---
title: "Elevated or Deformed Hemidiaphragm"
docid: "208baaa2-8772-4560-af34-46ce757edcb9"
authors:
- key: "c1df94ab-4a9f-44c4-add7-1f174fb9ac45"
value: "Siva P. Raman, MD"
breadcrumbs:
-
name: "Gastrointestinal"
slug: "gastrointestinal"
treeNodeId: "b52263f7-5978-4a22-a17d-7260e0033943"
-
name: "Differential Diagnosis"
slug: "differential-diagnosis"
treeNodeId: "a0fd80ff-6231-49d3-94b8-ea083449979d"
-
name: "Abdominal Wall"
slug: "abdominal-wall"
treeNodeId: "08db01f7-2961-47f7-954d-2a5fca7e707d"
-
name: "Anatomically Based Differentials"
slug: "anatomically-based-differentials"
treeNodeId: "1525b44f-9d47-4ff4-8330-693211bd5eb5"
-
name: "Elevated or Deformed Hemidiaphragm"
slug: "elevated-or-deformed-hemidiaphragm"
treeNodeId: null
category: "Gastrointestinal"
documentVersionId: "c5d9083d-d7a6-430b-9be6-4a6013d67387"
imageCount: 18
lastUpdated: "07/01/22"
pageDescription: "Elevated or Deformed Hemidiaphragm"
pageKeywords: "Gastrointestinal, Differential Diagnosis, Abdominal Wall, Anatomically Based Differentials, Elevated or Deformed Hemidiaphragm"
pageTitle: "Elevated or Deformed Hemidiaphragm | STATdx"
enhancedTitle: "Elevated or Deformed Hemidiaphragm"
type: "DDX"
references: true
breadcrumbs:
- "Gastrointestinal"
- "Differential Diagnosis"
- "Abdominal Wall"
- "Anatomically Based Differentials"
- "Elevated or Deformed Hemidiaphragm"
---
# ESSENTIAL INFORMATION
- ## Key Differential Diagnosis Issues
- Axial CT suboptimal for distinguishing diaphragm from spleen, liver, and muscle and identifying many diaphragmatic abnormalities
- Multiplanar reformations critical for accurate diagnosis
- Diaphragm easier to visualize discretely on MR compared to CT and can demonstrate diaphragm in multiple planes
- Fluoroscopy and US useful for providing functional information, particularly for paralysis
- Dynamic MR (not widely utilized) can provide functional information similar to US or fluoroscopy
- US in sagittal plane easily identifies diaphragm and location of peridiaphragmatic fluid collection
- Ascites and abdominal contents lie medial to and within confines of diaphragm
- Pleural fluid and thoracic contents lie outside confines of diaphragm
- ## Helpful Clues for Common Diagnoses
- **Paralyzed Diaphragm**
- Normal diaphragm that fails to contract secondary to abnormalities of brain, spinal cord, neuromuscular junction, phrenic nerve, or muscle
- US or fluoroscopy demonstrate no motion or paradoxical (upward) motion during inspiration or sniff test
- **Eventration of Diaphragm**
- Congenital thinning/weakness of portion of diaphragm, which normally attaches to costal margin
- Eccentric diaphragmatic contour (usually anteromedial right hemidiaphragm) ± paradoxical motion with large eventrations
- **Hiatal Hernia**
- Herniation of abdominal contents into thoracic cavity through esophageal hiatus
- Divided into sliding type (GE junction displaced upward through hiatus) and paraesophageal type (GE junction in normal location with stomach herniating above diaphragm)
- **Bochdalek Hernia**
- Type of congenital diaphragmatic hernia due to defect in posterolateral diaphragm (usually on left side)
- Hernia may contain retroperitoneal fat, bowel, kidney, stomach, spleen, or liver
- **Morgagni Hernia**
- Type of congenital diaphragmatic hernia due to defect in retrosternal diaphragm (usually on right side)
- Usually located in right cardiophrenic angle and most often contains just omental fat (but can contain colon, liver, small bowel, or stomach)
- **Traumatic Diaphragmatic Hernia**
- Traumatic injury may be due to blunt or penetrating trauma
- Multiple imaging signs of injury include dependent viscus sign, collar sign, and dangling diaphragm sign
- Injuries both above and below diaphragm should raise concern for diaphragmatic injury
- **Subdiaphragmatic Mass**
- Tumor, hepatomegaly, or splenomegaly can exert mass effect and raise ipsilateral diaphragm
- **Abdominal****Abscess**
- Subphrenic abscess can cause upward displacement of diaphragm due to mass effect or splinting (decreased motion of diaphragm due to pain)
- **Unilateral Lung Volume Loss**
- Diminished unilateral lung volume (lung resection, atelectasis) will cause elevation of ipsilateral diaphragm
- **Subpulmonic Pleural Effusion (Mimic)**
- Pleural fluid loculated in subpulmonic pleural space will displace lung upward and may simulate elevated diaphragm on radiographs (but not on cross-sectional imaging)
## References
# Selected References
1. [Abdellatif W et al: Unravelling the mysteries of traumatic diaphragmatic injury: an up-to-date review. Can Assoc Radiol J. 71(3):313-21, 2020](http://www.ncbi.nlm.nih.gov/pubmed/?term=32157897%5Bpmid%5D)
1. [Kharma N: Dysfunction of the diaphragm: imaging as a diagnostic tool. Curr Opin Pulm Med. 19(4):394-8, 2013](http://www.ncbi.nlm.nih.gov/pubmed/?term=23715292%5Bpmid%5D)
1. [Nason LK et al: Imaging of the diaphragm: anatomy and function. Radiographics. 32(2):E51-70, 2012](http://www.ncbi.nlm.nih.gov/pubmed/?term=22411950%5Bpmid%5D)
1. [Roberts HC: Imaging the diaphragm. Thorac Surg Clin. 19(4):431-50, v, 2009](http://www.ncbi.nlm.nih.gov/pubmed/?term=20112626%5Bpmid%5D)
1. [Verhey PT et al: Differentiating diaphragmatic paralysis and eventration. Acad Radiol. 2007 Apr;14(4):420-5](http://www.ncbi.nlm.nih.gov/pubmed/?term=17368210%5Bpmid%5D)
1. [Eren S et al: Imaging of diaphragmatic rupture after trauma. Clin Radiol. 61(6):467-77, 2006](http://www.ncbi.nlm.nih.gov/pubmed/?term=16713417%5Bpmid%5D)
1. [Eren S et al: Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol. 54(3):448-59, 2005](http://www.ncbi.nlm.nih.gov/pubmed/?term=15899350%5Bpmid%5D)
## Images
### Selected Images
 is paralyzed due to phrenic nerve involvement by the patient's mediastinal lymphoma (not shown).](images/app.statdx.com_image_thumbnail_27987cfb-8854-4a96-a958-9493891fa27f_annotated_true_size_900_quality_90_2fe0bc4785f5babcbbcfe01b8e100034c4fdc97e.jpg)
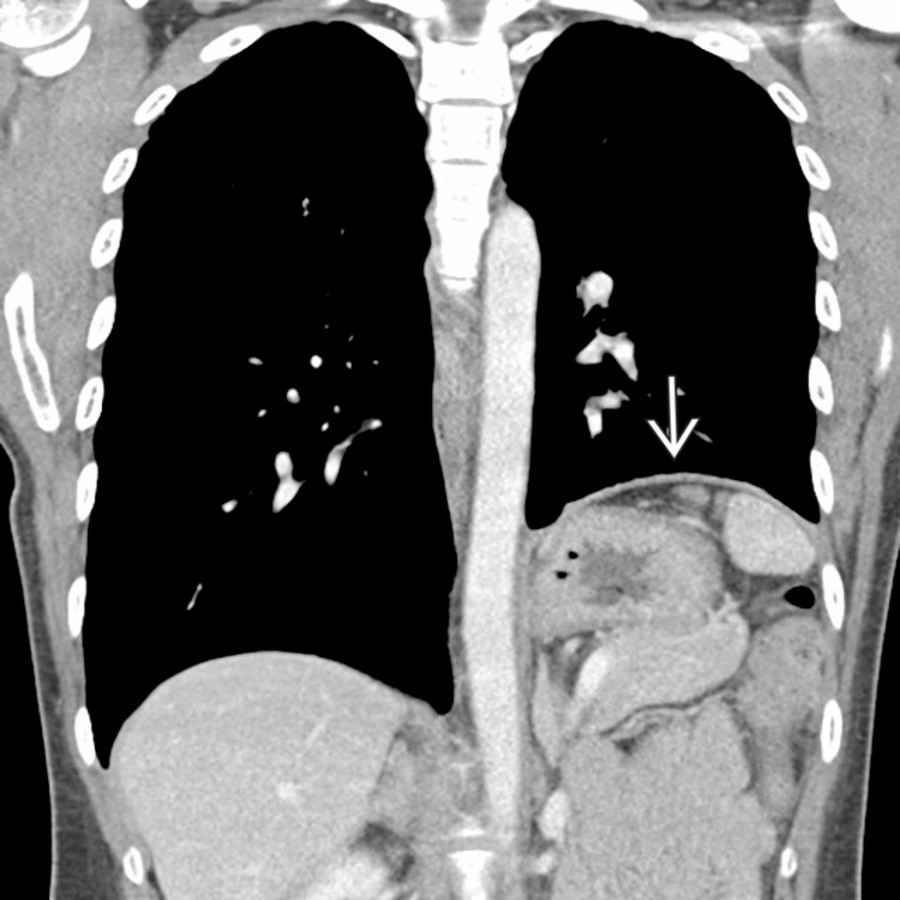
**Paralyzed Diaphragm**
*Coronal CECT shows marked asymmetric elevation of the left hemidiaphragm. In this case, the left diaphragm is paralyzed due to phrenic nerve involvement by the patient's mediastinal lymphoma (not shown).*

**Paralyzed Diaphragm**
*Coronal CECT shows marked asymmetric elevation of the left hemidiaphragm. In this case, the left diaphragm is paralyzed due to phrenic nerve involvement by the patient's mediastinal lymphoma (not shown).*

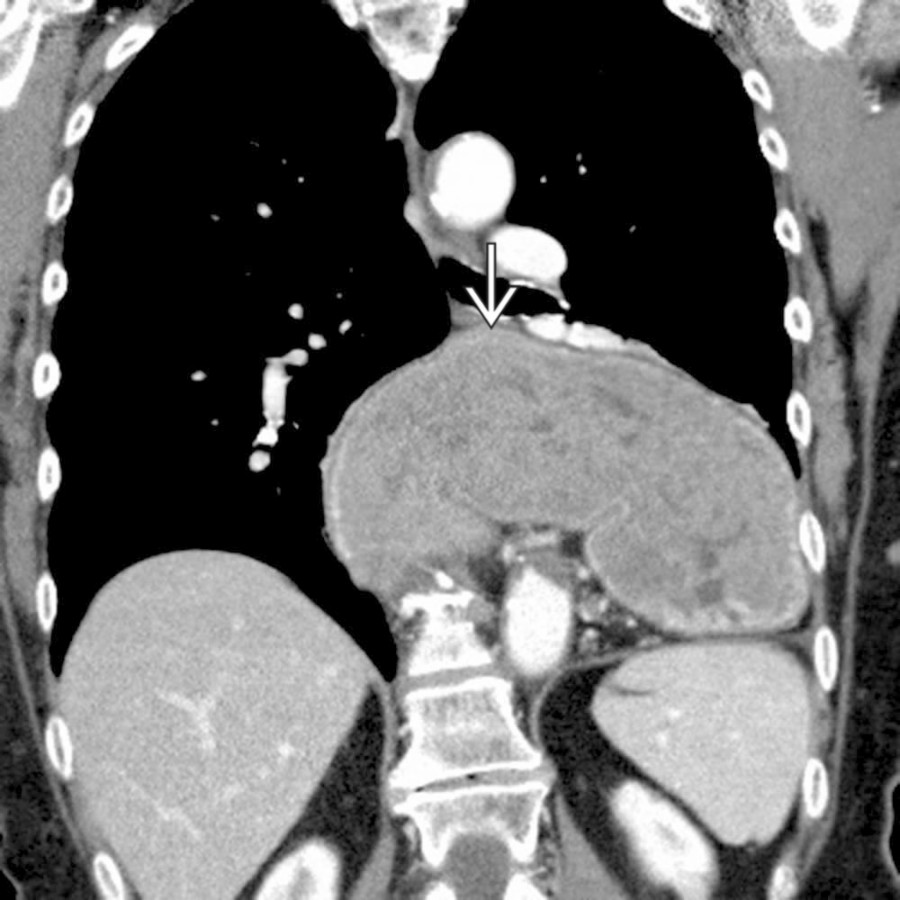
**Eventration of Diaphragm**
*Coronal CECT shows the characteristic appearance of diaphragmatic eventration with focal scalloping of the right anterior hemidiaphragm and superior protrusion of the liver at the site of eventration .*

**Hiatal Hernia**
*Coronal CECT shows a large hiatal hernia with the entirety of the stomach located within the thoracic cavity.*
**Paralyzed Diaphragm**
*Coronal CECT shows marked asymmetric elevation of the left hemidiaphragm. In this case, the left diaphragm is paralyzed due to phrenic nerve involvement by the patient's mediastinal lymphoma (not shown).*

**Paralyzed Diaphragm**
*Coronal CECT shows marked asymmetric elevation of the left hemidiaphragm. In this case, the left diaphragm is paralyzed due to phrenic nerve involvement by the patient's mediastinal lymphoma (not shown).*

**Eventration of Diaphragm**
*Coronal CECT shows the characteristic appearance of diaphragmatic eventration with focal scalloping of the right anterior hemidiaphragm and superior protrusion of the liver at the site of eventration .*

**Hiatal Hernia**
*Coronal CECT shows a large hiatal hernia with the entirety of the stomach located within the thoracic cavity.*
 with herniation of the kidney into the thorax.](images/app.statdx.com_image_thumbnail_facbda67-44b9-4fc9-b95f-797ab6e4d7d4_annotated_true_size_900_quality_90_d53e433decf1c199ee1ff0cadde4370dfcaf6062.jpg)
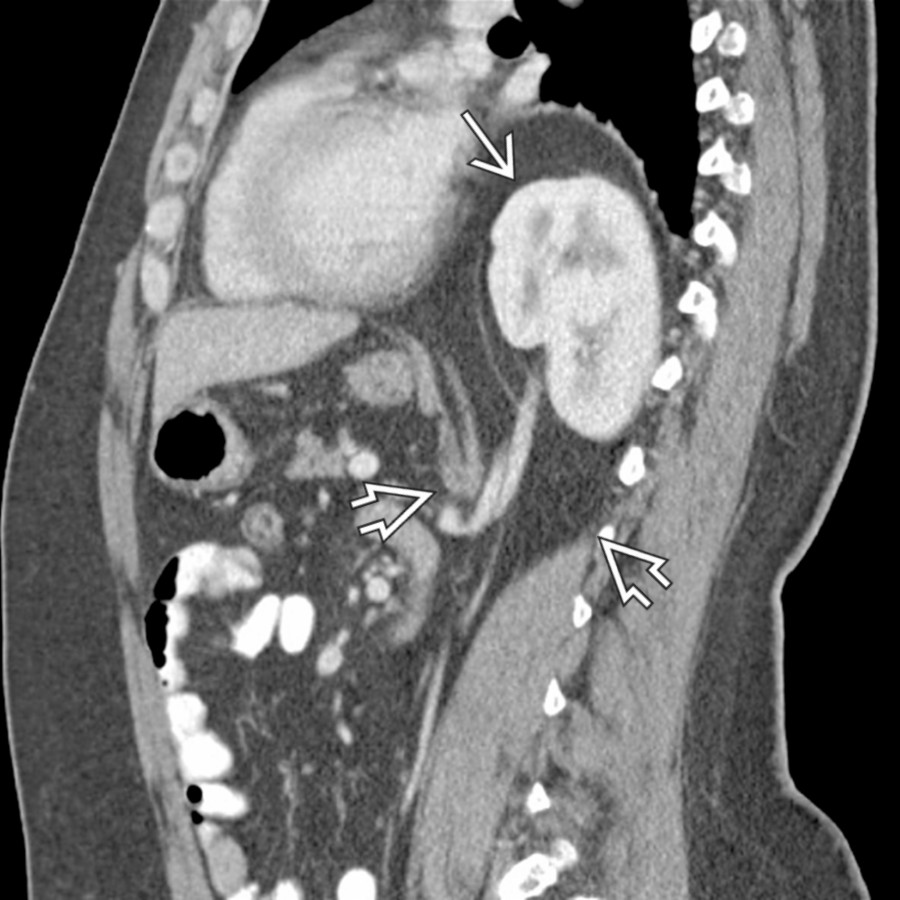
**Bochdalek Hernia**
*Sagittal CECT shows a large Bochdalek hernia containing bowel and kidney. There is focal interruption of the hemidiaphragm with herniation of the kidney into the thorax.*

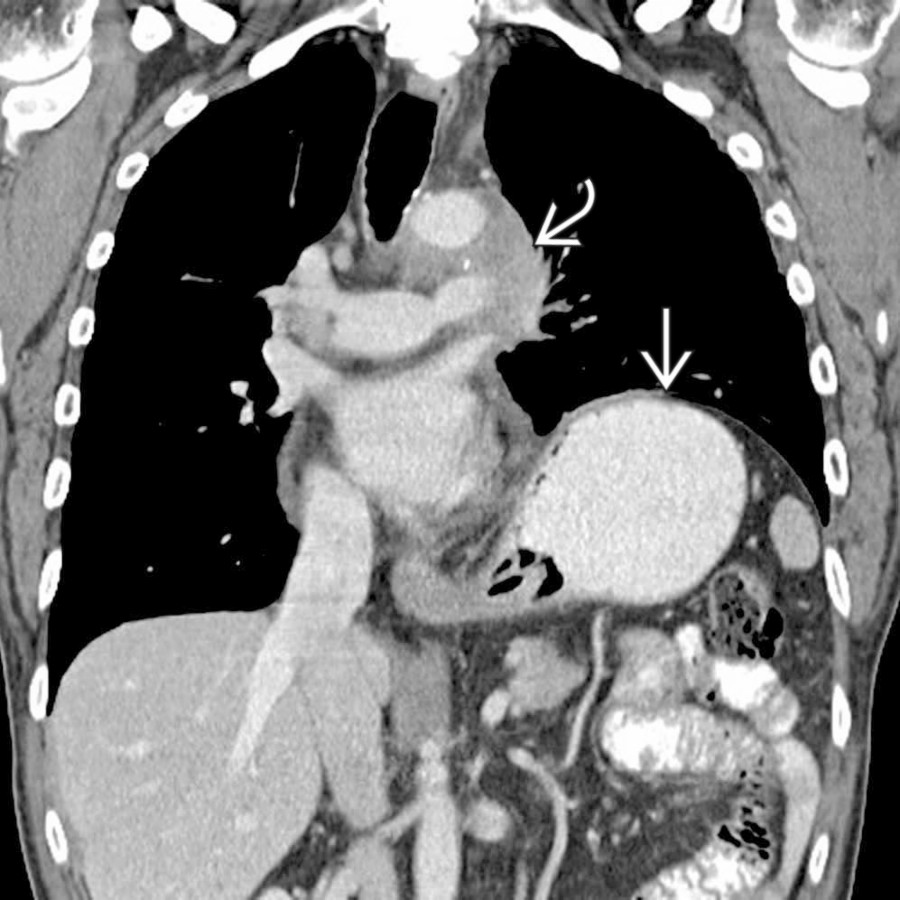
**Morgagni Hernia**
*Coronal NECT shows a characteristic Morgagni hernia with omental fat herniating into the chest through a defect in the right anteromedial diaphragm.*

**Traumatic Diaphragmatic Hernia**
*Sagittal T2 MR shows a posttraumatic defect in the left hemidiaphragm with the stomach herniating into the chest. Note that the diaphragm is identified as a low-signal curvilinear structure. The stomach is pinched as it traverses the defect in the diaphragm.*

**Traumatic Diaphragmatic Hernia**
*Axial CECT shows the fallen viscus sign associated with traumatic diaphragmatic injury. Note that the stomach lies in the chest and has fallen medially and posteriorly to lie against the lung and the posteromedial chest wall.*
**Bochdalek Hernia**
*Sagittal CECT shows a large Bochdalek hernia containing bowel and kidney. There is focal interruption of the hemidiaphragm with herniation of the kidney into the thorax.*

**Morgagni Hernia**
*Coronal NECT shows a characteristic Morgagni hernia with omental fat herniating into the chest through a defect in the right anteromedial diaphragm.*

**Traumatic Diaphragmatic Hernia**
*Sagittal T2 MR shows a posttraumatic defect in the left hemidiaphragm with the stomach herniating into the chest. Note that the diaphragm is identified as a low-signal curvilinear structure. The stomach is pinched as it traverses the defect in the diaphragm.*

**Traumatic Diaphragmatic Hernia**
*Axial CECT shows the fallen viscus sign associated with traumatic diaphragmatic injury. Note that the stomach lies in the chest and has fallen medially and posteriorly to lie against the lung and the posteromedial chest wall.*
 . Ascites lies medial to the diaphragm and adjacent to the cirrhotic liver.](dd9502d7-28db-4747-bd80-f80848a40af6)
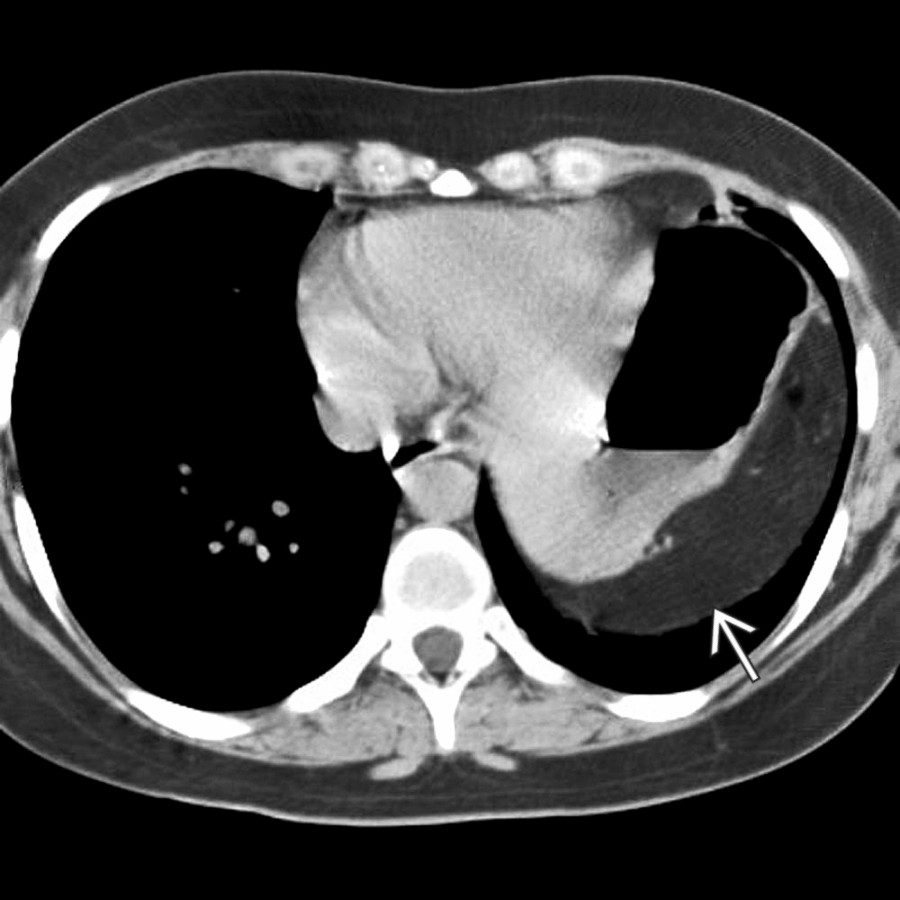
**Subpulmonic Pleural Effusion (Mimic)**
*Axial CECT shows a pleural effusion below the lung and lateral to the diaphragm . Ascites lies medial to the diaphragm and adjacent to the cirrhotic liver.*
### Additional Images
**Paralyzed Diaphragm**
*Axial NECT shows elevation of the left hemidiaphragm without focal bulge or eventration. The abdominal contents do not fall dependently but are suspended by the intact diaphragm.*

**Eventration of Diaphragm**
*Sagittal CECT shows a focal bulge of the liver through a weakened eventration of the right hemidiaphragm.*
**Hiatal Hernia**
*Axial NECT shows herniation of most of the stomach as well as the splenic flexure of colon through a massive hiatal hernia.*

**Bochdalek Hernia**
*Axial CECT shows bilateral defects in the posteromedial portions of the diaphragm with herniation of omental fat.*

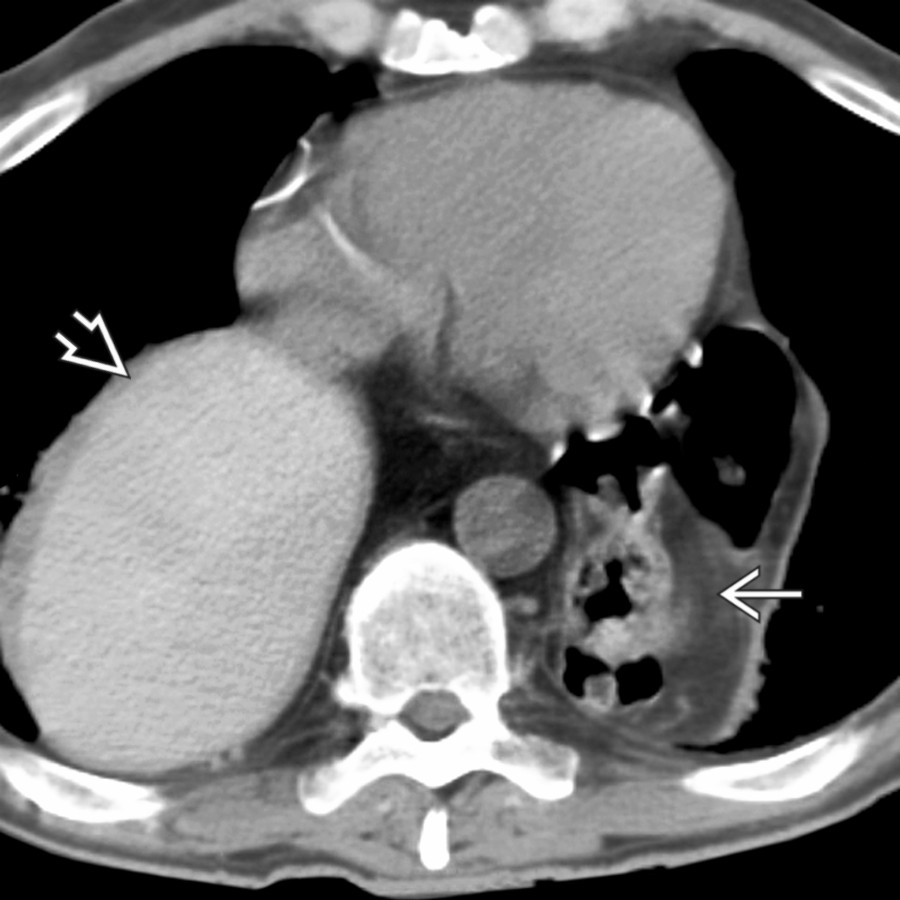
**Morgagni Hernia**
*Axial NECT shows a large hiatal hernia that contains much of the stomach. There is also a large Morgagni hernia , lateral to and displacing the heart, containing omental fat and colon.*

**Traumatic Diaphragmatic Hernia**
*Coronal T2 MR shows herniation of the stomach and omental fat through a defect in the left hemidiaphragm . The stomach is pinched as it traverses the defect in the diaphragm.*

**Traumatic Diaphragmatic Hernia**
*Axial CECT shows herniation of the stomach through a defect in the left hemidiaphragm. The stomach has fallen to lie against the posteromedial chest wall and is pinched .*
**Hiatal Hernia**
*Coronal CECT shows a large hiatal hernia with the entirety of the stomach located within the thoracic cavity.*
**Paralyzed Diaphragm**
*Coronal CECT shows marked asymmetric elevation of the left hemidiaphragm. In this case, the left diaphragm is paralyzed as a result of phrenic nerve involvement by a mediastinal soft tissue mass in this patient with metastatic lung cancer.*

**Bochdalek Hernia**
*Sagittal CECT shows a large Bochdalek hernia containing bowel and kidney. There is focal interruption of the hemidiaphragm with herniation of the kidney into the thorax.*
. Ascites lies medial to the diaphragm and adjacent to the cirrhotic liver.](dd9502d7-28db-4747-bd80-f80848a40af6)
**Subpulmonic Pleural Effusion (Mimic)**
*Axial CECT shows a pleural effusion below the lung and lateral to the diaphragm . Ascites lies medial to the diaphragm and adjacent to the cirrhotic liver.*
### Additional Images

**Paralyzed Diaphragm**
*Axial NECT shows elevation of the left hemidiaphragm without focal bulge or eventration. The abdominal contents do not fall dependently but are suspended by the intact diaphragm.*

**Eventration of Diaphragm**
*Sagittal CECT shows a focal bulge of the liver through a weakened eventration of the right hemidiaphragm.*

**Hiatal Hernia**
*Axial NECT shows herniation of most of the stomach as well as the splenic flexure of colon through a massive hiatal hernia.*

**Bochdalek Hernia**
*Axial CECT shows bilateral defects in the posteromedial portions of the diaphragm with herniation of omental fat.*

**Morgagni Hernia**
*Axial NECT shows a large hiatal hernia that contains much of the stomach. There is also a large Morgagni hernia , lateral to and displacing the heart, containing omental fat and colon.*

**Traumatic Diaphragmatic Hernia**
*Coronal T2 MR shows herniation of the stomach and omental fat through a defect in the left hemidiaphragm . The stomach is pinched as it traverses the defect in the diaphragm.*

**Traumatic Diaphragmatic Hernia**
*Axial CECT shows herniation of the stomach through a defect in the left hemidiaphragm. The stomach has fallen to lie against the posteromedial chest wall and is pinched .*

**Hiatal Hernia**
*Coronal CECT shows a large hiatal hernia with the entirety of the stomach located within the thoracic cavity.*

**Paralyzed Diaphragm**
*Coronal CECT shows marked asymmetric elevation of the left hemidiaphragm. In this case, the left diaphragm is paralyzed as a result of phrenic nerve involvement by a mediastinal soft tissue mass in this patient with metastatic lung cancer.*

**Bochdalek Hernia**
*Sagittal CECT shows a large Bochdalek hernia containing bowel and kidney. There is focal interruption of the hemidiaphragm with herniation of the kidney into the thorax.*