': 6, 'referenceCount': 0, 'showCompareButton': False, 'title': 'CNVIII (Vestibulocochlear Nerve)'}"
cases: 2
breadcrumbs:
- "Head and Neck"
- "Diagnosis"
- "Temporal Bone"
- "Intratemporal Facial Nerve"
- "Benign and Malignant Tumors"
- "Temporal Bone Facial Nerve Venous Malformation (Hemangioma)"
---
# KEY FACTS
- ## Terminology
- Facial nerve venous malformation (FNVM)
- Older terms: Facial nerve hemangioma/ossifying hemangioma
- Definition: Benign developmental lesion near intratemporal CNVII in geniculate fossa area
- ## Imaging
- Bone CT
- **Honeycomb high-density matrix** lesion (50%)
- Most commonly located in geniculate fossa
- T1 C+ FS MR
- Enhancing geniculate ganglion area lesion
- Usually with irregular margins
- ## Top Differential Diagnoses
- Normal intratemporal facial nerve enhancement
- Intratemporal facial nerve schwannoma
- Bell palsy
- Perineural parotid malignancy on intratemporal CNVII
- Congenital cholesteatoma within intratemporal CNVII canal
- ## Pathology
- **Immunohistochemical markers** critical to correct venous malformation (hemangioma) diagnosis
- Endothelial lining of vascular channels stain negatively for hemangioma-associated markers (**GLUT1 & LeY**)
- **Podoplanin** staining utilizing D2-40 antibody **negativity** excludes lymphatic malformation
- ## Clinical Issues
- Intratemporal FNVM produces **peripheral CNVII paralysis** early in its natural history
- Caveat: May be described as "**atypical Bell palsy**"
- Treatment: Perform surgery as soon as possible
- Final CNVII function depends on duration of preoperative CNVII deficit
- Smaller lesion are extraneural, larger lesion invade CNVII
# TERMINOLOGY
- ## Abbreviations
- Facial nerve venous malformation (FNVM)
- ## Synonyms
- Facial nerve hemangioma/ossifying hemangioma
- Historic terms for FNVM
- ## Definitions
- FNVM: Benign developmental lesion near intratemporal facial nerve in geniculate fossa area
# IMAGING
- ## General Features
- ### Best diagnostic clue
- **Honeycomb high-density matrix** lesion in geniculate fossa area (bone CT)
- Enhancing geniculate ganglion area lesion with irregular margins on T1 C+ MR
- ### Location
- **Geniculate fossa area** > > internal auditory canal (IAC)
- ### Size
- Range: 2 mm to 2 cm
- Small at presentation, **often < 1 cm**
- ### Morphology
- Irregular, invasive-appearing margins typical
- ## CT Findings
- ### Bone CT
- Poorly marginated lesion of geniculate fossa
- Larger lesions affect adjacent temporal bone
- Anteromedial to geniculate fossa
- Labyrinthine segment CNVII → IAC
- Dumbbell lesion appearance
- Amorphous**honeycomb bone changes** are distinctive
- Present in 50% of all lesions
- Seen in 100% of larger lesions
- Punctate high-density foci also possible
- ## MR Findings
- ### T1WI
- Mixed signal lesion with foci of low signal within lesion matrix (ossific matrix)
- ### T2WI
- High-signal lesion with foci of low signal within lesion matrix
- ### FLAIR
- Mixed intermediate- & high-signal lesion
- ### T1WI C+
- **Avid lesion enhancement** is rule
- Perineural spread from geniculate ganglion
- Posterolateral along tympanic segment CNVII
- Posteromedial along labyrinthine segment CNVII → IAC
- **Dumbbell** appearance possible
- Fundal IAC FNVM, exactly mimics vestibular schwannoma
- Ovoid, well-demarcated, enhancing IAC mass
- Low-signal foci may distinguish FNVM from vestibular schwannoma
- ## Imaging Recommendations
- ### Best imaging tool
- Imaging indicates CNVII (**facial nerve paresis**) or CNVIII (hearing loss) dysfunction
- 1st exam: Thin-section **T1 C+ MR** focused to cerebellopontine angle (CPA)-IAC-inner ear
- If MR negative or shows equivocal small area of enhancement along intratemporal CNVII, recommend **temporal** **bone CT**
- Bone CT may show small FNVM in geniculate fossa
- Inspect intratemporal CNVII canal carefully for 1- to 2-mm FNVM
# DIFFERENTIAL DIAGNOSIS
- [Normal Intratemporal Facial Nerve Enhancement](/document/intratemporal-facial-nerve-enhance-/a3569ec5-a566-411d-877f-41ad832e3fd2)
- Clinical: Asymptomatic
- Imaging: T1 C+ MR shows normal enhancement of geniculate ganglion, anterior tympanic CNVII, &/or mastoid segment CNVII
- Comment: Sometimes mistaken for facial nerve pathology
- [Intratemporal Facial Nerve Schwannoma](/document/temporal-bone-facial-nerve-schwann-/cf2bcc82-4a1b-4989-adeb-f4e82116111b)
- Clinical: Hearing loss ± gradual onset of CNVII paralysis
- Imaging: T1 C+ MR reveals tubular enhancing mass, smoothly enlarging CNVII canal (bone CT)
- Comment: Most commonly centered in geniculate ganglion similar to FNVM
- [Bell Palsy](/document/bell-palsy/0958e575-8f76-4d70-b806-0dbed9c62a67)
- Clinical: Acute onset of peripheral CNVII paralysis
- Imaging: T1 C+ MR shows prominent enhancement of all or most of intratemporal CNVII
- IAC enhancing tuft often present
- Comment: No focal mass; bone CT normal
- ## Perineural Parotid Malignancy on Intratemporal CNVII
- Clinical: Parotid malignancy in history, palpable or subclinical
- Imaging: T1 C+ MR shows invasive parotid mass
- Stylomastoid foramen is tissue filled
- CNVII enlarged & enhancing from distal to proximal
- CNVII may be involved to CPA-IAC
- Mastoid air cell invasion also possible
- Comment: Continuous linear nature different from focal FNVM
- ## Congenital Cholesteatoma Within Intratemporal CNVII Canal
- Clinical: Avascular mass behind intact tympanic membrane
- Imaging: T1 C+ MR shows nonenhancing middle ear mass tracking along CNVII canal
- Comment: Involvement of facial nerve canal rare with this lesion
# PATHOLOGY
- ## General Features
- ### Etiology
- Benign congenital venous malformation arising out of sites of anastomoses between feeding arteries in temporal bone
- ## Staging, Grading, & Classification
- Classification for vascular lesions based on clinical, histopathologic, & cytologic features was introduced by Mulliken & Glowacki in 1982
- **Malformation** term used for errors of vascular morphogenesis that develop in utero & persist postnatally
- **Hemangioma** term reserved for benign vascular tumors that arise by cellular hyperplasia
- ## Gross Pathologic & Surgical Features
- Richly vascular lesion without large feeding vessels
- ## Microscopic Features
- H&E: Nonencapsulated venous malformation composed of dilated vascular channels of varying sizes
- Widely ectatic vascular channels rimmed by thin smooth muscle coats without evident elastic laminae
- Flattened & mitotically quiescent endothelial cells
- Venous malformations = low-flow lesions
- Ossifying type: Lesion has spicules of lamellar bone
- When seen, called **ossifying venous malformation**
- **Immunohistochemical markers** critical to correct venous malformation diagnosis
- Endothelial lining of vascular channels stain negatively for hemangioma-associated markers (**GLUT1 & LeY antigen**)
- CD31-positive endothelial lining & smooth muscle component, consistent with venous malformation
- Venous vs. lymphatic malformation endothelial differentiation
- **Podoplanin** staining utilizing D2-40 antibody **negative** for endothelial cells confirms lack of lymphatic differentiation
# CLINICAL ISSUES
- ## Presentation
- ### Most common signs/symptoms
- Intratemporal FNVM produces **peripheral CNVII paralysis** early in its natural history
- Occurs early because of intimate relationship between CNVII & FNVM
- Onset of CNVII paralysis usually acute: May be slowly progressive or intermittent
- Caveat: May be described as "**atypical Bell palsy**"
- IAC FNVM
- Sensorineural hearing loss may be more prominent symptom
- IAC lesion with CNVII symptoms, consider FNVM
- ### Other signs/symptoms
- Hemifacial spasm may progress to CNVII paralysis
- ### Clinical profile
- Intratemporal FNVM: Adult with relatively rapid onset of peripheral CNVII paralysis (over weeks)
- IAC FNVM: Adult with relatively rapid onset of CNVII paralysis with concomitant Sensorineural hearing loss (SNHL) (over weeks)
- ## Demographics
- ### Age
- Wide range but usually adults
- ### Epidemiology
- Rare lesion
- 0.7% of all temporal bone lesions
- Slightly less common than CNVII schwannoma
- ## Natural History & Prognosis
- FNVM = slowly growing lesion
- Proportional growth is norm
- Disproportionate growth can occur secondary to infection, trauma, hormonal influences, or progressive hemodynamic forces
- Prognosis related to size at diagnosis, severity & duration of preoperative CNVII paralysis
- After surgery, full CNVII function rarely regained
- ## Treatment
- Surgery done as soon as possible
- Final facial nerve function depends on duration of preoperative CNVII deficit
- Surgical alternatives
- Middle cranial fossa (MCF) approach for lesions confined to geniculate fossa
- MCF-transmastoid approach for lesion of geniculate fossa & tympanic segment CNVII
- Small FNVM are extraneural
- Resection with preservation of CNVII function = goal
- Even with small lesions, rarely achieved
- Larger FNVM invades facial nerve
- Segmental facial nerve resection completed
- Followed by primary or cable graft repair of CNVII
- When necessary, yields poorer outcome
# DIAGNOSTIC CHECKLIST
- ## Consider
- FNVM presents with CNVII dysfunction when small
- Since early removal is best chance at CNVII preservation, radiologist must make diagnosis of subtle lesions
- Caveat: **Small FNVM** may be **subtle** on T1 C+ **MR**
- Use CT liberally in negative or equivocal MR
- ## Image Interpretation Pearls
- Poorly circumscribed, C+ lesion in geniculate fossa in setting of CNVII paralysis is most likely FNVM
ba26f431-c00d-4d38-b485-6267fa52965a
## References
# Selected References
1. [Rao D et al: A case of a facial nerve venous malformation presenting with crocodile tear syndrome. Surg Neurol Int. 11:3, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=31966922%5Bpmid%5D)
1. [Bonali M et al: Endoscopic transcanal approach to geniculate ganglion hemangioma and simultaneous facial nerve reinnervation: a case report. J Int Adv Otol. 15(1):165-68, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=30924777%5Bpmid%5D)
1. [Guerin JB et al: Facial nerve venous malformation: a radiologic and histopathologic review of 11 cases. Laryngoscope Investig Otolaryngol. 4(3):347-52, 2019](http://www.ncbi.nlm.nih.gov/pubmed/?term=31236470%5Bpmid%5D)
1. [ISSVA International Society for the Study of Vascular Anomalies. Published May 2018. Accessed 1/30/2021. https://www.issva.org/classification](https://www.issva.org/classification)
1. [Wick CC et al: Transcanal endoscopic ear surgery for excision of a facial nerve venous malformation with interposition nerve grafting: a case report. Otol Neurotol. 38(6):895-9, 2017](http://www.ncbi.nlm.nih.gov/pubmed/?term=28498268%5Bpmid%5D)
1. [Lahlou G et al: Geniculate ganglion tumors: clinical presentation and surgical results. Otolaryngol Head Neck Surg. 155(5):850-5, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27484229%5Bpmid%5D)
1. [Maiodna E et al: Cavernous malformation of the seventh cranial nerve: case report and review of literature. World Neurosurg. 91:676.e13-21, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27155386%5Bpmid%5D)
1. [Omor Y et al: "Honeycomb" sign. Presse Med. 45(5):541-3, 2016](http://www.ncbi.nlm.nih.gov/pubmed/?term=27062115%5Bpmid%5D)
1. [Yue Y et al: Retrospective case series of the imaging findings of facial nerve hemangioma. Eur Arch Otorhinolaryngol. 272(9):2497-503, 2015](http://www.ncbi.nlm.nih.gov/pubmed/?term=25108340%5Bpmid%5D)
1. [Ma X et al: Facial nerve preservation in geniculate ganglion hemangiomas. Acta Otolaryngol. 134(9):974-6, 2014](http://www.ncbi.nlm.nih.gov/pubmed/?term=24930913%5Bpmid%5D)
1. [Benoit MM et al: Facial nerve hemangiomas: vascular tumors or malformations? Otolaryngol Head Neck Surg. 142(1):108-14, 2010](http://www.ncbi.nlm.nih.gov/pubmed/?term=20096233%5Bpmid%5D)
1. [Greene AK et al: Intraosseous "hemangiomas" are malformations and not tumors. Plast Reconstr Surg. 119(6):1949-50; author reply 1950, 2007](http://www.ncbi.nlm.nih.gov/pubmed/?term=17440384%5Bpmid%5D)
1. [Isaacson B et al: Hemangiomas of the geniculate ganglion. Otol Neurotol. 26(4):796-802, 2005](http://www.ncbi.nlm.nih.gov/pubmed/?term=16015187%5Bpmid%5D)
1. [Bernardeschi D et al: Vascular malformation (so-called hemangioma) of Scarpa's ganglion. Acta Otolaryngol. 124(9):1099-102, 2004](http://www.ncbi.nlm.nih.gov/pubmed/?term=15513557%5Bpmid%5D)
1. [Piccirillo E et al: Management of temporal bone hemangiomas. Ann Otol Rhinol Laryngol. 113(6):431-7, 2004](http://www.ncbi.nlm.nih.gov/pubmed/?term=15224824%5Bpmid%5D)
1. [Achilli V et al: Facial nerve hemangioma. Otol Neurotol. 23(6):1003-4, 2002](http://www.ncbi.nlm.nih.gov/pubmed/?term=12438871%5Bpmid%5D)
1. [Friedman O et al: Temporal bone hemangiomas involving the facial nerve. Otol Neurotol. 23(5):760-6, 2002](http://www.ncbi.nlm.nih.gov/pubmed/?term=12218631%5Bpmid%5D)
1. [Salib RJ et al: The crucial role of imaging in detection of facial nerve haemangiomas. J Laryngol Otol. 115(6):510-3, 2001](http://www.ncbi.nlm.nih.gov/pubmed/?term=11429083%5Bpmid%5D)
1. [Dufour JJ et al: Intratemporal vascular malformations (angiomas): particular clinical features. J Otolaryngol. 23(4):250-3, 1994](http://www.ncbi.nlm.nih.gov/pubmed/?term=7996623%5Bpmid%5D)
1. [Martin N et al: Haemangioma of the petrous bone: MRI. Neuroradiology. 34(5):420-2, 1992](http://www.ncbi.nlm.nih.gov/pubmed/?term=1407526%5Bpmid%5D)
1. [Shelton C et al: Intratemporal facial nerve hemangiomas. Otolaryngol Head Neck Surg. 104(1):116-21, 1991](http://www.ncbi.nlm.nih.gov/pubmed/?term=1900607%5Bpmid%5D)
1. [Lo WW et al: Intratemporal vascular tumors: detection with CT and MR imaging. Radiology. 171(2):445-8, 1989](http://www.ncbi.nlm.nih.gov/pubmed/?term=2704809%5Bpmid%5D)
1. [Curtin HD et al: "Ossifying" hemangiomas of the temporal bone: evaluation with CT. Radiology. 164(3):831-5, 1987](http://www.ncbi.nlm.nih.gov/pubmed/?term=3112865%5Bpmid%5D)
1. [Mulliken JB et al: Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg. 69(3):412-22, 1982](http://www.ncbi.nlm.nih.gov/pubmed/?term=7063565%5Bpmid%5D)
## Differential diagnosis
### Bony Lesions of Temporal Bone
DDX:a33cf59d-2d6e-40cb-960e-4e1e37066d09
### Facial Nerve Lesion, Temporal Bone
DDX:1428754b-a8ee-48a0-98f8-4faeebf8dbab
### Inner Ear Lesion, Adult
DDX:e5bbf757-d77a-4546-a848-d1a1a64cb230
### Peripheral Facial Nerve Paralysis
DDX:4da52ac4-c03c-4711-ae7e-bb4f2f7c5ab8
## Anatomy
### Facial Nerve (CNVII)
Brain/ANATOMY:2f4818dd-6438-405b-8561-5cbbb9c91562
### Vestibulocochlear Nerve (CNVIII)
Brain/ANATOMY:498e844d-faca-4c6a-bff1-9c6ad4993e62
### Middle Ear-Mastoid Anatomy
Head and Neck/ANATOMY:99aff289-b689-4693-9b41-2adbbda59179
### Inner Ear Anatomy
Head and Neck/ANATOMY:48ee77aa-d460-43f3-a3e2-9fd61632ca4a
### CNVII (Facial Nerve)
Head and Neck/ANATOMY:98cb2d45-e64c-4295-9662-3470cd46513a
### CNVIII (Vestibulocochlear Nerve)
Head and Neck/ANATOMY:e9917c41-94c9-46aa-b9d8-b196c375d35b
## Cases
- {'cases': [{'authors': [{'key': '33151213-01b2-4542-9105-342e006b3915', 'value': 'H. Ric Harnsberger, MD'}, {'key': '94f835c8-fa13-4e8a-995b-53048e6b0605', 'value': 'Philip R. Chapman, MD'}], 'caseVersionId': '151a88e3-b12d-4b87-8615-71fe3ee561ba', 'description': 'Typical T-bone CT case of ossifying facial nerve hemangioma (FNH) of the geniculate fossa.\n\nThree T-bone CT images of the right ear presented from superior to inferior show an enlarged geniculate fossa (arrow, #1-3) filled by the FNH. Within the tissue of the lesion there is visible punctate areas ossification (open arrow, #1-3) making this an "ossifying hemangioma". On the two coronal T-bone CT images shown (#4,5) the hemangioma in the enlarged geniculate fossa (arrow) is again seen with its areas of ossification (open arrow). Notice the ovoid soft tissue area just inferolateral to the FNH on the upper cochlear promontory (curved arrow). This is the belly of the tensor tympani muscle.\n\nAxial T2 MR image (#6) shows tissue in the enlarged geniculate fossa (arrow) with low signal foci (open arrow) from intratumoral ossifications. Axial (#7,8) and coronal (#9) enhanced T1 MR images show the FNH enhances (arrow, #7,9). Again punctate low signal can be seen in the tumor matrix (open arrow, #8). \n\nPearl: About 50% of FNH are show areas of ossification. When seen in larger lesions the term "honeycomb ossification" may be applied. The geniculate ganglion is the most common location for FNH to be found within the T-bone.', 'history': 'Patient presents with history of acute onset of right facial nerve paralysis that did not resolve over 6 weeks. Initially called "Bell palsy" by referring clinician, MR was then completed looking for other causes of the facial nerve paralysis.', 'imagePoolId': '9f4fe8af-d0a3-4261-808f-af1426bc1118', 'name': 'Ossifying, geniculate fossa', 'teachingPoint': None, 'demographics': '31 Years old female'}, {'authors': [{'key': '624acd80-0502-4325-be71-e68fec740eb3', 'value': 'Richard H. Wiggins, III, MD, CIIP, FSIIM, FAHSE, FACR'}], 'caseVersionId': '61b1875a-9bb5-4f3b-a122-b23321928abe', 'description': 'This is a typical case of a facial nerve hemangioma.\n\nThe axial bone algorithm CT images (#1-3) show the abnormal osseous density in the region of the left geniculate ganglion (arrow). The mass seen arising from the geniculate ganglion is associated with loss of normal bone density at this site, and extends posteriorly, just medial and anterior to the inner ear ossicles (open arrow). The coronal bone algorithm CT images (#4-5) also show the abnormal osseous density at the anterior genu of the facial nerve (arrow), which extends posteriorly, to a location just medial to the ossicles (open arrow).\n\nThe axial T2 weighted image (#6) shows abnormal increased signal intensity at the left geniculate ganglion (arrow). The axial (#7) and the coronal (#8) images show the abnormal enhancement at the left geniculate ganglion (arrow), consistent with a facial nerve hemangioma.', 'history': 'Patient presented with a history of acute onset left facial nerve paralysis that remitted after one week.', 'imagePoolId': '9da9b6eb-b694-4755-8b07-a5a75f7cb034', 'name': 'Lateral geniculate', 'teachingPoint': None, 'demographics': '65 Years old female'}, {'authors': [{'key': '33151213-01b2-4542-9105-342e006b3915', 'value': 'H. Ric Harnsberger, MD'}], 'caseVersionId': '80cc900c-dae5-478d-a7be-2809aa8eb694', 'description': 'Typical CT and MR case of a large geniculate fossa facial nerve hemangioma with subtle ossific matrix.\n\nAxial (#1-4) and coronal (#5-6) T-bone CT images reveal a lesion in the right geniculate ganglion (arrow, #1-3) with extension along the anteromedial surface of the temporal bone (curved arrow). Note the enlarged, tumor filled labyrinthine segment of the facial nerve (open arrow, #1). In the coronal CT images (#5, 6) the geniculate fossa tumor (arrow) is again seen with spread along the cephalad surface of the temporal bone particularly apparent (open arrows). \n\nEnhanced MR images (axial, #7-9 and coronal, #10-12) demonstrate the hemangioma as an enhancing mass (arrow) that is larger than that perceived in the CT images. Coronal image #10 reveals the tumor in the labyrinthine segment of the facial nerve (open arrow).\n\nPearl: The crescentic shape of the lesion seen on axial CT arching around the cochlea medially on anterior surface of the temporal bone is typical of large facial nerve hemangiomas in this location.', 'history': 'Patient presents with right-sided peripheral facial nerve paralysis originally thought to be Bell palsy. When paralysis did not improve over a 2 month period, CT & MR images completed of the temporal bone.', 'imagePoolId': 'e6c0b56d-046d-425e-9c23-9f8694defa20', 'name': 'Large, subtle ossific matrix', 'teachingPoint': None, 'demographics': '52 Years old female'}, {'authors': [{'key': '624acd80-0502-4325-be71-e68fec740eb3', 'value': 'Richard H. Wiggins, III, MD, CIIP, FSIIM, FAHSE, FACR'}, {'key': '94f835c8-fa13-4e8a-995b-53048e6b0605', 'value': 'Philip R. Chapman, MD'}], 'caseVersionId': '85f20b2e-8a1a-425a-badf-a67dc89e7b85', 'description': 'This is a classic CT and MRI facial nerve hemangioma case.\n\nThe axial bone algorithm CT images (#1-2) show the unusual calcifications within the geniculate fossa (arrow).\n\nThe axial post-contrast T1 weighted images (#3-5) show the avid enhancement of the anterior genu of the facial nerve (arrow). The oblique sagittal image (#6) shows enhancement at the geniculate fossa (arrow) as well as the tympanic segment (open arrow), posterior genu, and descending (mastoid) segment (curved arrow) of the facial nerve.', 'history': 'Patient presented with a rapid onset of left facial nerve paralysis.', 'imagePoolId': 'd8915c51-5df7-4779-88fd-4a6fd2057b37', 'name': 'Rapid growth', 'teachingPoint': None, 'demographics': '45 Years old female'}, {'authors': [{'key': '624acd80-0502-4325-be71-e68fec740eb3', 'value': 'Richard H. Wiggins, III, MD, CIIP, FSIIM, FAHSE, FACR'}], 'caseVersionId': 'e6480ed9-39c7-4635-80cb-7d18d2280712', 'description': 'This is a classic case of a facial nerve hemangioma at the geniculate ganglion.\n\nThe axial bone algorithm CT images (#1-2) show the abnormal bony spicules (arrow) at the geniculate ganglion.\n\nThe axial post-contrast T1 weighted images (#3-4) show avid enhancement near the geniculate ganglion (arrow) correlating with the CT region of loss of bone density.', 'history': 'Patient presented with slowly progressive left facial nerve paralysis.', 'imagePoolId': '3488e8b3-51f1-4d3b-822f-c72d03db18b7', 'name': 'Classic', 'teachingPoint': None, 'demographics': '25 Years old female'}, {'authors': [{'key': '624acd80-0502-4325-be71-e68fec740eb3', 'value': 'Richard H. Wiggins, III, MD, CIIP, FSIIM, FAHSE, FACR'}], 'caseVersionId': '1ec6d174-59ca-435f-a04d-0bb7d4fcb74a', 'description': 'This is a classic case of a facial nerve ossifying hemangioma.\n\nThe axial bone algorithm CT images (#1, 2) demonstrate the honeycombing appearance (arrow) of the lesion at the geniculate fossa. There is extension of the ossification along the proximal tympanic segment (open arrow, #2). The coronal CT images (#3-6) also show the ossification at the geniculate fossa (arrow).\n\nThe axial T1 post-contrast images (#7, 8) and the coronal post-contrasted images (#9-10) show the avid enhancement at the geniculate fossa (arrow, #7, 9, 10). Note extension along tympanic segment of facial nerve (open arrow, #7).', 'history': 'Patient presented with chronic facial paralysis.', 'imagePoolId': 'da1af59f-0fc1-4d4b-9ae3-5bb2f772dd92', 'name': 'Ossifying', 'teachingPoint': None, 'demographics': '46 Years old male'}, {'authors': [{'key': '624acd80-0502-4325-be71-e68fec740eb3', 'value': 'Richard H. Wiggins, III, MD, CIIP, FSIIM, FAHSE, FACR'}], 'caseVersionId': '2b2cf5ba-8647-4713-95de-9953103b8708', 'description': 'This is a typical case of facial nerve hemangioma.\n\nThe axial bone algorithm CT images (#1-4) show the abnormal osseous density at the right anterior genu of the facial nerve (arrow). There is also extension of abnormal osseous density along the tympanic segment of the facial nerve (open arrow). The coronal CT images (#5-7) show the abnormal loss of bone density at the right geniculate ganglion (arrow).\n\nThe coronal T2 weighted image (#8) shows the abnormal increased signal intensity at the right anterior genu of the facial nerve (arrow). The axial post-contrast T1 weighted image (#9) and the coronal image (#10) show the abnormal enhancement at the right geniculate ganglion (arrow).', 'history': 'Patient presented with right sided hearing loss.', 'imagePoolId': 'da51d06a-3bbd-44a3-8057-33e6d52a9c48', 'name': 'Classic', 'teachingPoint': None, 'demographics': '40 Years old male'}, {'authors': [{'key': '624acd80-0502-4325-be71-e68fec740eb3', 'value': 'Richard H. Wiggins, III, MD, CIIP, FSIIM, FAHSE, FACR'}], 'caseVersionId': '4c1d64eb-b8c1-4089-990d-5b5801030581', 'description': 'This is a typical facial nerve hemangioma case.\n\nThe axial bone algorithm CT images (#1-2) show the laminated osseous deposition at the left geniculate ganglion (arrow).\n\nThe axial post-contrast T1 weighted images (#3-4) show the abnormal enhancement at the left geniculate ganglion (arrow). The coronal post-contrast images (#5-6) also show the abnormal enhancement at the anterior genu of the left facial nerve (arrow).', 'history': None, 'imagePoolId': '0842164c-2b9f-447d-a984-a8ac7ba3c3da', 'name': 'Classic', 'teachingPoint': None}, {'authors': [{'key': '624acd80-0502-4325-be71-e68fec740eb3', 'value': 'Richard H. Wiggins, III, MD, CIIP, FSIIM, FAHSE, FACR'}], 'caseVersionId': 'f6d47f77-0b7b-42d8-a832-66487719bcd1', 'description': 'This is a classic case of a facial nerve hemangioma at the anterior genu of the facial nerve.\n\nThe axial bone algorithm CT images (#1-4) show the laminated appearance of osseous deposition at the left geniculate ganglion (arrow), compared to the normal appearing osseous anatomic landscape at the right geniculate ganglion (open arrow).\n\nThe axial post-contrast T1 weighted images (#5-8) show the abnormal enhancement at the left geniculate ganglion (arrow), compared to the normal relative lack of enhancement in the region of the right geniculate ganglion (open arrow). The coronal post-contrast T1 weighted images also show the abnormal avid enhancement at the left geniculate ganglion (arrow), compared to the relative lack of enhancement in the region of the right ganglion (open arrow).', 'history': 'Patient presented with a 2 year history of worsening left facial nerve palsy, an "atypical Bell\'s palsy".', 'imagePoolId': '8aa84b20-5b7a-4ab3-a889-e7ebdcae04d1', 'name': 'Classic', 'teachingPoint': None, 'demographics': '42 Years old male'}], 'caseType': 'typical', 'name': 'TYPICAL'}
- {'cases': [{'authors': [{'key': '33151213-01b2-4542-9105-342e006b3915', 'value': 'H. Ric Harnsberger, MD'}, {'key': 'ab4396df-0647-4f6a-b534-995eda06646c', 'value': 'Nancy J. Fischbein, MD'}], 'caseVersionId': 'a7e74b0c-83f0-4c72-a092-8d063715beba', 'description': 'Variant case of facial nerve hemangioma (FNH)(venous malformation) involving the areas of the geniculate fossa and the internal auditory canal simultaneously.\n\nAxial (#1-3) and coronal (#4-6) temporal bone CT images show an intraosseous venous malformation (FNH) with the bone anteromedial to the geniculate fossa (arrows, #1-3,5-6) and around the geniculate fossa (curved arrows, #2-3,6). Subtle calcification in the internal auditory canal (IAC)(open arrows, #2-3,4-5) is visible. \n\nAxial T1 (#7-9), T2 (#10-11), and FLAIR (#12) MR reveals intraosseous component anteromedial to the geniculate ganglion (arrows, #7-8,10-11) and around the geniculate ganglion (curved arrows, #8-9,11). Signal in the IAC (open arrows, #9,12) indicates that the venous malformation (FNH) involves this area as well.\n\nEnhanced axial (#13-15) and coronal (#16-17) fat-saturated MR images demonstrate that the venous malformation (FNH) enhances in the medial temporal bone (arrows, #13-14,16-17), around the geniculate ganglion (curved arrows, #14-15,17), and in the IAC (open arrows, #15-16).', 'history': 'Patient presents with history of vertigo, left-sided hearing loss, and mild facial weakness. Referred for focused radiation therapy as "left vestibular schwannoma."', 'imagePoolId': '63023f4e-221d-42fb-8157-e7fb9ebbf4fa', 'name': 'Geniculate fossa area, IAC involvement', 'teachingPoint': 'This "ossifying" facial nerve hemangioma is most likely a "calcified venous malformation of the temporal bone." When the tissue is submitted to immunoanalysis, it is found to be GLUT1/LeY antigen and podoplanin negative, indicating that venous malformation is the better term for this lesion. Hemangiomas are GLUT1 and LeY antigen positive, with podoplanin positivity present if the lesion is a lymphatic malformation.', 'demographics': '38 Years old male'}], 'caseType': 'variant', 'name': 'VARIANT'}
## Images
### Selected Images
 of the temporal bone. Notice the honeycomb bone within the lesion matrix.](images/app.statdx.com_image_thumbnail_bc08df2b-cdf5-4378-8bd1-cc6052e72358_annotated_true_size_900_quality_90_abab398a0e88180ed2590ba08a323c5996e1511e.jpg)
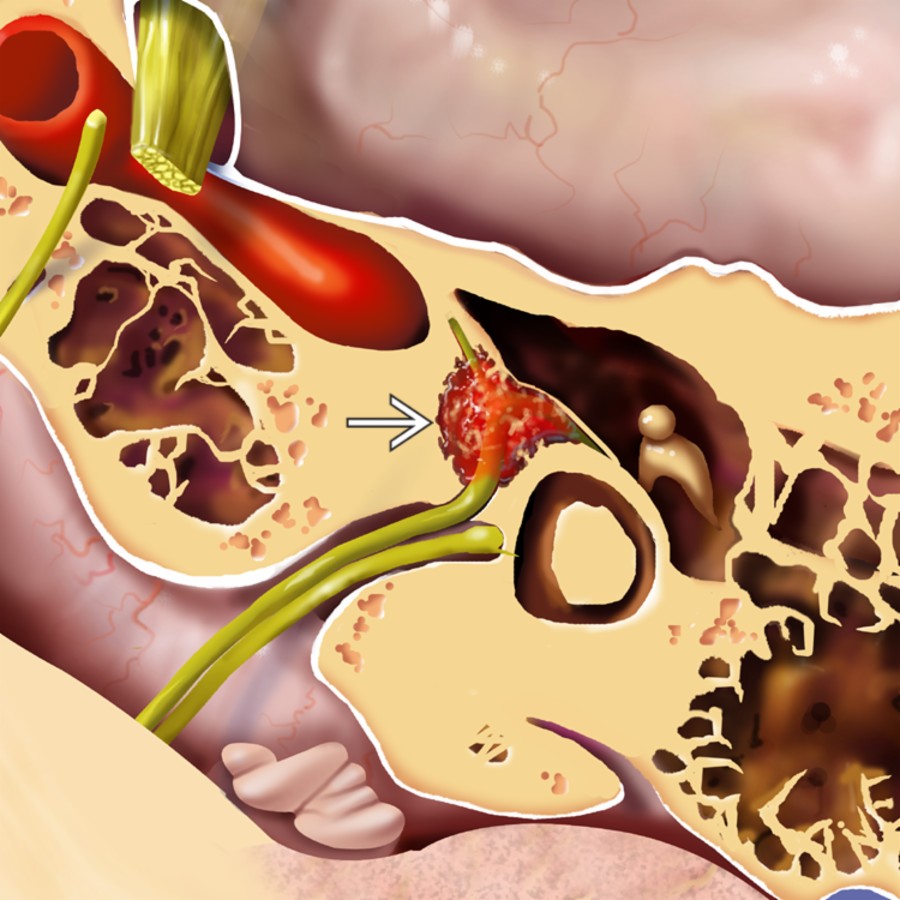
*Axial graphic illustrates a classic example of a medium-sized facial nerve venous malformation (FNVM) centered in the geniculate fossa of the temporal bone. Notice the honeycomb bone within the lesion matrix.*

*Axial graphic illustrates a classic example of a medium-sized facial nerve venous malformation (FNVM) centered in the geniculate fossa of the temporal bone. Notice the honeycomb bone within the lesion matrix.*
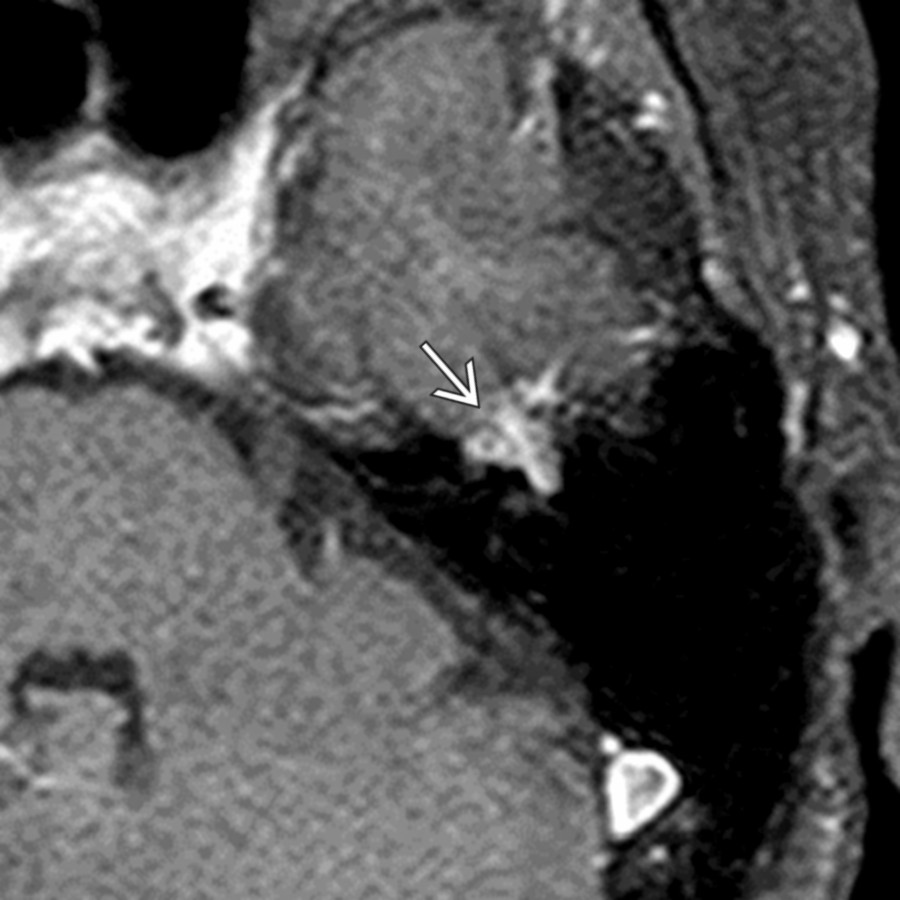
*Axial T1 C+ MR with fat saturation in a patient with left atypical Bell palsy reveals a classic left geniculate fossa enhancing FNVM . Punctate areas of high density on bone CT (not shown) confirmed this imaging impression.*
*Axial graphic illustrates a classic example of a medium-sized facial nerve venous malformation (FNVM) centered in the geniculate fossa of the temporal bone. Notice the honeycomb bone within the lesion matrix.*

*Axial graphic illustrates a classic example of a medium-sized facial nerve venous malformation (FNVM) centered in the geniculate fossa of the temporal bone. Notice the honeycomb bone within the lesion matrix.*

*Axial T1 C+ MR with fat saturation in a patient with left atypical Bell palsy reveals a classic left geniculate fossa enhancing FNVM . Punctate areas of high density on bone CT (not shown) confirmed this imaging impression.*
 .](images/app.statdx.com_image_thumbnail_57257255-49fe-4245-a7b3-2e475a5639f5_annotated_true_size_900_quality_90_25b6468b97fad9842b08cf50671c6657dedaae73.jpg)
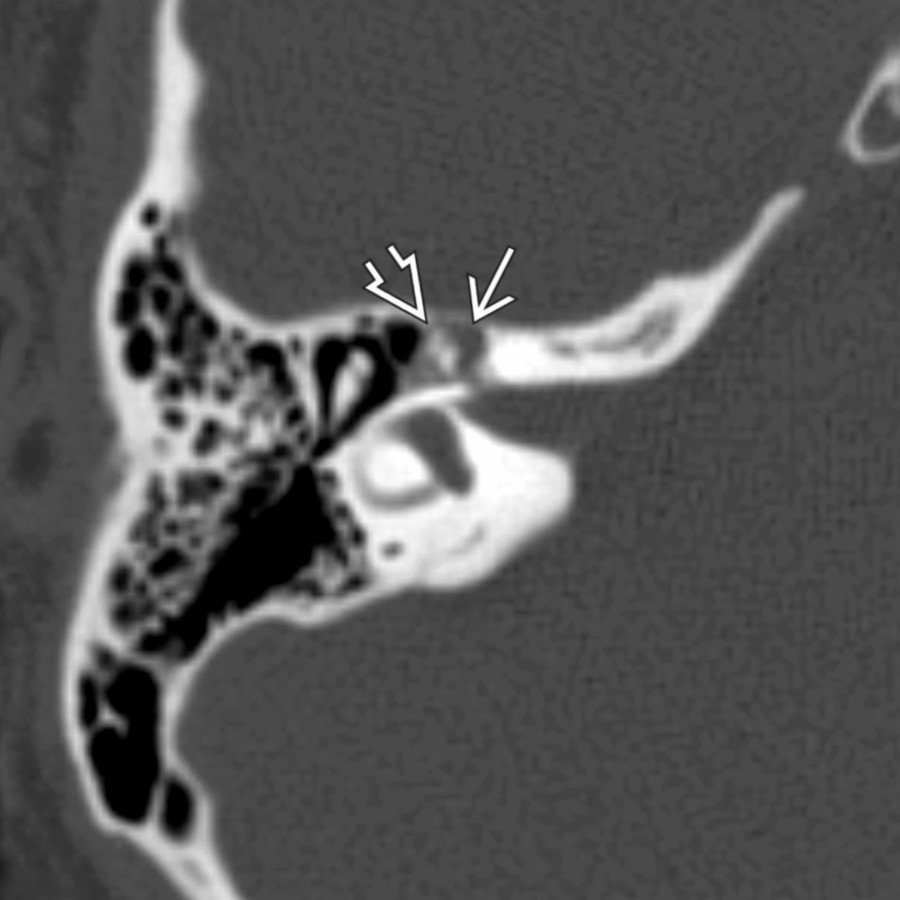
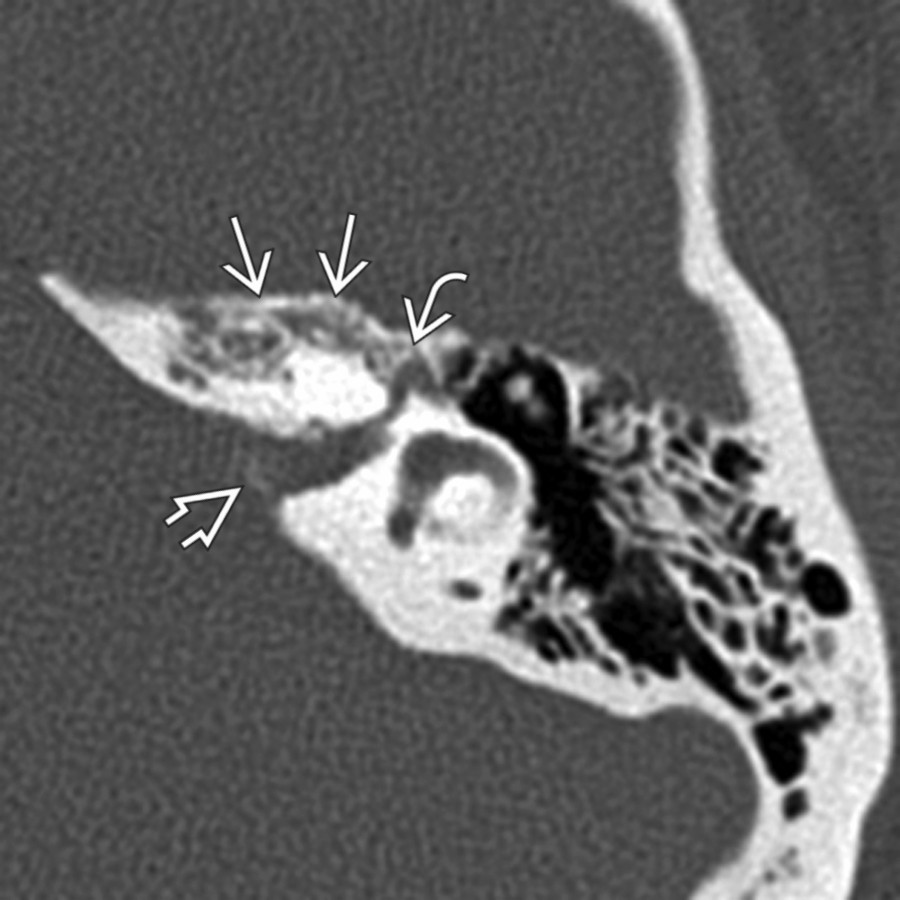
*Axial bone CT demonstrates the honeycombing appearance of FNVM centered in the geniculate fossa . Note extension of the lesion along the proximal tympanic CNVII segment .*

*Axial bone CT demonstrates the honeycombing appearance of FNVM centered in the geniculate fossa . Note extension of the lesion along the proximal tympanic CNVII segment .*
 and into the fundus of the internal auditory canal (IAC)
and into the fundus of the internal auditory canal (IAC)  . IAC extension occurred via the labyrinthine segment of CNVII (not shown).](images/app.statdx.com_image_thumbnail_e3aa7cbf-dea7-4bfd-b5da-9a9d59f7028e_annotated_true_size_900_quality_90_f217daaf08610eeec04cf81a7a877118ec1817d5.jpg)
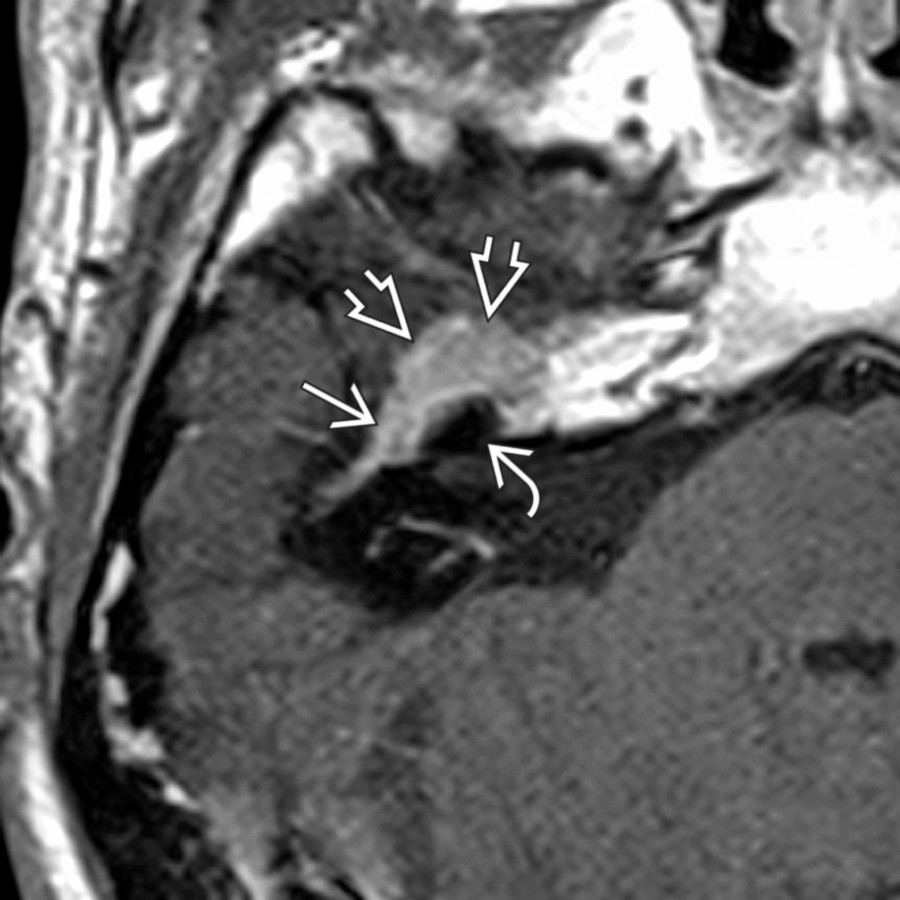
*Axial T1 C+ MR in the same patient shows a poorly marginated, avidly enhancing lesion in the geniculate fossa . Note extension along the tympanic segment of CNVII and into the fundus of the internal auditory canal (IAC) . IAC extension occurred via the labyrinthine segment of CNVII (not shown).*
*Axial bone CT in a patient with right facial nerve palsy shows a small FNVM in the geniculate fossa . Notice the punctate ossific foci within the lesion. This finding allows differentiation of FNVM from facial nerve schwannoma, which also occurs most frequently in the geniculate fossa.*

*Axial T1 C+ MR with fat saturation in the same patient reveals FNVM enhancing in the geniculate ganglion. The punctate ossific area is seen as an intralesional low-signal focus .*

*Axial bone CT through the right temporal bone demonstrates a medium-sized FNVM in the geniculate fossa with extension along the anteromedial surface of the temporal bone . The crescentic shape of this lesion arching around the cochlea medially on the anterior temporal bone surface is typical of FNVM.*
*Axial T1 C+ MR in the same patient shows diffuse FNVM enhancement in the geniculate fossa , arching around the cochlea along the anteromedial temporal bone surface .*
*Axial bone CT shows an FNVM within the anteromedial temporal bone and in the bone surrounding the geniculate fossa . Subtle foci of increased density are also seen in the IAC.*

*Axial T1 C+ FS MR in the same patient shows the venous malformation enhancing in the anteromedial temporal bone , around the geniculate ganglion , and in the IAC . The IAC lobe of FNVM occurs due to extension along the labyrinthine segment of CNVII (not shown).*
### Additional Images

*Axial left ear temporal bone CT reveals a typical medium-sized FNVM hemangioma) emanating from the geniculate fossa around the anterior cochlear surface. Note relative sparing of the otic capsule.*

*Axial T1 C+ MR in the same patient shows diffuse enhancement of a medium-sized FNVM (hemangioma) . MR is not fat saturated, making it difficult to distinguish petrous apex fatty marrow from this developmental lesion.*

*Axial temporal bone CT reveals a very small FNVM (hemangioma) as a single dot of high-density matrix within a mildly enlarged geniculate fossa. Note adjacent otic capsule involvement . Radiologists beware, as this would be easily missed.*

*Axial T1 C+ MR in the same patient demonstrates a tiny enhancing FNVM (hemangioma) in the location of the geniculate ganglion in this patient with acute-onset peripheral facial nerve paralysis. Also note the lesion involves the adjacent otic capsule .*
. IAC extension occurred via the labyrinthine segment of CNVII (not shown).](images/app.statdx.com_image_thumbnail_e3aa7cbf-dea7-4bfd-b5da-9a9d59f7028e_annotated_true_size_900_quality_90_f217daaf08610eeec04cf81a7a877118ec1817d5.jpg)
*Axial T1 C+ MR in the same patient shows a poorly marginated, avidly enhancing lesion in the geniculate fossa . Note extension along the tympanic segment of CNVII and into the fundus of the internal auditory canal (IAC) . IAC extension occurred via the labyrinthine segment of CNVII (not shown).*

*Axial bone CT in a patient with right facial nerve palsy shows a small FNVM in the geniculate fossa . Notice the punctate ossific foci within the lesion. This finding allows differentiation of FNVM from facial nerve schwannoma, which also occurs most frequently in the geniculate fossa.*

*Axial T1 C+ MR with fat saturation in the same patient reveals FNVM enhancing in the geniculate ganglion. The punctate ossific area is seen as an intralesional low-signal focus .*

*Axial bone CT through the right temporal bone demonstrates a medium-sized FNVM in the geniculate fossa with extension along the anteromedial surface of the temporal bone . The crescentic shape of this lesion arching around the cochlea medially on the anterior temporal bone surface is typical of FNVM.*

*Axial T1 C+ MR in the same patient shows diffuse FNVM enhancement in the geniculate fossa , arching around the cochlea along the anteromedial temporal bone surface .*

*Axial bone CT shows an FNVM within the anteromedial temporal bone and in the bone surrounding the geniculate fossa . Subtle foci of increased density are also seen in the IAC.*

*Axial T1 C+ FS MR in the same patient shows the venous malformation enhancing in the anteromedial temporal bone , around the geniculate ganglion , and in the IAC . The IAC lobe of FNVM occurs due to extension along the labyrinthine segment of CNVII (not shown).*
### Additional Images

*Axial left ear temporal bone CT reveals a typical medium-sized FNVM hemangioma) emanating from the geniculate fossa around the anterior cochlear surface. Note relative sparing of the otic capsule.*

*Axial T1 C+ MR in the same patient shows diffuse enhancement of a medium-sized FNVM (hemangioma) . MR is not fat saturated, making it difficult to distinguish petrous apex fatty marrow from this developmental lesion.*

*Axial temporal bone CT reveals a very small FNVM (hemangioma) as a single dot of high-density matrix within a mildly enlarged geniculate fossa. Note adjacent otic capsule involvement . Radiologists beware, as this would be easily missed.*

*Axial T1 C+ MR in the same patient demonstrates a tiny enhancing FNVM (hemangioma) in the location of the geniculate ganglion in this patient with acute-onset peripheral facial nerve paralysis. Also note the lesion involves the adjacent otic capsule .*